This study attempts to validate the use of the Geriatric Fever Score to predict 30 day mortality in patients over age 65 presenting to an emergency department with fever.
The Geriatric Fever Score uses: leukocytosis, severe coma, and thrombocytopenia. One point is award for each abnormality.
Not surprisingly, mortality went up with the higher the score (33%, 42% and 57% for 0,1,2 points)
For me, I’m not discharging anyone with severe coma, leukocytosis or thrombocytopenia in this patient population therefore I’m not sure this scale has much utility for the practicing emergency physician.
This study looked at the success rates of femoral vs proximal tibial IOs in the prehospital setting. Over a 9 year period, there were 163 pediatric patients who received either a tibial or femoral IO. Femoral IOs were introduced into the EMS protocol in this study area in 2015 as a location option and were the recommended site starting in 2019. The success rate of femoral IO placement was 89% and for proximal tibial sites was 84.7%. After further data analysis the study found an adjusted odds ratio of 2 for successful IO placement in the distal femur compared to the proximal tibia. The complication rates for both sites were similar.
Bottom line: This study suggests that the distal femur is a reasonable site for IO access in the pediatric population.
The use of seizure prophylaxes in moderate to severe head injury has been recommended for 7 days post-injury. In general, levetiracetam is used for seizure prophylaxes in this group of patients. This study looked retrospectively at high (over 500 mg BID) vs. low (500 mg bid) dosing and found there was no difference in seizure events in either group. Overall 6% of patients had a seizure in this seven day window even with medication given.
This study looks at the efficacy of ketamine vs. midazolam for the prehospital sedation of acutely agitated patients, examining the need for repeat sedation (by EMS or in the ED), adverse events and length of stay.
A greater number of patients required repeat sedation within 90 minutes with initial ketamine dosing compared to midazolam. There was no difference in patients receiving repeat sedation within 20 minutes between the two groups.
There were no significant differences in time to repeat sedation, total sedation doses (by EMS or in the ED), use of bag valve mask ventilation or intubation, use of physical restraints, admission location/level of care, or length of stay in the Emergency Department (ED), hospital, or Intensive Care Unit.
I wanted to send out two websites curated in part by UMEM current and past faculty/residents/fellows which have a wealth of critical care lectures and resources:
Disclosure: *I am one of the webmasters for the STCMTCC, but have no affiliation with MCCP other than as an enthusiastic reader.
The benefits of calcium treatment for hyperkalemia have historically been attributed to “membrane stabilization,” as it has been hypothesized to restore cardiac resting membrane potential. However, the true mechanism by which calcium improves cardiac function in this setting remains unclear. This has led to inconsistencies in the clinical threshold for treating hyperkalemia with calcium.
Piktel et al. recently conducted an experimental study investigating the adverse electrophysiologic effects of hyperkalemia and therapeutic effects of calcium treatment in isolated canine myocytes using ex vivo tissue and in vivo cellular techniques.
Key study findings:
Effects of hyperkalemia:
Effects of calcium treatment in the setting of hyperkalemia:
Limitation:
Bottom line: Findings of this study suggest that calcium's beneficial effects in hyperkalemia are not attributed to “membrane stabilization,” but rather to restoration of conduction velocity through L-type calcium channels and subsequent narrowing of the QRS complex. This supports calcium treatment in hyperkalemia when the ECG shows conduction slowing and QRS widening.
Airway management in the pre-hospital setting is a matter of much controversy, and overall I will defer to my EMS colleagues, but several previous studies have failed to show a benefit to endotracheal intubation in the field as opposed to alternate approaches like a supraglottic airway. Another nod in this direction has recently come out, with Battaglini et al performing a post-hoc analysis of one of the larger studies in the history of cardiac arrest, TTM-2, looking specifically at outcomes stratified by pre-hospital airway management strategy.
Do patients who undergo endotracheal intubation in the field do better than those who get a supraglottic airway?
No, they don't. TTM-2 included 1900 patients, of whom 1702 had enough data to be included in this re-analysis. 28% got supraglottic airways, and 72% got endotracheal intubation. The groups were reasonably well matched on most characteristics, and if anything most well-known prognostic factors favored the endotracheal intubation group (very slightly). It should be noted that several outcome metrics, including modified Rankin scale, did show slight signs of benefit for the endotracheal intubation group, even sometimes in a statistically significant fashion, but fell out when a multi-regression analysis, which was the primary endpoint, was done.
