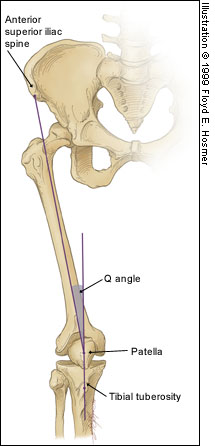
Patellofemoral Syndrome (Chondromalacia Patella)
Slipped capito-femoral epiphysis (SCFE) is a favorite board exam topic, and typically involves a young early or pre-adolescent obese girl with hip pain and the classic "ice cream falling off the cone" appearance on hip radiographs. However, keep these three pearls in mind when thinking about SCFE:
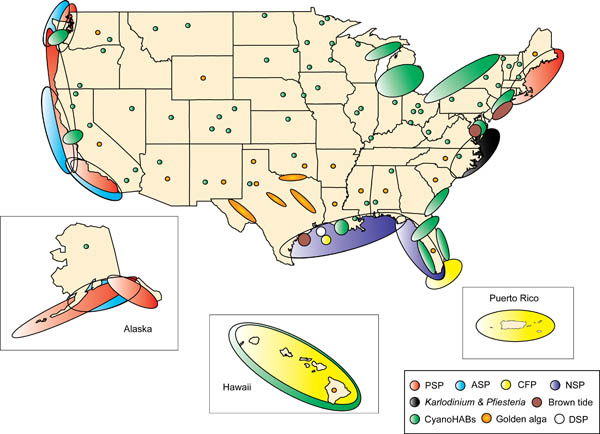
Although we may not be able to eat as much shellfish after the oil spill, there are still some left that can cause some interesting toxicity here in the USA. Shellfish act as vectors for the bacteria, virus etc that produces toxin thus not specific to one species of shellfish. There is a map attached that shows where shellfish poisoning occurs most. In the picture CFP=ciguatera, PSP=Paralytic and ASP=AmnesticC. Surprising the distribution and it will be interesting how the oil spill affects the distribution. Treatment for all of these is supportive with no known antidote and incidence increases during Red Tide months:
Chlorhexidine (CHG) has rapidly become the antiseptic of choice for most skin preparation prior to any percutaneous procedures including:
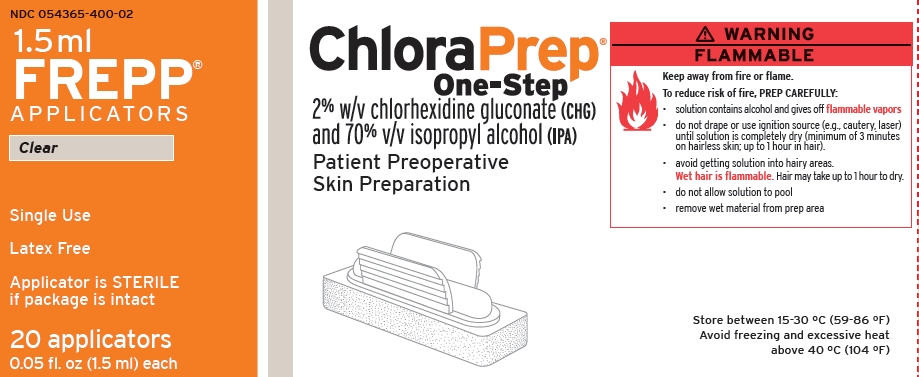
The Chlorprep(R) label notes: "DO NOT USE FOR LUMBAR PUNCTURE OR IN CONTACT WITH THE MENINGES" (attached)
Authors of the British Royal College of Anaesthetists 3rd National Audit Project provided some guidance for the use of chlorhexidine for spinal procedures
Further: Correspondance from the Journal of Regional Anesthesia and Pain Medicine
"Dr. David Hepner published a correspondence in the April 2007 issue of Anesthesiology that stated the expert panel for Regional Anesthesia and Pain Medicine “felt strongly that although the US Food and Drug Administration has not approved chlorhexidine before lumbar puncture, it has a significant advantage over povidone iodine because of its onset, efficacy, and potency” and commented that “interestingly, povidone iodine is also not approved for lumbar puncture."
Chlorhexidine off-label use is supported in academic literature. Due to specific labeling prohibiting use, a formal institutional policy to support such use may be indicated.
While you should always involve ID consultants when managing critically-ill HIV/AIDS patients on HAART, consider this; sub-therapeutic levels of anti-retrovirals may promote HIV resistance, potentially invalidating a class of drug for future use. Therefore, it may be advantageous to discontinue the drug(s) during critical-illness to avoid resistance.
Two examples leading to sub-therapeutic HAART levels in critical-illness:
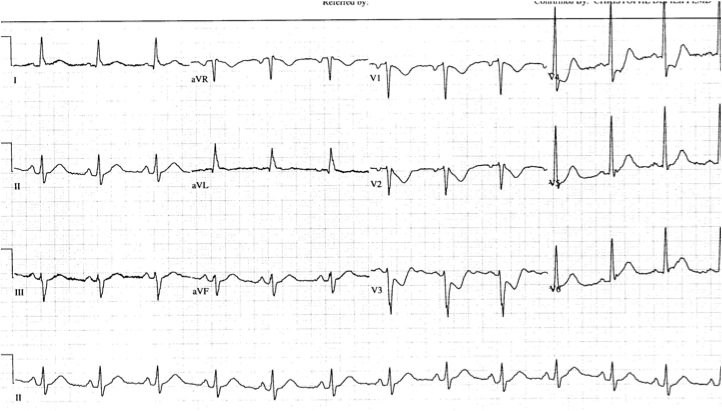
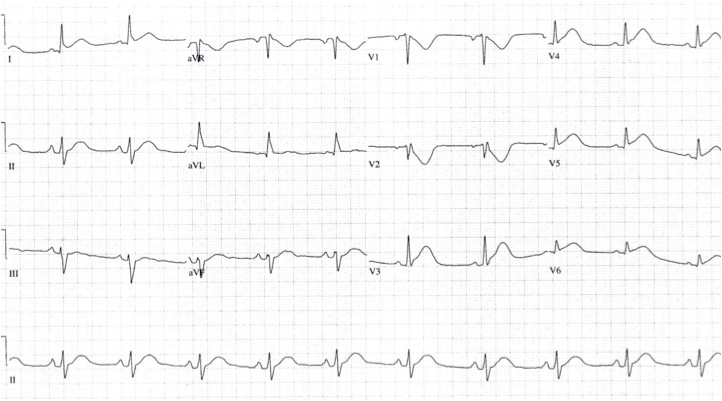
Approximately 4% of acute MIs will present as an isolated posterior MI (AKA "true posterior MI"). These are easily misdiagnosed as simply anterior ischemia because of the ECG findings. However, the distinction is critically important because posterior STEMI is now considered an indication for immediate reperfusion (PCI or lytics), whereas anterior ischemia is not.
The diagnosis of posterior STEMI is made by looking for:
1. ST segment depression, typically in leads V1-V3
2. upright T-waves in leads V1-V3
3. development of tall R-waves (R > S in amplitude) in V1-V3 over the course of a few hours (this is analogous to Q-waves forming in the posterior portion of the ventricle)
Early on, you may not be able to rely on the presence of tall R-waves to help you. Therefore, it's best to simply do the following: whenever you find ST-segment depression in leads V1-V3, always repeat the ECG using posterior leads (simply place a couple of the V leads on the left mid-back area). These leads will "look" directly at the posterior heart. If those leads show ST elevation, the diagnosis is posterior STEMI. If those leads don't show ST elevation, you can then make the diagnosis of simply anterior ischemia and hold off on immediate PCI or lytics.
The first ECG below shows ST depression in the anteroseptal leads, suspicious for posterior STEMI. The ECG was then repeated, second ECG, with leads V3-V6 placed wrapping around to the left mid-back area. The ST elevation in these leads confirmed the presence of a posterior STEMI and justified immediate reperfusion therapy.
Injury was originally described as an occupational hazard in Scottish gamekeepers (from breaking the necks of rabbits against the ground). Today, skiing is now the most common cause and injury is now the second most common orthopedic injury in skiers (MCL injury #1).
Injury to the ulnar collateral ligament (UCL) results from a sudden forced abduction (radial deviation) stress at the MCP joint of the thumb, commonly due to a fall against a ski pole or the ground.

http://blog.fitter1.com/wp-content/uploads/2010/04/b_14_1_2a.jpg
The most frequent site of rupture is the insertion into the proximal phalanx. The UCL may even avulse a small portion of the proximal phalanx at its insertion site.

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652013.jpg
Consider imaging before stress testing (to avoid further displacing a fracture)

http://img.medscape.com/pi/emed/ckb/sports_medicine/84611-97564-98460-1652060.jpg
Stabilize in a thumb spica splint and refer to hand surgery.
Calling this entity a “simple sprain” may result in chronic disability (chronic pain, instability, loss of pinch strength)
Life-threatening Bleeding in Hemophilia A Patients
Pulmonary Embolism and IVC Filters
Inferior vena cava filters are placed in patients with massive DVT and /or in patients who cannot receive systemic anticoagulation.
The question is, can patients develop pulmonary embolism if a filter is already in place? The answer: yes
How does this happen?:
There is a correction factor for erythrocyte sedimentation rate in the elderly. The top normal ESR in the elderly is (age + 10)/2. For example, an 80 yo patients would have a top normal ESR of (80+10)/2 = 45. Most laboratories do not, however, report this correction factor, but simply list < 20 (or thereabouts) as normal.
Be certain to take this correction factor into account when using ESRs for workups for temporal arteritis or other similar conditions.
Pain Control in the Elderly
So the take home lesson for this pearl is that the elderly have a lower risk of delirium if their pain is treated appropriately.
A fentanyl patch contains 100-fold more fentanyl in the reservoir than what is posted on the patch. For instance, 100mcg/hr patch will have over 10mg - thats milligrams - of fentanyl. This provides a rather large source for potential abuse. Overdose and deaths have occurred by patients in the following ways:
It is the many
(Sorry for the previously mislabeled pearl...)
Necrotizing soft tissue infections (NSTI) are on the rise and, despite improved surgical and critical care, over the years there has only been a mild reduction in mortality. Survival is associated with early diagnosis and treatment. Unfortunately, NSTI are not always obvious because deeper tissues made be involved first. Despite a validated scoring system and better radiology, our clinical suspicion still rules and relies on a meticulous history and physical exam.
Here are some subtle signs of NSTI:
Pain out of proportion to exam
Edema beyond region of erythema
Skin anesthesia
Skin erythema and/or hyperthermia
Epidemolysis
Skin bronzing
If NSTI is suspected, be vigilant! Start broad-spectrum antibiotics, begin appropriate resuscitation and involve your surgeons early.
17-18% of cases of syncope are attributable to arrhythmias
The greatest predictors of arrhythmias as the cause of syncope are:
a. Abnormal ECG (odds ratio 8.1)
b. History of CHF (odds ratio 5.3)
c. Age older than 65 (odds ratio 5.4)
[Sarasin, et al. Academic Emergency Medicine 2003]
Supraspinatus: “Empty can” test. Have the patient abduct the shoulders to 90 degrees in forward flexion with the thumbs pointing downward. The patient attempts to lift the arms against the examiner’s resistance.
http://bjsportmed.com/content/42/8/628/F2.large.jpg
Infraspinatus and teres minor: These muscles are responsible for external rotation of the shoulder. Have the patient flex both elbows to 90 degrees while the examiner provides resistance against external rotation.
http://www.physio-pedia.com/images/4/4b/Infraspinatus_test.jpg
Subscapularis: “Lift-off” test. The patient rests the dorsum of the hand on the lower back (palm out) and then attempts to move the arm and hand off the back. Patients with tears may be unable to complete test due to pain.
http://www.aafp.org/afp/2008/0215/afp20080215p453-f4.jpg
As RSV season approaches, remember these key points in managing bronchiolitis:
In the setting of acute cyanide poisoning, it is virtually impossible to obtain a timely cyanide level to help assess toxicity. However, there are two diagnostic tests that can help confirm your diagnosis.
Remember cyanide halts cellular respiration meaning the cells cannot utilize oxygen. Therefore, the venous PO2 should be about the same as the arterial PO2. The cells then switch to anaerobic metabolism, thereby producing lactate.
How to Perform a Median Nerve Block
{kind=link}
{kind=link}
{kind=link}