I don't know about you, but I'm always eager to hear new and alternative methods of pain control…
This study examined the effectiveness of transcutaneous electrical nerve stilumlation (TENS) in patients with abdominal pain. Patients were randomized to TENS or sham applied to the abdomen. The primary outcome of interest was change in pain score 30 min after the intervention, and secondary outcome was percentage of patients requiring rescue analgesia. Pain scores were measured on a verbal numeric score scale with a range from 0 to 10, with any adult patients with a minimum score of 5 being eligible.
The mean reductions in pain scores after the intervention were also similar in patients treated with TENS and sham TENS (1.9 vs. 1.7 respectively, p = 0.81). THe use of rescue analgesia was 49% in patients treated with TENS and 51% in those who received sham TENS (p=0.66). No adverse events were noted.
The authors did note that there is a challenge in blinding due to toeh absence of electrical stimulation in the sham group; nonetheless, TENS was not found to be more effective than sham. It also did not reduce the need to rescue analgesia.
Guess I'll keep looking…
This May, the Society of Critical Care Medicine (SCCM) published new recommendations [1] for the use of corticosteroids in critical illness (separate from patients with known adrenal insufficiency or on chronic steroids), namely:
Bottom Line:
For severe bacterial pneumonia and septic shock, ED physicians should feel comfortable administering a dose of hydrocortisone 50mg IV as hydrocortisone 200mg/day is an accepted regimen for these disease processes.
For patients with ARDS who remain boarding in the ED, EM docs should discuss initiation of steroids with their intensivists, whether the institutional preference is for dexamethasone 20mg IV (per DEXA-ARDS) [6] or methylprednisolone 1mg/kg/day (per Meduri)[7].
POCUS has been shown to have a 92.4% sensitive (95% CI 89.0% to 94.7%) and 96.6% specific for identifying SBO.
Some characteristics of SBO include:
-dilated fluid filled bowel
-contents of bowel moving to and fro like a washer machine
-wall thickening and ability to see plicae circulares
- in high grade obstruction you may also notice intraperitoneal fluid near the dilated bowel.
Patient struck in left eye. The patient was asked to look up during exam and this is the finding. What imaging modality would you order if so inclined, what is the injury, and what is the disposition/plan?

Hypokalemia is a common electrolyte abnormality found in pediatric patients. The cut off for low potassium is based on age, with young infants having higher baseline levels of potassium when compared to older children and adults. The most common cause of hypokalemia in children is GI losses (diarrhea), though other considerations include malnutrition, congenital adrenal hyperplasia, renal abnormalities and medication effects.
Typically, hypokalemia is well tolerated, and the focus of management is based on treating the underlying cause, rather than repleting the potassium.
Medications should ONLY be initiated in patients who have potassium levels < 3.0 mmol/L OR with those with levels < 3.5 mmol/L with ECG changes.
In patients receiving treatment, oral potassium administration is typically recommended unless any of the following criteria are met:
In these patients IV potassium should be given (typically KCl at 0.5-1mEq/kg/DOSE - Max of 40 mEq/dose).
Just like in adults, ALL patients require continuous cardiac monitoring when receiving potassium infusions.
Spontaneous coronary artery dissection (SCAD) occurs when there is an intimal tear that develops within the wall of an epicardial coronary artery, leading to intramural hematoma and false lumen formation with compromised coronary blood flow. This tear develops in the absence of atherosclerosis, trauma, or iatrogenic injury. SCAD is believed to account for 4% of acute coronary syndromes, and has been found to be the cause of ACS in 35% of women under the age of 50. Women comprise the majority of cases of SCAD( 87-95%).
Patients with Pregnancy-associated SCAD (P-SCAD) will often present with higher-risk features and more severe presentations compared with non-pregnancy related SCAD. They are more likely to present with STEMI (>>NSTEMI), impaired left ventricular function, left main and multivessel disease, and shock than other cohorts of SCAD patients.
The peak timing of P-SCAD is within the first month postpartum (with the highest incidence within the first week), although cases can occur throughout all trimesters of pregnancy or many months postpartum.
Keep SCAD in your differential for patients without typical risk factors who present with signs/symptoms of ACS. A strong index of suspicion is necessary to prevent bad outcomes and improve morbidity and mortality from this disease entity.
Noninvasive Ventilation for Preoxygenation
192 trauma patients who were receiving pre-hospital fentanyl for moderate to severe pain were randomized to placebo or intranasal 50 mg ketamine as an adjunct for pain control. There was no difference between the two groups in decrease in pain scale.
The authors concluded: “In our sample, we did not detect an analgesic benefit of adding 50 mg intranasal ketamine to fentanyl in out-of-hospital trauma patients.”
