Fabella Syndrome
The fabella is a sesamoid bone that is embedded in the tendon of the gastrocnemius muscle where the fibers of the popliteus, arcuate complex and the fibular-fabellar ligament attach.
Fabella syndrome is a painful condition of the posterolateral knee that is exacerbated when the knee is extended. The pain can be exacerbated by palpation of the fabella and if it is compressed against the condyles. The condition is most common in adolescence, but occurs in adults too.
Consider this condition in patients with posterolateral knee pain, which can also be due to tears of the posterior horn of the lateral meniscus, and tendonitis of the lateral head of the gastrocnemius.
General information:
· Salmonella typhi – transmission through fecal-oral, contaminated food, human carriers
· Most cases in the US acquired abroad – Africa, Latin American, Asia
· Vaccine available – not life-long immunity, need 1-2 weeks to take effect
Clinical Presentation:
· sustained high fever (103-104)
· Faget sign: fever and bradycardia (also seen in yellow fever, atypical pneumonia, tularemia, brucellosis, Colorado tick fever))
· Abdominal pain, GI bleed/perforation, hepatosplenomegaly, delirium
· “Rose spots” – erythematous macular rash over chest and abdomen
· Without treatment sx can resolve after 3-4 weeks, mortality from secondary infections 12-30%
Diagnosis:
· Pan-culture for S. typhi
· Serologic: Widal test (negative for 1st week of symptoms, 7-14 days to result)
Treatment:
· Abx: amoxicillin, trimethoprim-sulfamethoxazole, and ciprofloxacin
· MDR typhoid: ceftriaxone or Azithromycine 1st line
Bottom Line:
· Get vaccinated if travelling to endemic areas 1-2 weeks before travel
· Suspect in travelers to endemic areas with sustained high fevers
· Spontaneous resolution does occur but may become carriers without abx
Famous victims or Typhoid fever:
· Wilbur Wright (Wright brothers)
· Prince Albert (Queen Victoria’s husband)
· Hakaru Hashimoto (discovered Hashimoto’s thyroiditis)
· Abigail Adams (1st Lady, wife of John Adams)
University of Maryland Section of Global Emergency Health
Author: Veronica Pei, MD
Monitoring Hyperosmolar Therapy
60 year-old male with a history of pulmonary fibrosis presents to the Emergency Department after a lung biopsy. He is complaining of facial swelling and dyspnea. What's the diagnosis?

Diffuse Idiopathic Skeletal Hyperostosis
aka 1) ankylosing hyperostosis, 2) Vertebral osteophytosis
Large amount of osteophyte formation in the spine, confluent, spanning 3 or more disks
Most commonly seen in the thoracic and thoracolumbar spine.
Osteophytes follow the course of the anterior longitudinal ligaments.
2:1 male to female ratio. Most patients >60yo.
Sx's: Longstanding morning and evening spine stiffness.
PE: Spinal stiffness with flexion and extension.
Dx: plain films
Tx: NSAIDs and physical therapy
http://www.learningradiology.com/caseofweek/caseoftheweekpix2013%20538-/cow542-1arr.jpg
Strychnine poisoning is still occasionally found in rat poisons and in adulterated street drugs and herbal products. The typical symptoms are involuntary, generalized muscular contractions resulting in neck, back, and limb pain. The contractions are easily triggered by trivial stimuli (such as turning on a light) and each episode usually lasts for 30 seconds to 2 minutes, for 12 to 24 hours. Classic signs include opisthotonus, facial trismus, and risus sardonicus.
Differential diagnosis includes:
Case Presentation:
A Spanish speaking man in his late 20s is brought in by ambulance for severe dyspnea. Given the language barrier and his clinical status you are unable to obtain any history. He is tachypnic, had a low pulse ox, and was placed on BiPAP. On exam you hear bibasilar rales and a faint holosystolic murmur.
Clinical Question:
What should be included in the differential?
Answer:
Rheumatic heart disease is the result of valvular damage due to an abnormal immune response following a group A streptococcal infection. It affects 15.6 to 19.6 million people worldwide. Most patients present with dyspnea between the ages 20-50. The most common valvular disease is mitral insufficiency, but it may present with mitral stenosis or aortic regurgitation. The disease is most prevalent in sub-Saharan Africa and among the Indigenous population of Australia but it can be found in many developing countries. People who live in rural areas without access to medical care are those at highest risk for developing rheumatic fever and subsequently rheumatic heart disease.
Bottom Line:
Rheumatic heart disease should be considered in patients who present from an endemic region.
University of Maryland Section of Global Emergency Health
Author: Jenny Reifel Saltzberg, MD, MPH
Fluid boluses are often administered to patients in shock as a first-line intervention to increase cardiac output. Previous literature states, however, that only 50% of patients in shock will respond to a fluid bolus.
Several validated techniques exist to distinguish which patients will respond to a fluid bolus and which will not; one method is the passive leg raise (PLR) maneuver (more on PLR here). A drawback to PLR is that it requires direct measurement of cardiac output, either by invasive hemodynamic monitoring or using advanced bedside ultrasound techniques.
Another technique to quantify changes in cardiac output is through measurement of end-tidal CO2 (ETCO2). The benefits of measuring ETCO2 is that it can be continuously measured and can be performed non-invasively on mechanically ventilated patients.
A 5% or greater increase in end-tidal CO2 (ETCO2) following a PLR maneuver has been found to be a good predictor of fluid responsiveness with reliability similar to invasive measures.
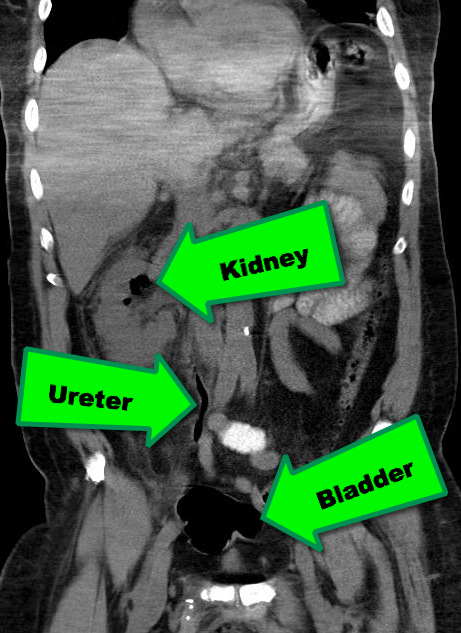
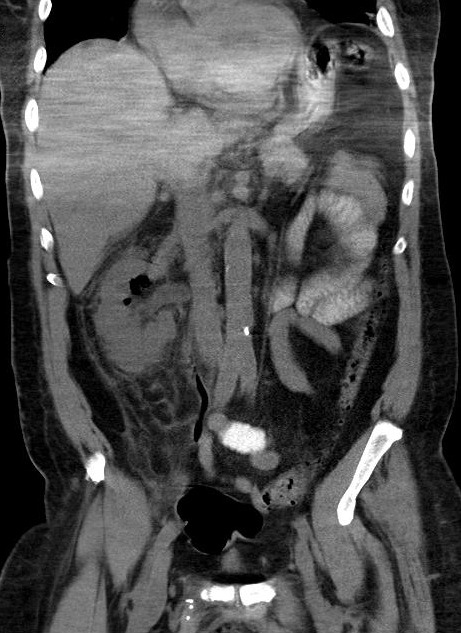
38 year-old male with a past medical history of diabetes presents with back pain and hypotension. CT scan is shown below. What's the diagnosis?
Introduction
Fosphenytoin is a prodrug and is metabolized quickly to phenytoin after administration. The conversion of fosphenytoin to phenytoin involves the release of phosphate. In fact, each mmol of fosphenytoin releases 1 mmol of phosphate.
Clinical Question
Are patients at risk for hyperphosphatemia after fosphenytoin loading?
Data
There are only two cases of reported hyperphosphatemia.
Bottom Line
Despite the phosphate load from fosphenytoin administration, hyperphosphatemia is very rare and probably associated with renal insufficiency and dosing errors.
Acute ischemic stroke occurs in 3.3/100,000 children per year. Up to 30% of these are caused by varicella. This can be diagnosed if the patient has had varicella infection within the past 12 months, has a unilateral stenosis of a great vessel, and has a positive PCR or IgG from the CSF.
Treatment includes anticoagulation, acyclovir for at least 7 days and steroids for 3-5 days.
Outcome is normally good and spontaneous improvement can be seen.
Inflammation of other arteries, including other areas of the brain, can also be seen. Treatment options for this can include high dose glucocorticoids and possibly immunosuppresive agents.
Approval of Kcentra™ may open the door for studying treatment of the bleeding patient on newer oral anticoagulants.
General Information: Antibiotics are generally classified as time- and concentration-dependent.
Concentration-dependent antibiotics
-Fluoroquinolones (i.e. Levofloxacin)
-Aminoglycosides (i.e. Gentamicin)
-Azithromycin
Relevance to the EM Physician:
Concentration-dependent antibiotics should be given at the highest appropriate dose for the target tissues (i.e. Levofloxacin 750mg for pneumonia is preferable to 500mg). This is also the rationale for high dose, extended-interval dosing for Gentamicin (>5mg/kg initial dose).
University of Maryland Section of Global Emergency Health
Author: Andi Tenner, MD, MPH
Neuromuscular Blocking Agents in the Critically Ill
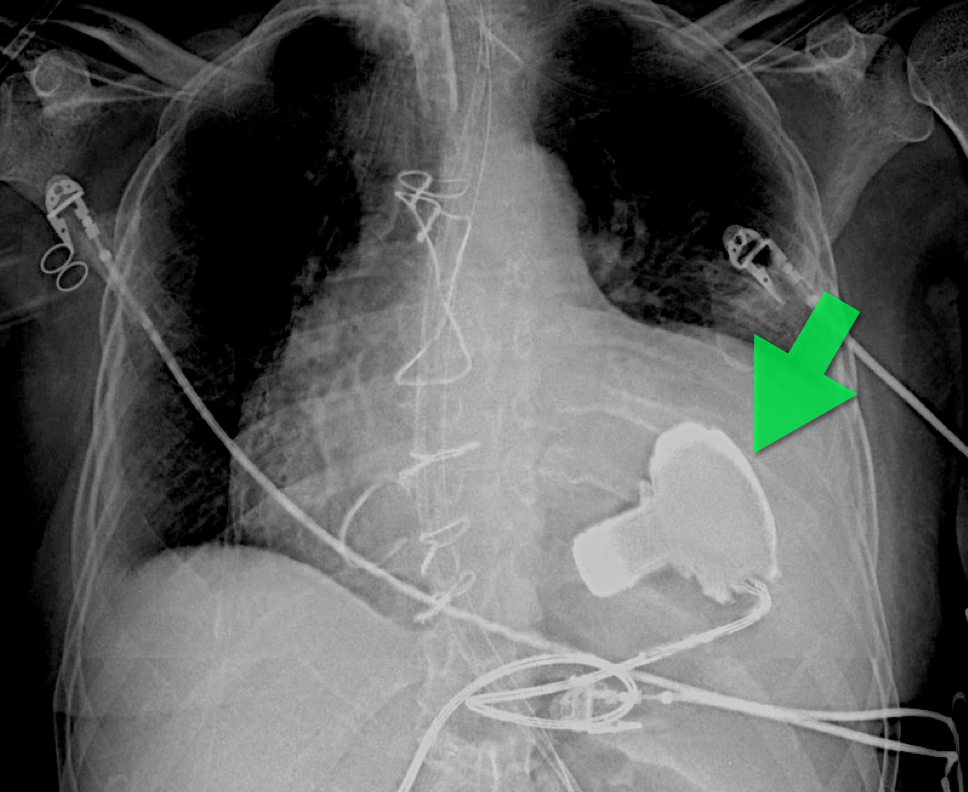
57 year old male presents with a cough. The CXR is shown below. What's the diagnosis?
You have a patient with a spinal cord syndrome and you order the MRI. Have you ever had that conversation with radiology where you have to "choose" what part of the spine you want imaged?
The entire spine needs to be imaged!
The reason: False localizing sensory levels.
For example: The patient has a thoracic sensory level that is caused by a cervical lesion.
A study of 324 episodes of malignant spinal cord compression (MSCC) found that clinical signs were very unreliable indicators of the level of compression. Only 53 patients (16%) had a sensory level that was within 3 vertebral levels of the level of compression demonstrated on MRI.
Further, pain (both midline back pain and radicular pain) was also a poor predictor of the level of compression.
Finally, of the 187 patients who had plain radiographs at the level of compression at referral, 60 showed vertebral collapse suggesting cord compression, but only 39 of these predicted the correct level of compression (i.e. only 20% of all radiographs correctly identified the level of compression).
The authors note that frequently only the lumbar spine was XR at the time of clinical presentation (usually at the referring hospital), presumably due to false localizing signs and a low awareness on the part of clinicians that most MSCC occurs in the thoracic spine (68% in this series).