Bottom line
ED crowding remains a critical problem in the US and globally. It is frequently driven by the “boarding” of admitted patients. Improved patient flow is needed to be able to take care of patients presenting with acute care needs.
University of Maryland Section of Global Emergency Health
Author: Jon Mark Hirshon, MD, MPH, PhD
A 50yo man found dow in the snow was brought into our ER last week in cardiac arrest with a bladder temperature of 21° C. Let’s warm him up!
We were able to get ROSC with CPR and ACLS and then used Artic Sun to re-warm successfully.
Other tips/tricks:
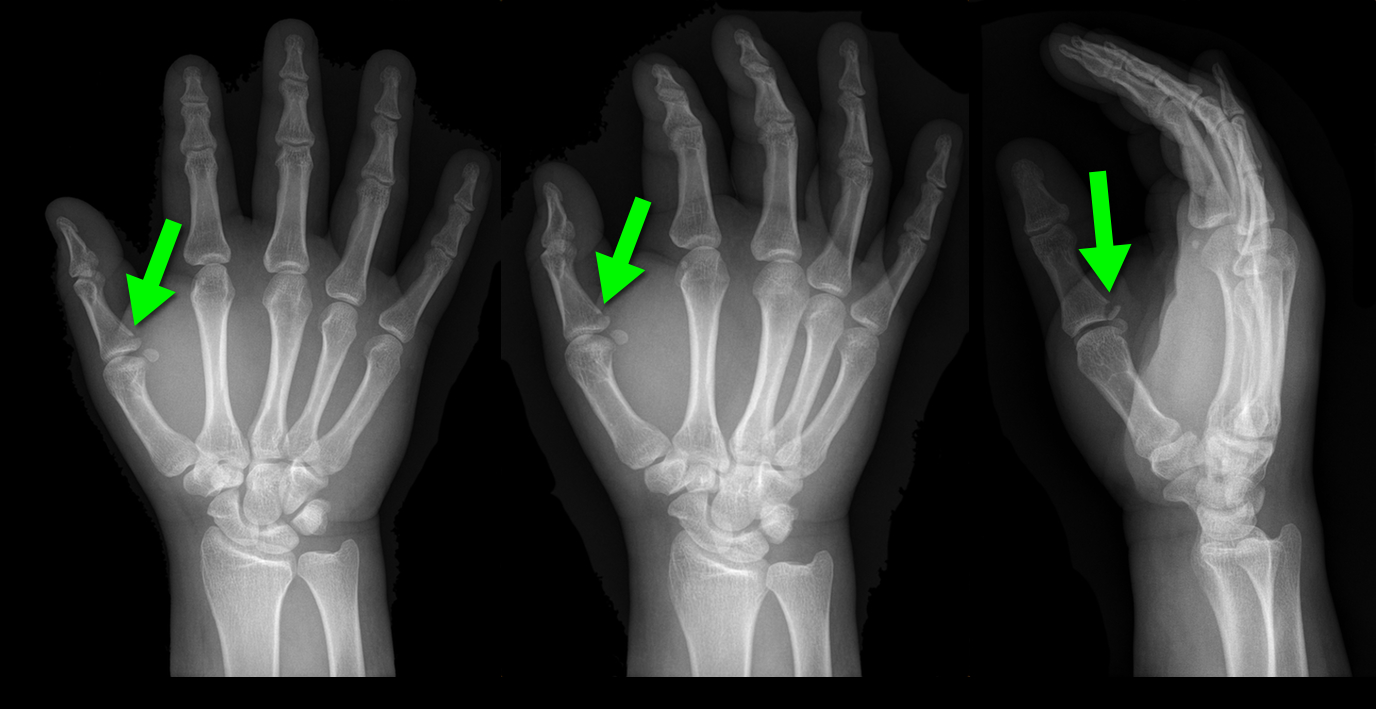
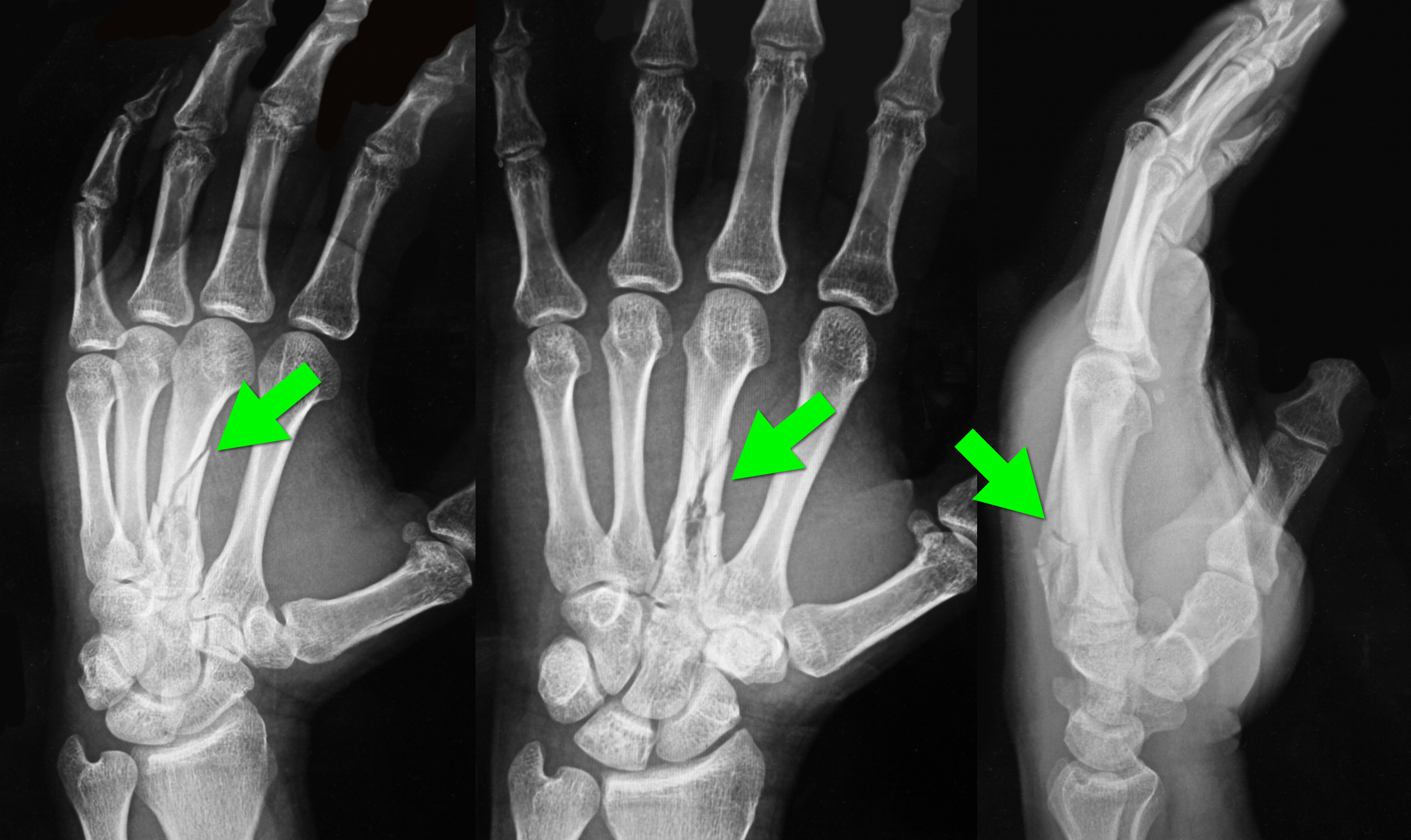
25 year-old male presents after falling off his bicycle. He complains of pain in his right-hand (he is right-hand dominant). What's the diagnosis?

The importance of new ST-segment depressions (STD) and/or T wave inversions (TWI) in lead aVL have not been emphasized or well recognized across specialties. Computer-assisted ECG readings typically report these findings as normal or nonspecific.
There is growing evidence that changes in lead aVL are abnormal, and that paying attention to that lead can be clinically useful. Reciprocal changes presenting as STD or TWI in lead aVL may be indicative of a significant coronary artery lesion and can sometimes be the only ECG manifestation of acute MI.
STD in lead aVL is considered a sensitive marker for early inferior STEMI, and has been shown to help differentiate STEMI from pericarditis. Another recent retrospective study suggests that TWI in aVL might be associated with significant LAD lesions.
Bottom Line: Paying close attention to subtle changes and abnormalities in lead aVL may help in early identification and initiation of therapy for patients who are having an acute MI.
Overtraining syndrome
A maladaptive response to excessive exercise without adequate functional rest
-Results in disturbances of multiple body systems (neurologic, endocrinologic, immunologic and psychologic).
- May be caused by systemic inflammation and resultant neurohormonal changes
- Multiple hypotheses exist
-Symptoms
Parasympathetic alterations: fatigue, depression, bradycardia
Sympathetic alterations: insomnia, irritability, agitation, tachycardia, hypertension, restlessness
Other: anorexia, weight loss, poor concentration, anxiety
Usual presentation is prolonged underperformance despite adequate rest and recovery (weeks to months).
Ondansetron (Zofran) is a great anti-emetic that, since it has gone generic, is also inexpensive. High dose ondansetron has been reported to cause QT prolongation and that practice is largerly discontinued now in the oncology world. Another uncommon adverse drug reaction may be dystonia. Though we think of ondansetron as a 5-HT3 blocker and should not cause the dystonic reaction like we see in metoclopramide, there are case reports of this reaction occurring.
Tranexamic Acid (TXA) topically applied was compared to anterior nasal packing in 216 patients with acute anterior epistaxis. Cotton pledgets (15 cm) soaked in injectable TXA (500 mg/5 ml) were inserted into the bleeding nostril and removed after bleeding had arrested. This was compared to standard anterior packing.
RESULTS
| TXA Anterior packing |
| % pts bleeding stopped in 10 min: 71% 31.2% |
| Discharge after 2 hours 95.3% 6.4% |
| Rebleeding in 24 h hours 4.7% 11% |
| Satisfaction scores 8.5 4.4 |
Bottom line: topical tranexamic acid looks promising for control of uncomplicated anterior epistaxis.
General Information:
Area of the world affected:
Relevance to the US physician:
Bottom Line:
VRU traffic injuries are the greatest challenge of today's worldwide road safety.
University of Maryland Section of Global Emergency Health
Author: Terrence Mulligan DO, MPH
Mechanical Ventilation During ECMO
34 year-old left-hand dominant male sustained injury to left hand after his pressurized greasing-gun discharged into the palm of his hand. He has a small lac to the hand but is in extreme pain. On exam his hand is very puffy and he is neurovascularly intact (XR below) What is the next step in management?

Myocardial Infarction in Women After Childbirth
World Health Organization reports that obesity is the 5th leading cause of global death with the highest impact on women <65 years of age
The association of obesity and cardiovascular risk in young women is currently being researched
A recent nationwide cohort looking at obesity and future cardiovascular risk looked at Danish women giving birth (2004-2009) and followed them a median time of 4.5 years
This study grouped women via pre-pregnancy body mass index (BMI)
1. Underweight (BMI <18.5)
2. Normal weight (BMI <25)
3. Overweight (BMI <30)
4. Obese (BMI >30)
Data revealed that healthy women of fertile age, pre-pregnancy obesity alone was associated with increased risk of myocardial infarction in the years after childbirth
In most situations (dependant on state laws and institutional policies), methadone-maintained patients enrolled in a drug abuse program are best managed by continuing methadone at the usual maintenance levels with once-a-day oral administration.
Pearl: In the event the methadone clinic is closed and/or the dose cannot be verified, 30-40 mg (10-20 mg IM) is generally enough to prevent withdrawal in most patients.
This is only a short-term measure and some patients may require additional methadone. Full doses of methadone should be reinstituted as soon as possible.
Case Presentation: A 63 year old woman from Texas with no recent international travel presents to the ED with persistent fatigue which onset a month ago and is associated with anorexia and occasional fevers and chills. She has been to her family doctor who tested her for a number of viral illnesses and was told she had West Nile virus.
Clinical Question:
What other febrile illness could this be?
Answer:
This patient had dengue. Dengue is now endemic in the US, and locally-acquired cases have been reported in Florida, Texas and Hawaii. The fatigue and anorexia are typical and can last for weeks after other symptoms have resolved.
West Nile virus testing may be falsely positive when another flavivirus is present such dengue, yellow fever or Japanese encephalitis.
Bottom Line:
Other possible illnesses like dengue should be considered in patients who have tested positive for West Nile virus.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
NSSTIs occur secondary to toxin-secreting bacteria; NSSTIs are surgical emergencies with a high-morbidity / mortality
Risk factors: immunocompromised host (DM, AIDS, etc.), intravenous drug use, malnourishment, peripheral vascular disease
Type I (polymicrobial; most common), Type II (monomicrobial; typically clostridia, streptococci, staph, or bacteroides), Type III (Vibrio vulnificus; seawater exposure)
Signs / Symptoms: pain out of proportion to exam (occasionally no pain at all), skin findings (blistering / bullae, gray-skin discoloration, or “Dishwater-like” discharge), or systemic toxicity (altered mental status, elevated lactate, etc.)
Diagnostic radiology
Treatment is emergent surgical debridement with simultaneous hemodynamic resuscitation PLUS broad-spectrum antibiotics; consider clindamycin becuase it has anti-toxin activity
Adjunctive therapies include Intravenous intraglobulin (neutralizes toxins secreted by bacteria) and hyperbaric oxygen
32 year-old with diabetes presents with fever, erythema, and warmth of his lower extremity; his leg is not particularly painful. He is diagnosed with cellulitis, started on antibiotics, and admitted to the hospital. While boarding in the Emergency Department he becomes rigorous and hypotensive. An ultrasound of his cellulitis is performed and is shown below. What’s the diagnosis?
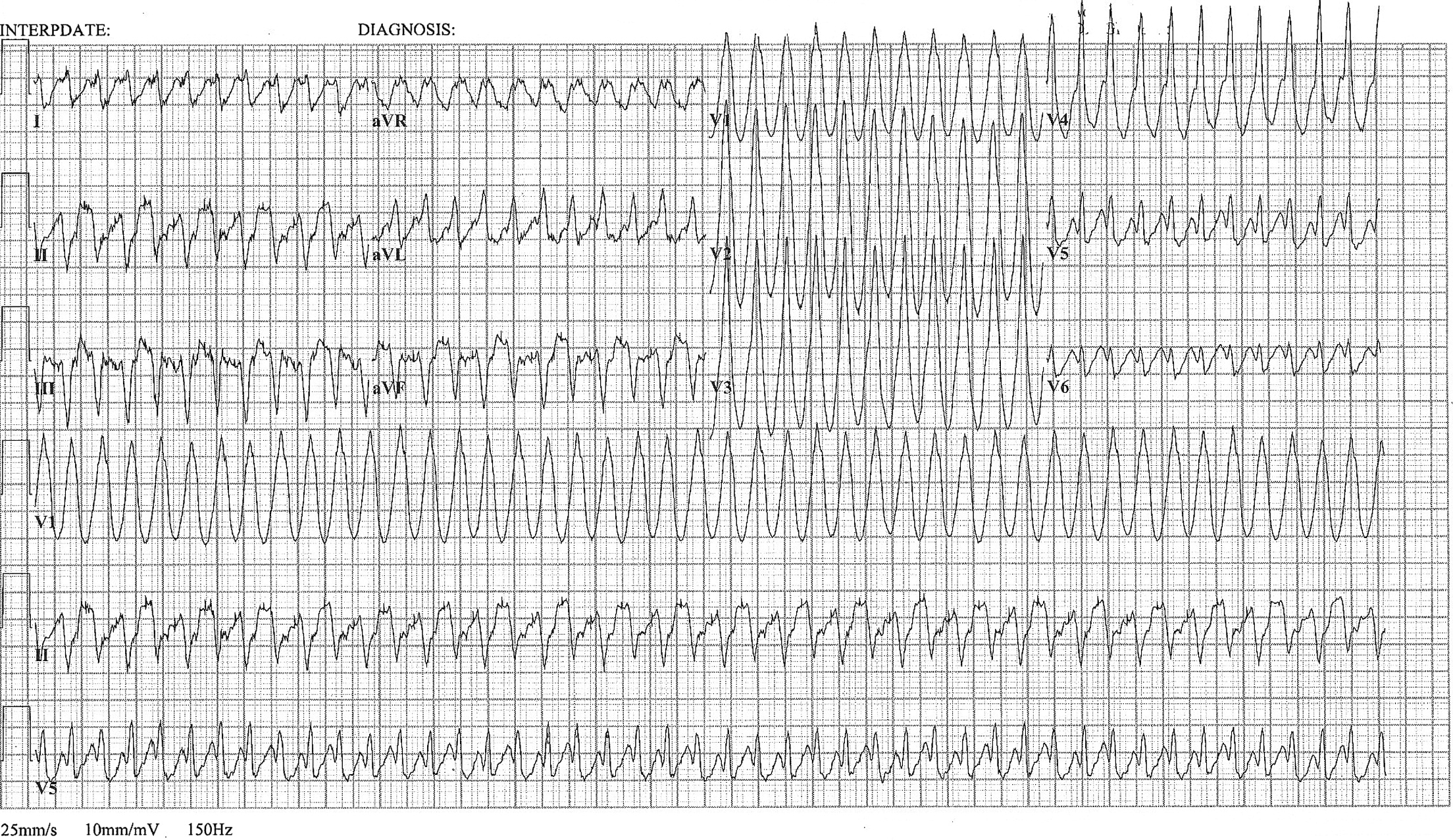
A 48 year old woman has acute chest pain and palpitations over the past several hours. She has felt similar palpitations in the past but never sought medical attention. She arrives to your ED alert and anxious. HR = 270, BP=130/100. ECG is below. What’s the diagnosis and treatment?
Pelllegrini-Stieda lesion
Ossified post-traumatic lesions at the MCL adjacent to the femoral attachment site of the medial femoral condyle.
Mechanism is likely from an avulsion injury that subsequently calcifies after the initial trauma.
Often an incidental finding on plain films.
If symptomatic, refer to ortho as an outpatient
If not symptomatic, no treatment is indicated
http://images.radiopaedia.org/images/30076/b62e61e83241e30f2da693901edcdc_gallery.jpg
http://www.imageinterpretation.co.uk/images/knee/PELLEGRINI%20STIEDA2.jpg
Everyone has admitted an altered mental status, patient or bradycardic patient and all of your test results are coming back normal except for a mild increase in creatinine. Take a look at the medication list. Creatinine is a poor indicator of renal function and GFR may be severely impaired even with a mild elevation of creatinine. If you have a predominantly renally excreted drug, you can see toxic effects of a drug even if administered at therapeutic levels.
Common bradycardia inducing medication that is renally cleared: atenolol (very high renal excretion) and digoxin (70%).
Altered Mental Status and on Keppra? Keppra is 100% renally cleared!
Ask your pharmacist for help with the medication list with renal or hepatic insufficiency.