Medical Cannabis is permitted in 39 states and Washington DC while 18 sates and Washington DC has legalized recreational cannabis use. As cannabis products become more available, pediatric exposure has also increased.
A retrospective study of National Poison Data System involving children < 6 years from 2017 and 2021 showed: Pre-COVID (2017-2019) & COVID (2020-2021)
Common Clinical effects
Disposition
Conclusion
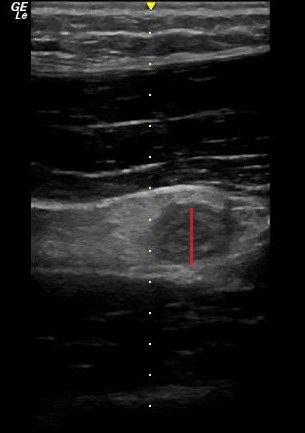
POCUS can be used to screen for appendicitis.
A recent study showed a sensitivity of 66.7% (CI 95% 47.1–82.7), and a specificity of 96.8% (CI 95% 83.3–99.9) during pregnancy, with the highest sensitivity in the first trimester.
2 methods to locate the appendix are:
1) have your patient point to the area where it hurts the most
2) perform a lawnmower technique over the right lower quadrant looking for the right psoas mucle and the iliac vessels. The appendix will usually be near these structures.
Sometimes it is easiest to use your curvilinear probe to identify an area of inflammation and then change to the linear probe for better visualization.
On ultrasound, appendicitis is defined as a non-compressible blind pouch with an outer diameter greater than 6 mm. On short axis the inflammed appendix will look like a target sign:
Shock index (heart rate/systolic blood pressure) has been used to predict trauma outcomes. This study from American Journal of Emergency Medicine looked at 89,000 pre-hospital patients who had a normal shock index on arrival at an emergency department. They then looked for those with abnormal pre-hospital shock index vs. those without an abnormal shock index and compared outcomes. Those with an abnormal pre-hospital shock index had worse outcomes than those with normal pre-hospital shock index.
Bottom line: A good handoff from pre-hospital to emergency department staff is critical because any abnormal shock index predicts a worse outcome than those with a normal shock index.
Author- Steve Schenkel, MD MPP Professor of Emergency Mediciner at UMEM:
A recent Annals of Emergency Medicine Publication (here https://www.annemergmed.com/article/S0196-0644(22)01276-8/fulltext) tested a predictive rule for Likelihood to Occupy an Inpatient Bed associated with a common Electronic Health Record.
At the individual patient level, the score performed ok. Depending on the chosen threshold, it traded off sensitivity and specificity and generally became more accurate the longer the patient was in the ED.
The authors and the associated editorial (here https://www.annemergmed.com/article/S0196-0644(22)01401-9/fulltext) suggest a different, potentially more beneficial use: to allow aggregate prediction of admissions across an entire department and therefore prompt earlier planning to prevent crowding on account of boarding.
The takeaway: Administrative prediction rules oriented toward individual patients may be more meaningfully used to predict resource needs, including in-patient beds, across the ED population.
Settings: Retrospective data from 3 Dutch EDs (development of the score), 2 Denmark ED (for validation of the score). The novel score (International Early Warning Score) will be composed of the National Early Warning Score (NEWS) + Age +Sex
Components of the National Early Warning Score:
Participants: All adult patients in the Netherlands Emergency department Evaluation Database (NEED) and Danish Multicenter Cohort (DMC).
Outcome measurement: in-hospital mortality, including death in EDs.
Study Results:
Discussion:
Conclusion:
This multicenter study showed that IEWS perform better than the NEWS for predicting in-hospital mortality for ED patients.
The use of a fascia iliaca compartment block has been shown to reduce pain, decrease length of stay and decrease the opiate requirements for patients with hip fractures.
Check out this page on how to perform this procedure.
Fascia iliac blocks can be challenging to implement routinely in the emergency department. Studies show that 2.5% of eligible patients, despite departmental implementation, receive a block.
One recently published article showed that large scale multi-disciplinary implementation can increase the use of fascia iliac blocks. After implementation, the study team found that 54% of eligible patients received a fascia iliac block.
This article is interesting as it provides helpful resources including physician and nursing protocols for performing this block.
Use of intravenous lidocaine has been proposed as an adjunct/replacement for opioids in trauma patients with rib fractures. These small studies show a signal that the use of lidocaine decreased the need for opiate pain medication in this cohort of patients. Larger studies are needed, however, trauma surgeons maybe reaching for intravenous lidocaine in patients they are admitting with rib fractures. Also, transdermal lidocaine patches have been shown to have a similar effect in this patient cohort. “In admitted trauma patients with acute rib fractures not requiring continuous intravenous opiates, lidocaine patch use was associated with a significant decrease in opiate utilization during the patients’ hospital course.” 3
How much screen time after concussion?
Adolescents spent more than 7 hours daily on screen time during the pandemic.
Historically, experts recommended screen time abstinence to various degrees after concussion.
Prior study: RCT of concussion patients (ages 12 to 25) found that those who abstain from screen time for the first 48 hours recovered 4.5 days sooner than those who were permitted screen time.
Population: 633 children and adolescents with acute concussion and 334 with orthopedic injuries aged 8 to 16, recruited from 5 Canadian pediatric emergency departments.
Post concussion symptoms were measured at 7 to 10 days, weekly for three months, and biweekly for three to six months post injury. Screen time was measured.
Results: Screen time was a significant predictor of post concussion symptom recovery with both parent reported somatic and self-reported cognitive symptoms.
There may be an effect of low to moderate screen time (Goldilocks effect) demonstrating that those in the 25th to 50th percentiles had less severe symptoms than those on the higher end of screen time use or those who minimally use of screens!
Low and high screen time were both associated with relatively more severe symptoms in the concussion group compared to the orthopedic injury group during the first 30 days post recovery but not after 30 days.
Conclusion: The association of early screen time with post concussion symptoms is not linear. Recommending moderation in screen time may be the best approach to clinical management.
Children need to strike a balance between avoiding boredom, deconditioning, isolation, and overexerting themselves physically or cognitively.
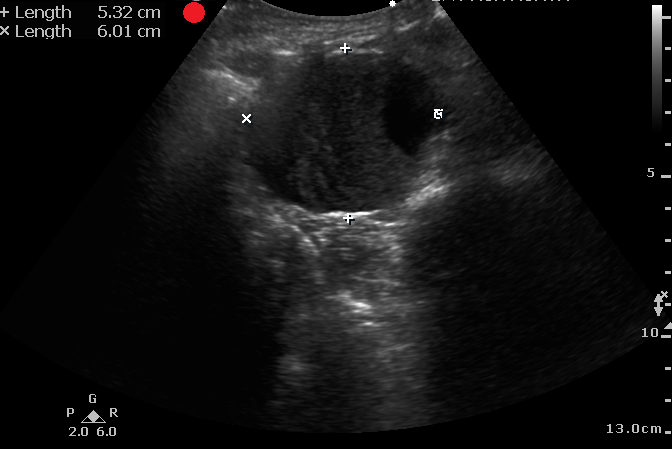
It is difficult to diagnosis a ruptured AAA with POCUS. However, based on one systematic review and meta-analysis, POCUS has a sensitivity of 97.8% and a specificity of 97% for diagnosing AAA in patients supsected of having a ruptured AAA.
Remeber:
Laslty, make sure you are measuring the aortic wall and not a mural thrombus.
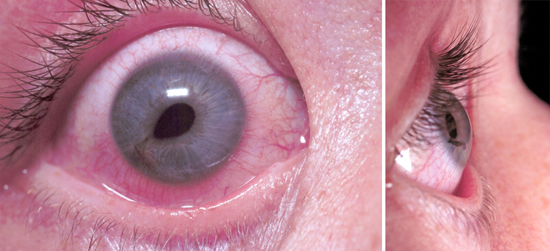
Lithium toxicity can present acutely with gastrointestinal symptoms and chronically with neurologic symptoms such as tremor and ataxia. Diagnosis and treatment with normal saline hydration and/or dialysis depends on lithium levels in conjunction with signs and symptoms.
Lithium levels can be falsely elevated when blood samples are collected in green top tubes which contain lithium heparin, or if the blood collection volume is too small. Not recognizing that a lithium level may be falsely elevated can lead to misdiagnosis as well as unnecessary hospitalizations and treatments. The study by Wills et al found lithium levels as high as 4 mmol/L (therapeutic range 0.6-1.2 mmol/L) in lithium naïve volunteers collected in the wrong tube and with small blood volumes. If a patient has an elevated lithium level in the absence of lithium toxicity symptoms, consider a falsely elevated level and redraw using the appropriate tube and sample size.
In summary:
a 37 year old patient comes in with chest pain, you obtain the following ECG. Is this a STEMI or Pericarditis?
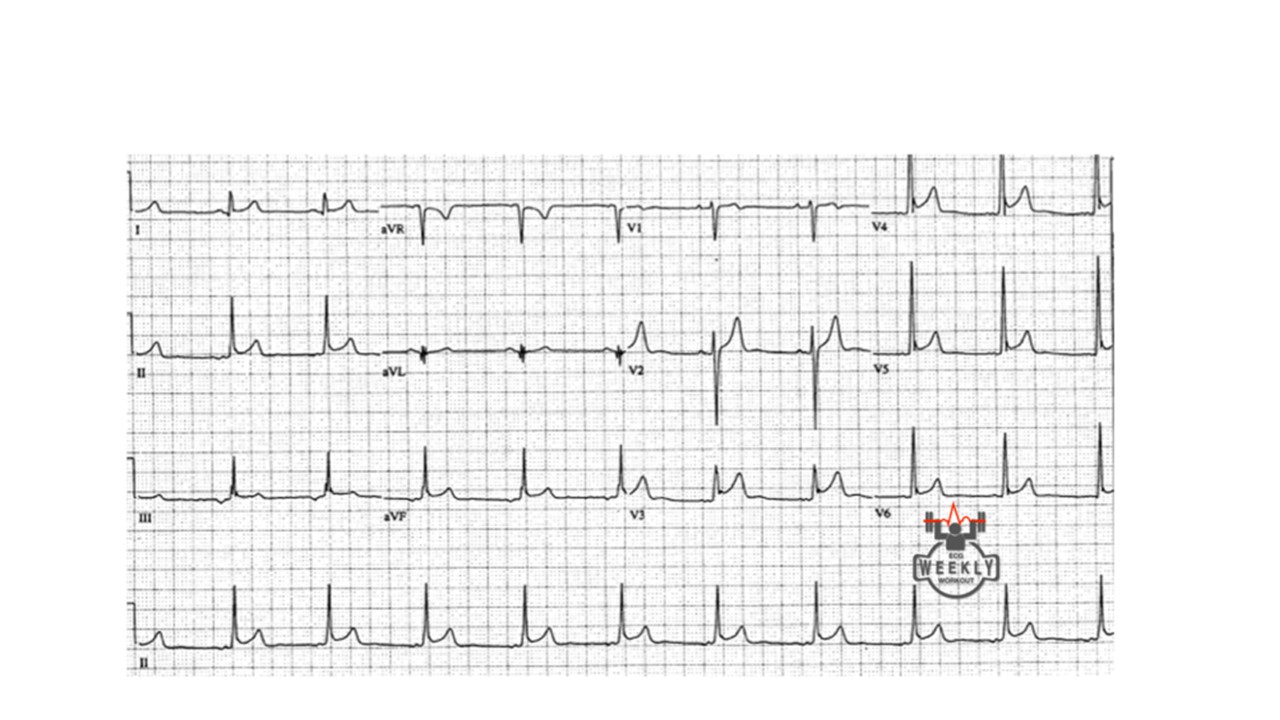
How can you tell? well, you follow the algorithm Dr. Mattu taught us....
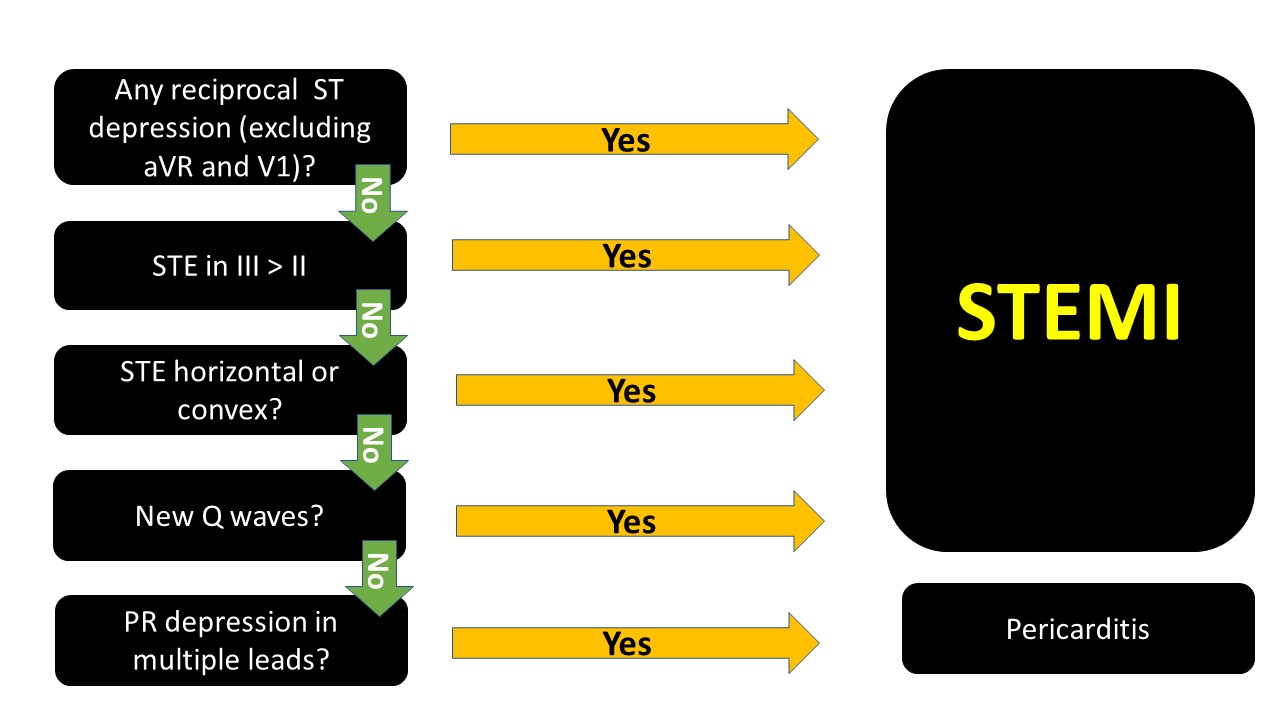
The ECG above, if you go through the algorithm you will see that it is most likely pericarditis.
note that PR depression can be transient and you might not see them.
When in doubt, it is not wrong to consult cardiology. Getting serial ECGs also is important, STEMIs will usually evolve.
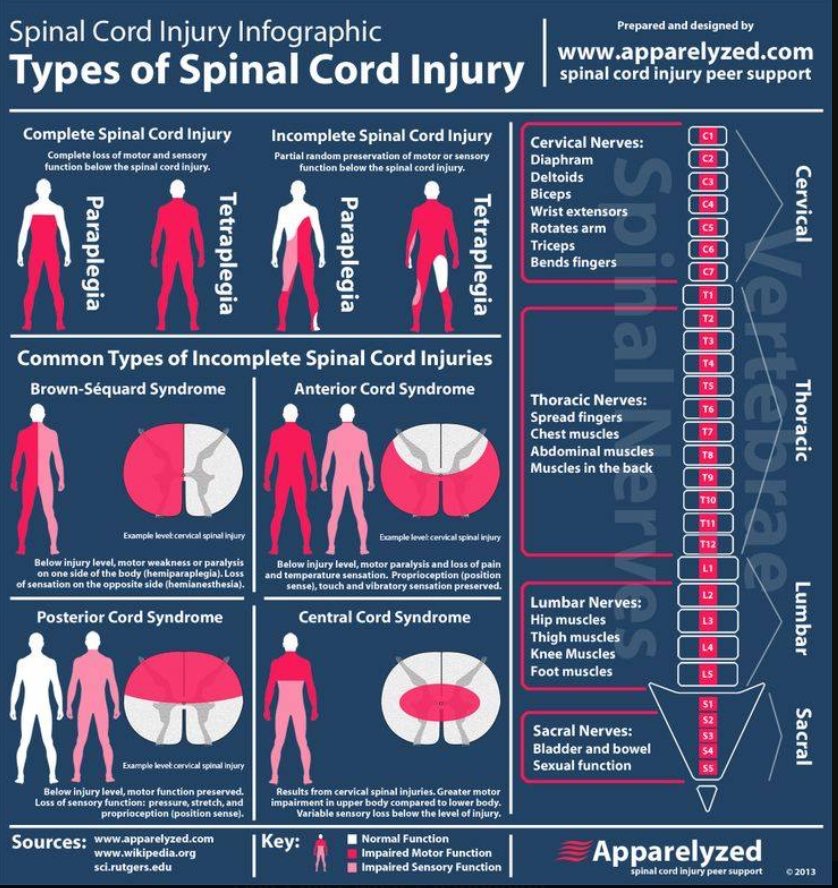
Recognizing that the studies discussing emergency department thoracotomy (ERT) in traumatic injuries are performed at large institutions where surgical back-up is available, emergency physicians should be familiar with the indications of emergency department thoracotomy in the setting of trauma. An informed decision should be made based on resources available along with the limited literature available to make the best decision for the patient and staff present.
Adding to last week’s pearl of no cardiac activity and no pericardial fluid on FAST exam, what else prognosticates intact survival? A 2020 paper concluded “ERT had the highest survival rates in patients younger than 60 years who present with signs of life after penetrating trauma. None of the patients with blunt trauma who presented with no signs of life survived.” 1A review in Trauma last month recommended: “Based on our scoping review of existing literature, we can conclude three major findings in the context of RT: (1) Resuscitative Thoracotomies (RT) performed in the setting of blunt trauma have a worse prognosis compared to patients undergoing RT for penetrating injuries, (2) procedures that have the potential to delay patient transport to hospital, such as intubation, may significantly increase the risk of mortality and (3) the presence of signs of life or hemodynamic stability in the prehospital or in-hospital setting are positive survival predictors in the setting of RT” 2 The best outcome is in patients brought immediately to an ED (preferably a trauma center) with limited on scene time. Police transport had a major association with survival in these patients. Stab wounds have the highest rate of intact survival.
For those at non-trauma centers, have a conversation within your ED group as well as with general surgeons (if available) to decide ahead of time if this procedure will be utilized in the setting of traumatic cardiac arrest and in which patient population.
Adhesive capsulitis aka frozen shoulder
Definition: Gradual development of global limitation of both active and passive shoulder motion, characterized by severe pain and lack of radiographic findings
Idiopathic loss of BOTH active and passive motion (significant reduction of at least 50%)
Motion is stiff and painful especially at the extremes.
Occurs due to thickening and contracture of the shoulder capsule.
Affects up to 8-10% of people of working age.
Affects patients between the ages of 40 and 60.
Peak age mid 50s
Onset before 40 is rare (consider other diagnosis).
Affects women more than men.
Diabetes is the most common risk factor.
Patients with DM, suffer a more prolonged course and are more resistant to therapy
Also associated with thyroid disease and prolonged immobilization
Increased risk following trauma to shoulder region (rotator cuff tear, following shoulder surgery, fracture of proximal humerus)
Presents unilaterally (other shoulder may become involved in next 5 years)
Slight increased risk of non-dominant shoulder
Take away: Be prepared (with blood products and/or vasopressors) for hypotension in trauma patients post-intubation particularly the elderly and severely injured. Pre-intubation tachycardia predicts post-intubation hypotension. Resuscitation with saline in traumatically injured patients is inferior to blood products or permissive hypotension.
A UK study retrospectively looked at trauma patients undergoing helicopter based emergency medicine intubation using induction agents of fentanyl, ketamine, and rocuronium for hypotensive episodes. “This study demonstrates that more than one in five patients who undergo PHEA have a new episode of significant hypotension within the first ten minutes of induction. Increasing patient age, multi-system injuries, a higher baseline heart rate, and intravenous crystalloid administration by the ambulance service before HEMS arrival were all significantly associated with PIH, whereas the addition of fentanyl to the induction drug regime was not.”
Nitroglycerin easily migrates into polyvinyl chloride (PVC), a plastic commonly used in intravenous tubing due to its flexibility and low cost. A slow rate of flow and long tubing length increase the loss of nitroglycerin. While using less absorptive tubing (i.e. polyethylene or polypropylene) when administering nitroglycerin is recommended, most published clinical studies looking at nitroglycerin have used PVC tubing.
A 1989 study compared nitroglycerin delivery through PVC tubing and low sorbing tubing at various concentrations and flow rates.1 Samples were obtained from the nitroglycerin bottle and the distal end of the tubing at several time points.
A 2018 study enrolled 8 volunteers to receive nitroglycerin infusions through PVC tubing and low sorbing polyolefin tubing.2
Bottom Line: Most studies evaluating nitroglycerin use in various clinical scenarios have used PVC tubing. Doses based on use with PVC tubing may be too high when using less absorptive tubing. Employing more conservative dosing strategies when using low sorbing tubing can help mitigate the risk of adverse effects (i.e. hypotension, headache).