Needed for sample size determination
Power – (1-beta), where beta is the risk of a type 2 error – rejecting the accepting the null hypothesis when it is true – this is usually selected to be 0.8 or 0.9.
Significance (alpha), the chance of making a type 1 error – accepting the alternate hypothesis when the null hypothesis is true. This is usually selected to be 0.05.
One-tailed or two-tailed – is the null hypothesis one of no difference (experimental arm not better or worse) or one-sided (experimental arm not better)?
Effect Size. This is the challenging part. This is the size of the difference in outcomes you’re looking for.
For continuous outcomes (example – difference in pain scores). You’ll need an estimate for the variation in the scores between presentations, or the standard deviation. You can get this from a literature estimate or a from small local measurement, say of 10 patients or so.
For a dichotomous outcome (example – percentage of successes), you can usually estimate the percentage in one group and choose the difference you are looking for.
The effect size has a big effect on the sample size. Generally, cutting the effect size in half increases the sample size by fourfold.
Statistical software - next pearl.
Prioritizing the timely admission of older patients from the emergency department (ED) to appropriate wards is essential to reduce adverse events, such as falls and infections, and to decrease the duration of hospital stays. Recent cohort studies, both observational and prospective, have demonstrated that elderly patients who experienced prolonged or overnight stays in the ED had a higher in-hospital mortality rate compared to those who were admitted earlier to inpatient care. Efficient patient flow and early admission from the ED to appropriate wards are crucial strategies for improving survival rates and reducing morbidity among older patients.
The systematic review of presyncope literature found that presyncope should be treated the same as syncope in terms of work up and disposition.
“In conclusion, the prevalence of short-term serious outcomes among ED patients with presyncope ranges from one in four to one in 20, with arrhythmia being the most common serious outcome. Our review indicates that presyncope may carry a similar risk to syncope, and hence, the same level of caution should be exercised for ED presyncope management as that of ED syncope.”
“Administrative harm” (defined as “the adverse consequences of administrative decisions within health care”) is a relatively new term for challenges that arise in complex health care work environments.
41 mostly hospitalists participating in interviews and focus groups found that the concept resonated, and that administrative harms could arise at all levels of leadership, negatively impacted both workforce and patients, were challenging to measure, and pointed to a lack of leadership responsibility and accountability. The group also suggested many approaches and solutions for prevention.
The article is here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2820266. If interested, take a look at the thematic tables 2 and 3.
There is a brief editorial comment here, https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/2820275.
Background: Sepsis remains a common entity associated with a relatively high rate of inpatient mortality, with timely recognition and treatment being key to improving patient outcomes. Various screening and warning scores have been created to attempt to identify sepsis and those patients at high risk of mortality earlier, but have limited performance because of suboptimal sensitivity and specificity.
A prospective observational study compared the performance of a variety of these scores (SIRS, qSOFA, SOFA, MEWS) as well as a machine learning model (MLM) against ED physician gestalt in diagnosing sepsis within the first 15 minutes of ED arrival.
Although not without its limitations, this study highlights the importance and relative accuracy of physician gestalt in recognizing sepsis, with implications for how to develop future screening tools and limit unnecessary exposure to unnecessary fluids and empiric broad spectrum antibiotics.
Bottom Line: In the era of machine learning models and AI, ED physicians are not obsolete. Even at 15 minutes, without lab results and diagnostics, our assessments lead to appropriate diagnoses and care. In this new normal of prolonged wait times and ED boarding, ED triage and evaluation models that optimize early physician assessment are of the utmost importance.
Author:
Gabriella Miller (She/Her)
Clinical Instructor
Department of Emergency Medicine
University of Maryland School of Medicine
Doxycycline PEP for the prevention of bacterial STIs.
The CDC now recommends “doxy PEP” for high-risk individuals. Doxycycline post-exposure prophylaxis (doxy PEP) is a prescription for patients to self-administer 200 mg doxycycline by mouth within 72 hours after anal, oral, or vaginal sex to prevent the transmission of chlamydia, gonorrhea, and syphilis. The CDC defines “high-risk” as men who have sex with men (MSM) and transgender women (TGW) who have been diagnosed with a bacterial STI within the past 12 months. They summarize the findings of the French IPERGAY and ANRS DOXYVAC studies, as well as the US DoxyPEP study, which all show promising reductions in risk ratios or hazard ratios of decreasing bacterial STI transmission on high-risk populations, including those who are taking PrEP for HIV. No significant adverse events related to doxy PEP have been reported.
Conclusion:
Counsel patients at high risk for bacterial STIs regarding the prescription of doxy-PEP for patient self-administration within 72 hours after sex.