Bottom Line: In pre-hospital cardiac arrest, there remains limited data to support the notion that endotracheal intubation results in better outcomes than supraglottic airway placement. You should defer to your local protocols and continue to work with your paramedics and EMS directors as evidence continues to evolve. For now, I don't think there's sufficient data to suggest that a given patient should be intubated vs undergoing supraglottic airway placement, and it is probably best to defer to the judgement, training, and protocols of your folks on scene.
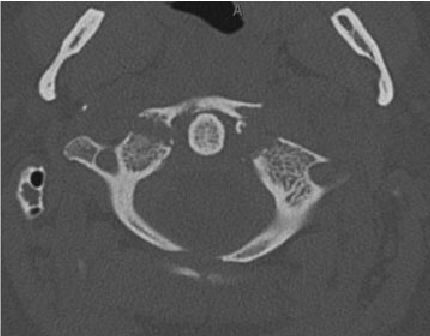
Predicting which blunt abdominal trauma patients have mesenteric or bowel wall injuries early in their ED course will decrease morbidity and mortality. It is also a challenge even in the age of advanced CT imaging. This study from India looks at the Bowel Injury Prediction Score as a possible means to catch these injuries early in the course of care. The score uses white blood cell count over 17,000 (1 point), abdominal tenderness at the time of presentation(1 point), as well as a McNutt's scoring scale grade 4 (1 point) (table). The study found those with a score greater than 2 (out of 0-3) were much more likely to have bowel or mesenteric injury at time of laparotomy. Tenderness and CT findings were more likely to be predictive of bowel injury than WBC greater than 17,000. “BIPS had 94.5% sensitivity, 72% specificity, 88% PPV, and 86% NPV for identifying patients with sBBMI.”
My take away is an abnormal CT scan or significant tenderness of presentation warrant concern for mesenteric or bowel wall injury and surgical evaluation is appropriate for these patients. An elevated or normal white blood cell count isn't helpful in these patients. Surgeons may use this scale to help them decide if a patient warrants a trip to the operating room
| GRADE | FINDING |
|---|---|
| 1 | Isolated mesenteric contusion without associated bowel wall thickening or adjacent interloop fluid collection |
| 2 | Mesenteric hematoma?<?5 cm without associated bowel wall thickening or adjacent interloop fluid collection |
| 3 | Mesenteric hematoma?>?5 cm without associated bowel wall thickening or adjacent interloop fluid collection |
| 4 | Mesenteric contusion or hematoma (any size) with associated bowel wall thickening or adjacent interloop fluid collection |
| 5 | Active vascular or oral contrast extravasation bowel transaction or pneumoperitoneum |
This review reminds us that discharging emergency department patients with abnormal vital signs is a risk for the patient and the provider. The more abnormal vital signs that are present, the higher the risk of adverse event and subsequent return to the emergency department.
“Hypotension at discharge was associated with the highest odds of adverse events after discharge. Tachycardia was also a key predictor of adverse events after discharge and may be easily missed by ED clinicians.”
Always address abnormal vital signs in your medical decision making portion of the chart and be very wary of discharging anyone with tachycardia or other abnormal vital signs.
Continuing with the electrolyte derangements in children: Hyponatremia
Hyponatremia is defined as a Sodium of less than 135 mmol/L and does not depend on patient age.
This is the most common electrolyte abnormality in pediatric patients. Excessive free water is often the culprit and is usually thought of in the neonate or infant whose guardians are mixing formula incorrectly. * Additional causes include inappropriate ADH (Antidiuretic hormone) secretion, or in the case of dehydrated patients appropriate ADH secretion. Sodium wasting is rare.
Total body water (TBW) is important to consider, and preterm neonates have higher TBW (80%) than full term (70%) and 1 year old infants (~60%) putting them at higher risk of hyponatremia.
Recognizing the volume status of the patient aids in determining the etiology of the hyponatremia and allows for appropriate treatment. This may require obtaining urine sodium.
Treatment:
Hypertonic saline should be used only for patients with severe neurologic complications including seizures or altered mentation. In these patients, a hypertonic saline bolus should be given at 3-5 ml/kg of 3% NaCl over 10-15 minutes.
In hypovolemic patients without neurologic symptoms, fluid resuscitation is the mainstay with caution to increase sodium levels by no more than 6-8mmol/L/day. For euvolemic or hypervolemic patients, fluid restriction is advised.
Prevention:
Importantly, when children receive IV fluids, the choice should be made to select isotonic fluids (0.9% NaCl) rather than hypotonic fluids (0.45% NaCl) to avoid iatrogenic development of hyponatremia.
*Reminder: 2 ounces (about 60 ml) of water should be placed in the bottle, and then 1 full scoop of formula, unless directed to have higher caloric content by their doctor- in which case the amount of formula in the mixture should be higher
Mycoplasma genitalium (M.genitalium, or Mgen) is a pathogen that is increasingly associated with cervicitis, pelvic inflammatory disease, preterm labor, spontaneous abortion, and infertility. Although many are asymptomatic, M.genitalium can be found in 10-30% of women with symptoms/exam findings of cervicitis.
NAAT testing for M.genitalium is FDA-approved for use with urine and urethral, penile meatal, endocervical, and vaginal swab samples.
According to CDC guidelines, women with recurrent or persistent cervicitis should be tested for M.genitalium, and testing should be considered among women with PID. It is not recommended to test for asymptomatic infections at this time, even in pregnancy.
High rates of macrolide resistance in this pathogen make 1 g of Azithromycin insufficient. The recommended regimen for NAAT-positive M.genitalium infections is: Doxycycline 100 mg PO BID x 7 days to reduce bacterial load, followed by moxifloxacin 400 mg PO daily x 7 days.
Overall, more studies are needed to truly determine the clinical relevance of this pathogen.
Consider testing for M.genitalium in patients presenting with recurrent or persistent cervicitis or pelvic inflammatory disease, as this may not respond to typical antibiotic regimens.
The incidence of opioid-overdose-related deaths has clearly increased in the past decade, with recent estimates of up to 17% of OHCA being opioid-related in 2023. [1,2] The use of naloxone for opiate reversal in overdose is well-established, with reasonable inference but no formal proof that its use could help in opioid-associated out of hospital cardiac arrest (OA-OHCA). [3] The August publication of two trials [4,5] retrospectively examining naloxone administration in OHCA offers some perspectives…
and
[View “Visual Diagnosis” for slightly more detail on the referenced studies.]
Bottom Line: While prospective trials are absolutely needed to offer more definitive evidence regarding the use of empiric naloxone in nontraumatic OHCA, the rising incidence of OA-OHCA in the U.S. and current findings are convincing enough to encourage early naloxone administration, especially in populations with higher incidence of opioid use.
U.S. Mortality due to Opioid Overdose (CDC data)
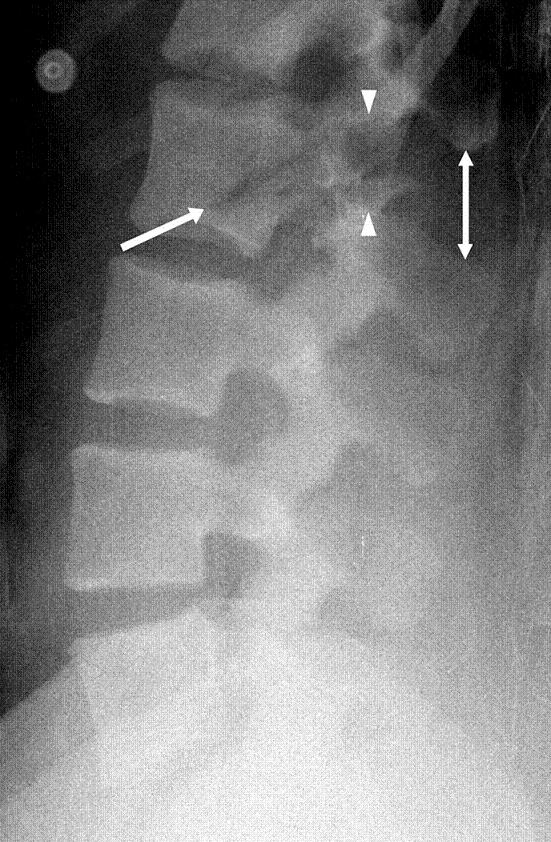
In this systemic literature review of orthopedic injuries identified in intimate partner violence (IPV) the authors remind us that finger, hand, and especially isolated ulnar fractures are very commonly associated with IPV. When we see these injury patterns extra effort is required to determine if IPV is involved.
| Citation | **Bhandari et al.**3 | **Khurana et al.**18 | **Loder et al.**12 | **Porter et al.**13 | **Kavak et al.**7 | **Thomas et al.**17 |
|---|---|---|---|---|---|---|
| Division of injury locations | Fingers, wrist, shoulder dislocation, humerus fracture | Finger, hand, wrist, forearm, elbow, humerus, shoulder | Finger, hand, wrist, forearm, elbow, humerus, shoulder | Radius/ulna, humerus, upper extremity, right/left | Phalanx, radius, ulna (diaphysis/metaphysis, distal/proximal) | Phalanges (distal/medial/proximal), hand/finger, forearm, arm/shoulder right/left |
| Most common UEF location | Fingers (n = 11) | Finger (34.3%) | Finger (9.9%) | Radius and ulna (n = 80; 5.9%) | Ulna (14.5%) | Finger (46%) |
| Most common injury type‡ | Musculoskeletal sprains (all n = 21; 28% back n = 7; neck n = 6) | UEF (27.2%) | Contusions/abrasion (43.4%) | Rib fracture (17.5%) | Soft-tissue lesions (n = 1,007, 82.2%) | UEF (52%) |
* IPV = intimate partner violence, UEF = upper extremity fracture, and UEI = upper extremity injury.
† Summary table demonstrating the location prevalence of UEIs caused by cases of IPV. Fractures were quantified separately from other UEIs in this specific table.
‡ In all included articles the most common injury type was an injury to the head or neck; these are excluded because of the study aim.
Autism Spectrum Disorder (ASD) can often be a diagnosis that complicates usual ED evaluation and management. One of the frequently asked questions is “what medications work well for patients with autism?” It is often said, although with quite variable evidence in the literature, that benzodiazepines should be avoided in patients with ASD due to the risk of paradoxical reaction.
This study was a meta-analysis that included 20 different studies that looked at efficacy and adverse effect of various medications and medication combinations for procedural sedation for a variety of painful and nonpainful procedures. Although the heterogeneity of the indications, medications, and other details of study design of the studies included precludes a definitive recommendation as to the best medication or regimen, it does suggest overall reasonable efficacy of midazolam both as a single agent as well as in combination with dexmedetomidine, especially when balanced against adverse effects noted with some of the more efficacious regimens.
Take Home Point: Medication choice for patients with ASD should be individualized to the patient based on prior experiences, parental or patient input, and prescriber experience given proven efficacy of multiple regimens. Benzodiazepines should be considered within the toolkit.
This retrospective study of Swiss trauma patients looked at blood gas oxygen levels within 3 hours of arrival to the trauma bay in severely injured patients over age 16. When comparing hypoxic, hyperoxic and normo-oxic patients there was no difference in 28 day mortality. Those with above normal oxygen levels tended toward longer hospital stays. The above normal oxygen cohort also were more likely to be intubated in the field.
This study fits with others showing around 20% of trauma patients arrive to our trauma bays over oxygenated. More research is needed to see the impact this has on care. Be mindful of over oxygenation especially in intubated trauma patients.
Traditional Medicare now covers < 50% of Medicare beneficiaries. It reimburses on a fee-for-service basis. For beneficiaries, it includes deductibles and coinsurance requirements that yield average annual out-of-pocket expenses measured in the thousands of dollars.
Medicare Advantage, the new alternative, has grown quickly. Plans typically promise beneficiaries fewer co-pays and more services. It relies on private insurers (think United, Blue Cross, Kaiser Permanente) to coordinate care and rein in costs. Subsidies to Medicare Advantage have helped spur growth, subsidies that mean costs per beneficiary for Medicare Advantage exceed those for traditional Medicare.
Which means Medicare still needs to figure out how to save money and remain viable while the US population over 65 grows.
When listening to a lecture about Medicare or reading a study that uses Medicare data, take a moment to ask “Which Medicare? Fee-for-service? Or Advantage?”
For a take on the future of Medicare, see McWilliams JM, The Future of Medicare and the Role of Traditional Medicare as Competitor, NEJM, August 22/29, 763-769.
To understand why Medicare Advantage plans are popular, see https://www.kff.org/medicare/issue-brief/10-reasons-why-medicare-advantage-enrollment-is-growing-and-why-it-matters/.
Hepatorenal Syndrome
We see patients with nausea, fatigue, altered mental status, and other vague symptoms all day, every day in the ED. Let's not forget about hypercalcemia in the differential, especially in patients with a known malignancy! Many tumor types secrete a Parathyroid hormone (PTH)- related protein that mimics PTH and leads to high calcium levels.
Here are some clinical pearls on hypercalcemia of malignancy: