Clinical Presentation:
Diagnosis
Treatment
Bottom line:
Chikungunya virus can cause symptoms similar to dengue fever but is not as deadly. This week the first cases of CHIKV were reported in the Caribbean. Consider this in travelers returning from endemic areas.
Distinguishing features:
University of Maryland Section for Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
The Concentrated Overview of Resuscitative Efforts (CORE) Scan
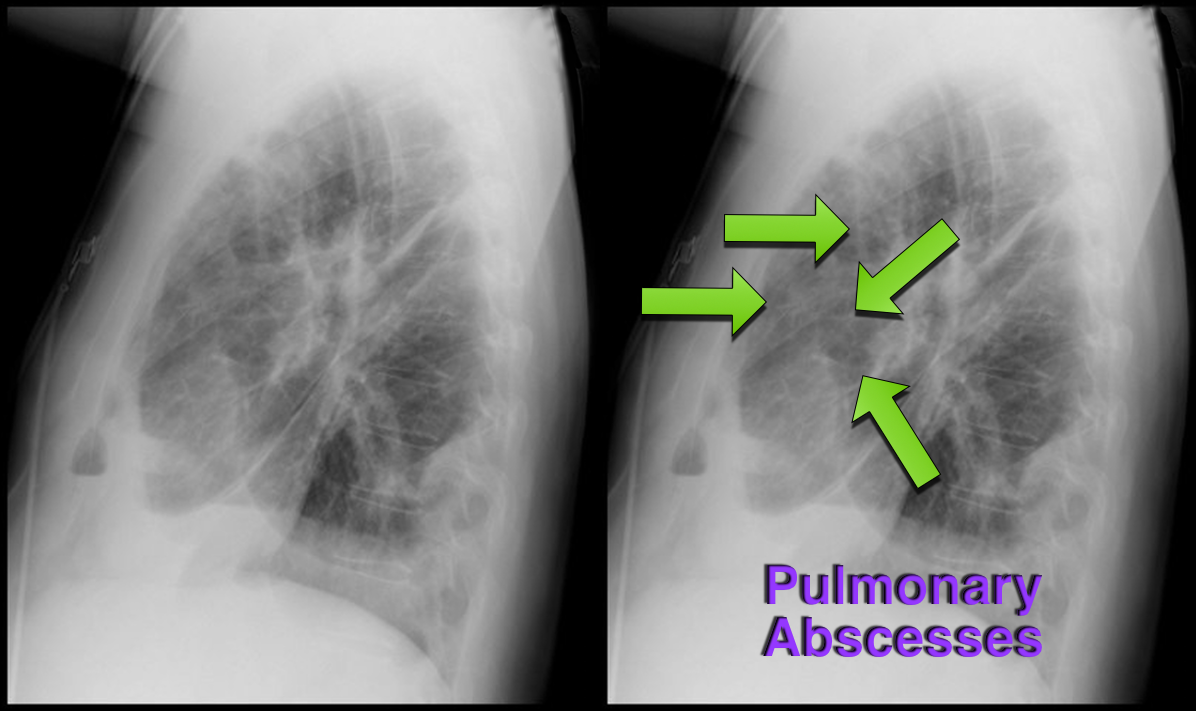
37 year-old male presents with cough and a fever. What's the diagnosis and name three risk factors assiciated with disease?

Bottom-line: The HEART score can help to objectively risk stratify ED patients with chest pain into low, intermediate, and high risk groups. Using the HEART score can also facilitate more efficient and effective communication with colleagues.
Want more emergency cardiology pearls? Follow me @alifarzadmd
In a potentially ground breaking study of healthcare-associated pneumonia (HCAP) patients, atypical pathogens were identified in 10% of cases!
Application to clinical practice: Add atypical coverage with a macrolide or respiratory fluoroquinolone for HCAP patients who have been in the community for any length of time.
The study also identified HCAP patients who may not require 3 'big gun' broad-spectrum antibiotics. This is a practice changing article for ED providers. For more analysis of the study, please note the bonus reading links below.
Bonus reading:
Dr. Emily Heil (@emilylheil) analyzes the full study in more depth at Academic Life in Emergency Medicine: http://academiclifeinem.com/new-treatment-strategy-not-so-sick-health-care-associated-pneumonia/
Dr. Ryan Radecki (@emlitofnote) critiques the study at Emergency Medicine Literature of Note: http://www.emlitofnote.com/2013/10/down-titrating-antibiotics-for-hcap.html
It has linear, predictable pharmacokinetics, achieves maximal concentration within 1-2 hours, is 50% renally excreted, and has a half life is 9-11 hours.
Edoxaban was evaluated in a recent trial comparing warfarin in patients with atrial fibrillation.
The primary end point or first stroke or systemic pulmonary embolic event occurred in 1.5% with warfarin, compared with 1.18% in the high dose edoxaban (HR 0.79; 97.5% CI 0.63-0.99, P<0.001). In the intention to treat there were trends favoring high dose edoxaban and unfavorable trends with the lower dose.
The principal safety end point of major bleeding occurred in 3.43% with warfarin versus 2.75% with high dose edoxaban (HR 0.86; 95% CI 0.71-0.91, P<0.001).
Bottom line: Both high dose (60 mg) and low dose (30 mg) edoxaban were non-inferior to warfarin with prevention of stroke or systemic emboli, and were associated with significantly lower rates of bleeding and death from cardiovascular causes.
Currently it is approved for use in Japan.
General Information:
Fever and headache or rash in those with close contacts from the affected universities should be considered for rapid, empiric meningococcal treatment.
Vent Management: Finding the AutoPEEP!
OK, so we all know not to, "...Fall asleep on Auto-PEEP" thanks to Dr. Mallemat's pearl that can be seen here. But now the question is, how do you know if your patient is air-trapping?
There are 3 ways you can look for evidence of Auto-PEEP on the ventilator:
Which view of the heart is this and can you name the structures from A-G?
ECG Following Cardiac Transplant
Posterior Shoulder Dislocations

(A posterior shoulder dislocation will show the humeral head displayed superiorly in the image away from the clavicle which is the inferior most bone)
Some things to look for on the AP view that will suggest a posterior shoulder dislocation:
Life in the Fast Lane as a great discussion of posterior shoulder dislocations at http://lifeinthefastlane.com/posterior-shoulder-dislocation/
Best way to make the diagnosis --- suspect it and get an axillary view.
Bottom Line: In a stable pediatric abdominal trauma victim, combined FAST and LFT results are an effective screening tool to evaluate for intra-abdominal injury.
The management of alcohol withdrawal syndrome (AWS) includes supportive care focusing on the ABC’s and administration of benzodiazepines (BDZ).
While BDZ are effective in the treatment of AWS, some patients may require very high doses of BDZ to control symptoms (tachycardia, hypertension, diaphoresis, etc.); unfortunately, high-doses of BDZ may lead to suppression of the respiratory drive and endotracheal intubation.
Dexmedetomidine (DEX) is a sedative agent that is an intravenous alpha2-agonist (it's like clonidine); it reduces sympathetic outflow from the central nervous system and it may help treat withdrawal syndromes. The major benefit of DEX is that it does not suppress the respiratory drive, thus intubation is not required.
Smaller trials and case series have shown that patients with AWS who were treated with BDZ in addition to DEX had better symptom control, lower overall BDZ doses, and less respiratory depression/intubation.
Bottom-line: While more trials are needed, consider adding DEX for patients with AWS who require high-doses of BDZ.
What view of the heart is this and can you name everything from A-G?
Want more emergency cardiology pearls? Follow me @alifarzadmd
Unexplained respiratory symptoms during exercise are often incorrectly considered secondary to exercise induced asthma/bronchospasm.
An important diagnosis on the differential should be exercise-induced laryngeal obstruction (EILO).
Of 91 athletes referred for asthma workup, 35% had EILO.
The presence of inspiratory symptoms did not differentiate athletes with and without EILO.
61% of athletes with EILO used regular asthma medication at referral.
Reversal of the new anticoagulants rivaroxaban (Xarelto) and dabigatran (Pradaxa) has been challenging particularly in the ED setting with no definitive reversal agent. Intracerebral hemorrhage or critical GI bleed management becomes challenging and worsens mortality.
There is growing literature that states activated prothrombin complex concentrate or non-activated PCC may reverse these new anticoagulants. A volunteer study (1) showed its efficacy and concensus workgroups are now recommending aPCC as first line therapy(2). The search goes on for a reliable reversal agent for these new anticoagulants which were suppose to solve more problems instead of create new ones.
General Information:
Nisseria meningitidis is the common culprit in epidemic meningitis. Serogroup B is currently causing an outbreak on the Princeton campus. So what are the serogroups and why are they important?
Six main serogroups cause disease: A, B, C, Y, X, W-135.
Two quadrivalent vaccines are currently licensed in the US that cover Serogroups A, C, Y, and W-135.
Relevance to the EM Physician: The currently available vaccines in the US cover the majority of serogroups of meningococcus, however, Serogroup B (currently causing an outbreak at Princeton) is not covered, nor is Serogroup X (for travelers to Sub-Saharan Africa).
Bottom Line: Serogroups B and X are not covered by the currently available vaccines in the US and at risk populations (and physicians treating those patients) should be made aware of the gap in coverage. Investigations for a vaccine for Serogroup B (licensed in Europe and Australia, but not in the US) are currently underway.
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH, FACEP
Ottawa Rules for Subarachnoid Hemmorhage (SAH)
Background
Design
Results
132 (6.2%) had SAH
Decision rule including any:
Had 98.5% sensitivity (95% CI, 94.6%-99.6%) and 27.5% specificity (95% CI, 25.6%-29.5%)
Adding “thunder-clap” headache and “limited neck flexion on examination” (inability to touch chin to chest or raise the head 8cm off the bed if supine) resulted in 100% (95% CI, 97.2%-100%) sensitivity.
The rule was then evaluated using a bootstrap analysis on old cohort data to validate the rule.
Conclusion/Limitations
For alert patients older than 15 y with new severe nontraumatic headache reaching maximum intensity within 1 h
Not for patients with new neurologic deficits, previous aneurysms, SAH, brain tumors, or history of recurrent headaches (≥3 episodes over the course of ≥6 mo)
Investigate if ≥1 high-risk variables present:
Age ≥40 y
Neck pain or stiffness
Witnessed loss of consciousness
Onset during exertion
Thunderclap headache (instantly peaking pain)
Limited neck flexion on examination