Two recommendations from the recent GRACE 4 publication in Academic Emergency Medicine to consider:
1. Use phenobarbital along with benzodiazepines in patients with moderate to severe alcohol withdrawal. The evidence isn’t robust but is positive when compared to benzos alone.
2. Adults with alcohol use disorder can benefit from anti-craving medications such as naloxone and gabapentin at time of discharge.
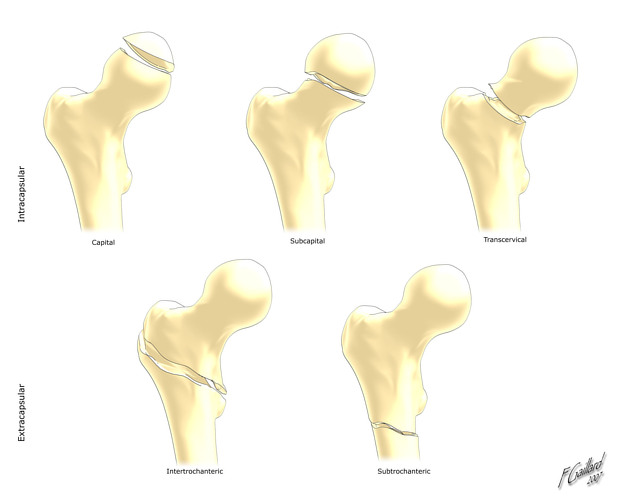
Hip Fractures
Femoral neck and intertrochanteric fractures occur most commonly among patients aged 65 and over
Major risk factors for hip fractures include osteoporosis and falls.
Patients with a low body mass index (BMI <22) appear to be at higher risk
Isolated trochanteric fractures occur more often in young active adults
In-hospital mortality rates are approximately 5% (range 1-10%)
In addition to making the diagnosis and consulting orthopedic surgery, ED providers must remember to provide adequate analgesia as elderly patients are often under medicated.
-Up to 72% receive no prehospital analgesia.
Extracapsular fractures cause more pain than intracapsular fractures due to the greater degree of periosteal trauma.
Poor pain control predisposes hip fracture patients to delirium
Retrospective studies indicate that patients at higher risk for significant bleeding have at least 2 of the following risk factors:
Age over 75 years, initial Hgb below 12 g/dL and peri trochanteric fracture location.
Teaching has circulated that a temperature of 40 degrees Celsius or above (hyperpyrexia), was associated with a greater incidence of serious bacterial infection. However, this teaching originated in a time prior to the availability of childhood vaccinations. In fact, the largest retrospective study to support this used data from 1966-1974.
2565 WELL APPEARING patients between the ages of 61 days and their 18th birthday who presented to a single tertiary care pediatric emergency department with the chief complaint of fever were included. The prevalence of serious bacterial infection was compared to the presence of hyperpyrexia, age, chronic conditions, gender and vaccination status.
Serious bacterial infections (SBIs) included: deep space infections, appendicitis, pneumonia, mastoiditis, lymphadenitis, acute bacterial rhinosinusitis, urinary tract infection, pyelonephritis, cholecystitis, tubo-ovarian abscess, septic arthritis, osteomyelitis, bacteremia or bacterial meningitis.
There was NO statistically significant association between hyperpyrexia and SBIs. Older age and make sex were associated with a higher risk of SBIs.
Bottom line: In well appearing children 61 days and older, having a temperature >/= to 40 degrees was not associated with serious bacterial infections.
A prospective European study of patients over age 65 presenting with a ground level fall obtained troponin levels to ascertain if myocardial infarction was a cause of the ground level fall. Troponin levels were elevated in a majority of patients however only 0.5% were defined as having a myocardial infarction. Of the 3% who died within 1 year, troponin was found to be higher than those that survived the one-year study period. The authors concluded “Our data do not support the opinion that falls may be a common presenting feature of MI. We discourage routine troponin testing in this population. However, hs-cTnT and hs-cTnI were both found to have prognostic properties for mortality prediction up to 1?year.”
Several studies have shown that patients who require a resuscitative thoracotomy (RT) have a higher odds of survival if they are transported by police or in private vehicles. This study examined 195 patients who required RT to see if prehospital intubation and out of hospital time (OOHT) affected ROSC rates.
There was no association between OOHT and ROSC and no association of OOHT and survival. The mean OOHT for this study was only 25 minutes which is faster than other studies.
The odds of ROSC were lower in patients who had ANY intubation attempts prior to arrival.
Bottom line: BLS airway management (or supraglottic placement) may be more beneficial for the trauma arrest patient in the prehospital setting.
-668ade5e780f0.jpg)