How many times have you had a patient with an allergy to codeine described as stomach upset? Or how about a rash with morphine (probably secondary to histamine release)? True anaphylactic reactions to opioids are very rare (< 1%). But what happens when you have a patient with a true allergy, but still need to give an opioid? No problem, you just need to choose one that is structurally different.
All of the group 1 and 2 agents are structurally very similar to each other and should not be given if a true allergy exists to any other natural or semi-synthetic derivative. Group 3 agents have structures different enough that they can be given to a patient intolerant to the natural or semi-synthetics without fear of cross reactivity. They are also very different from others in this same group.
Seizures in the Critically Ill
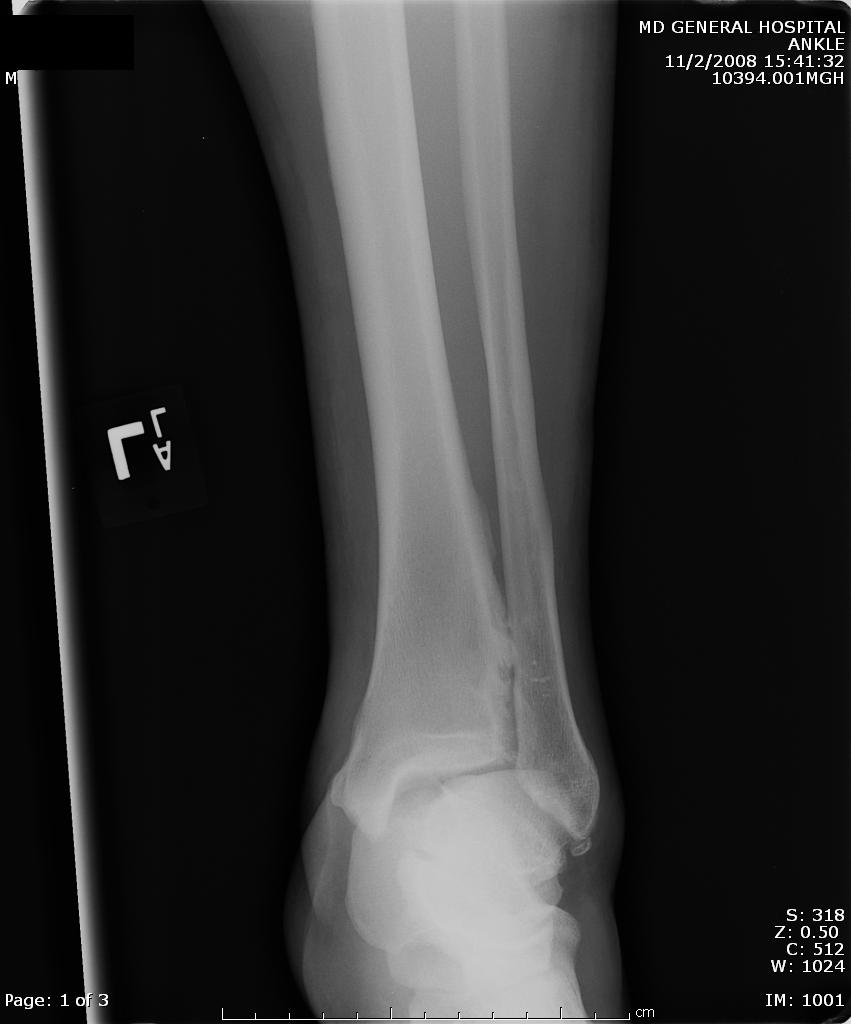
A maisonneuve fracture is a fracture dislocation resulting from external rotational forces to ankle -- through interosseous ligament to fibula.
If stability is questionable, orthopedic evaluation under anesthesia is required. Additionally always consider compartment syndrome. Do not rely on Kanduval's signs (pain, paraesthesia, pallor, poikilothermia, pulselessness) - "... with the exception of pain and paraesthesia, these traditional signs are not reliable." Emergent orthopedic consultation and compartment pressure assessment should be performed. (see attached photos)




This is a psychoactive herb which can induce strong dissociative effects by stimulation of the kappa receptor. It has become increasingly well known and available in modern culture, and popularized by YouTube Salvia (also known as Sage, Diviner's Sage, Magic Mint, or Sally D) is usually smoked, but can be chewed or ingested.
The high it produces is very intense, but lasts only approximately 10 minutes. Currently many states have enacted legislation against it, including Fla, IL, KA, MI, MO, ND, OK and VA, but it is available over the internet.

The following video demonstrates clinical effects of drug.
Although it is amusing, this is not meant to condone use.
(if you can not view the embeded video here is the link)
http://www.youtube.com/watch?v=w6dgXX0ytSo
- vertigo
- headache
- muscle weakness
- coordination abnormalities
- gait abnormalities
- visual abnormalities
Auto-PEEP in the non-COPD patient
The classic risk factors for coronary artery disease (e.g. hypertension, diabetes, smoking, etc.) are helpful at predicting the long-term risk of CAD, but they have limited utility at predicting whether a patient with acute symptoms is having an acute coronary syndrome or not. In one recent study of > 800 patients with suspected cardiac chest pain, 12% of patients with NO cardiac risk factors ruled-in for acute MI.
Never rule out ACS in a patient purely based on the absence of traditional cardiac risk factors!
[Body R, McDowell G, Carley S, et al. Do risk factors for chronic coronary heart disease help diagnose acute myocardial infarction in the Emergency Department? Resuscitation 2008;79:41-45.]
High altitude illnesses is typically called Acute mountain sickness (AMS) and is associated with two major complications high altitude pulmonary edema (HAPE) and high altitude cerebral edema (HACE).
Symptoms associated with AMS are headache, fatigue, nausea and vomiting, anorexia and insomia. Cough, Cyanosis, hypoxia, and dyspnea are associated with HAPE. HACE is associated with progressive neurologic symptoms and can lead to ataxia and coma.
Factors that increase your risk for altitude illnesses are:
How do we know if we really need to put all those red eyes sent in from daycare centers and schools on antibiotics? The following study shows us why.
Bacterial Conjunctivitis in Children
Methylenedioxymethamphetamine (MDMA) or "Ecstasy"
A designer club drug that has been classified as a "hallucinogenic" amphetamine though it does not cause visual hallucinations like are reported with LSD. It has many of the sympathomimetic effects like other amphetamines but its main mechanism of action which both causes the euphoria and toxicity is serotonin agonism. Since Anti-diuretic hormone is released by the hypothalamus under the direct regulation of serotonin, there is a transient but dangerous episode of Syndrome of Inappropriate ADH (SIADH). Combined with the club culture and fear of dehydration while taking MDMA, patients ingest MDMA concomitantly with free water through the night further exacerbating the hyponatremia. The time sequence of events for these patient is (women appear genetically predisposed to this phenomena):
Treatment: Fluid restriction - this is the one time that the 1L NS Bolus can kill a patient with cerebral edema. If you must give fluid give 3% NaCl if there is symptomatic hyponatremia. Remember the patient has dropped their sodium in about 24 hours so you can replenish in about the same time quite safely and even faster in severe cases. Treated correctly, patients improve rapidly - within 24-48 hours. Read a great case report in the reference below.
-- motor function (right leg)
-- motor function (left leg)
-- gaze
-- visual fields
-- language
Ventilator Therapy for ED Patients with ARDS
Reversal of Warfarin
Reversal of Warfarin can be accomplished by administering any of the following:
A few pearls:
Syncope patients are often misdiagnosed as having a seizure. Some factors favoring true syncope:
1. Preceding nausea or diaphoreses
2. Oriented (not confused) upon waking (no post-ictal period).
3. Age > 45
4. Prolonged sitting or standing before episode
5. History of CHF or CAD
Factors favoring seizures:
1. History of seizure disorder
2. Tongue biting
3. Confusion upon waking
4. Loss of consciousness > 5 min
5. Age < 45
6. Preceding aura
7. Observed unusual posturing, jerking, or head turning during episode
Management of Felons
For good photos of the incision technique please visit the reference article listed.
Clark, DC. Common Acute Hand Infections. Am Fam Physician 2003;68:2167-76
With the cooler weather on us all our favorite viral infections will start to appear. Included in this is the "slapped - cheek disease" Erythema infectiosum.
Erythema Infectiosum
Olanzapine (Zyprexa)
This is an atypical antipsychotic that gained popularity because it caused less sedation and fewer extrapyramidal effects. However, there are many other adverse effects that need to be emphasized. Some of these may contribute to a patient's condition in the ED: