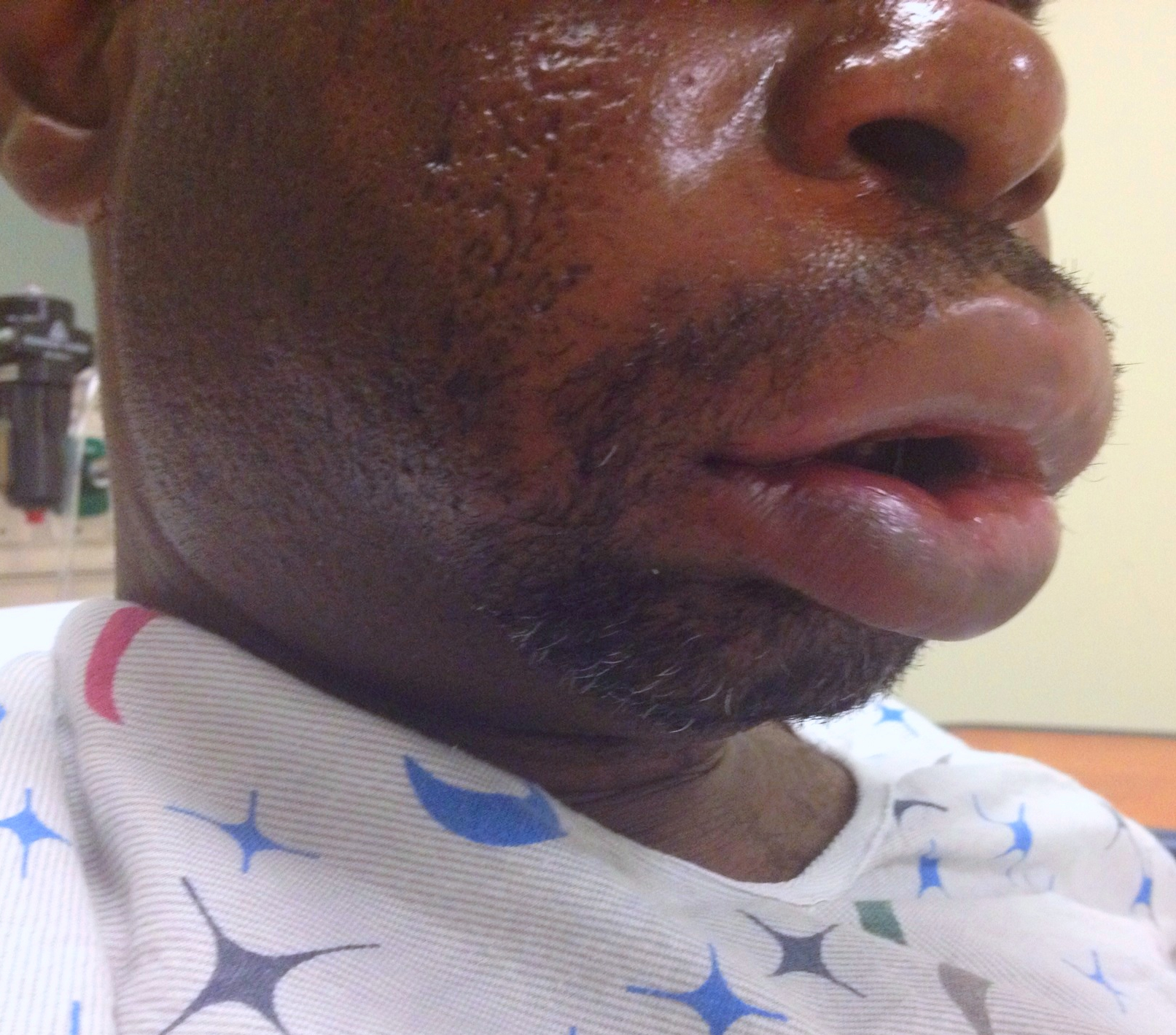
31 year-old male with recently diagnosed hypertension presents with rapid lip swelling. He started taking an unknown medication for his hypertension last week. Further history reveals that he has had prior, although milder, episodes previously. Name two medications that may help treat him.
Metacarpal Neck Fractures (i.e.: Boxer’s Fracture if 5th Metacarpal)
Depending on the MCP joint involved a certain amount of angulation is permissible before it adversely affects normal function.
Wishing everybody a Happy and Healthy New Year.
Despite a paucity of data, pain management clinics are administering topical gel mixtures that have included ketamine, tricyclics, calcium channel blockers and baclofen. Internet blogs have already identified this gel mixture as a way to "get high". This is one of those google searches you have to do on your own.
Bottom Line: A mild increase in blood parasite count after initiation of treatment is not uncommon. Marked increases should indicated treatment failure and the treatment drug should be changed to another class.
University of Maryland Section for Global Emergency Health
Author: Emilie J.B. Calvello, MD, MPH
VV-ECMO for Refractory Hypoxemia
52 year-old male with diabetes complains of severe left foot pain for one month and now inability to ambulate. Vital signs are normal and X-rays are shown below. What's the diagnosis and why should you get a biopsy early?

NSAIDs are commonly used by professional and recreational athletes to both reduce existing and/or prevent anticipated exercise induced musculoskeletal pain
NSAIDs have potential hazardous effects on the gastrointestinal (GI) mucosa during strenuous physical exercise
Potential effects include mucosal ulceration, bleeding, perforation. and short-term loss of gut barrier function in otherwise healthy individuals
Intense exercise by itself has previously been shown to induce small intestine injury
Human intestinal fatty acid binding protein (1-FABP) is a protein found in mature small bowel enterocytes which diffuses into the circulation upon injury
Ibuprofen and endurance exercise (cycling) independently result in increased 1-FABP levels
When occurring together, ibuprofen ingestion with subsequent exercise causes significantly increased small bowel injury and intestinal permeability
Small bowel injury was found to be reversible in 2 hours
Taking empiric NSAIDs before endurance exercise may be an unhealthy practice and should be discouraged in the absence of a clear medical indication
Parents bring in their child who placed a bead, seed, or other object up her nose. What do you do? Who should you call?
Research suggests that a decades-old home remedy (of sorts) known as the “mother’s kiss” may do the trick for children 1-8 years of age. It’s also much less invasive or frightening than some of the tools and techniques used in emergency departments with a success rate approaching 60%
First described in 1965, here’s how the mother’s kiss technique works:
Myth: The ornamental red plant - poinsettia - gained a reputation as a poisonous plant from a case report. In 1919, a 2-year-old child reportedly died from an ingestion and later an 8-month-old developed mucosal burns. These anectdotal case reports perpetuated the myth that poinsettia plants are poisonous. In the modern literature there is one single case of anaphylaxis(1) due to poinsettia ingestion/exposure, an allergic dermatitis(2) and one case of dermatitis(4).
Krenzelok et al.(3) showed there were 22,793 cases of poinsettia exposure and there were no fatalities reported to poison centers. 96.1% were kept at home without sequelae.
· A parasitic disease transmitted by the bite of the 'Glossina' insect (tsetse fly.)
· The disease is most prevalent in rural areas of Africa. Untreated, it is usually fatal. Infection with the genus Trypanosoma brucei gambiense may lead to chronic asymptomatic illness.
· Travelers to endemic areas in Africa are risk becoming infected.
· Symptoms resemble a viral illness; headaches, fever, weakness, pain in the joints, and stiffness. The parasite is able to crosses the blood-brain barrier and causes neurological symptoms, mainly psychiatric disorders, seizures, coma and ultimately death.
· Diagnosis is by serological tests (Card Agglutination Trypanosomiasis Test or CATT). Confirmation of infection requires the performance of parasitological tests to demonstrate the presence of trypanosomes in the patient.
· Treatment: four drugs are registered for the treatment of HAT: pentamidine, suramin, melarsoprol and eflornithine.
Management of patients with severe traumatic brain injury (TBI) typically involves the use of invasive intra-parenchymal pressure monitors. Although use of these monitors is recommended by TBI management guidelines, good quality evidence of benefit is lacking.
A recently published study evaluated the outcomes of TBI patients using a management protocol incorporating either an intracranial pressure (ICP) monitor compared to use of the clinical exam PLUS serial neuroimaging; a total of 324 patients were prospectively randomized into either group.
The primary study outcome was a composite of survival, impaired consciousness, and functional status at both three and six months.
The results of the study did not show a significant difference in the:
Bottom line: This study suggests that clinical exam PLUS serial neuroimaging may perform as well as invasive intra-parenchymal monitors for guiding therapy in TBI patients.
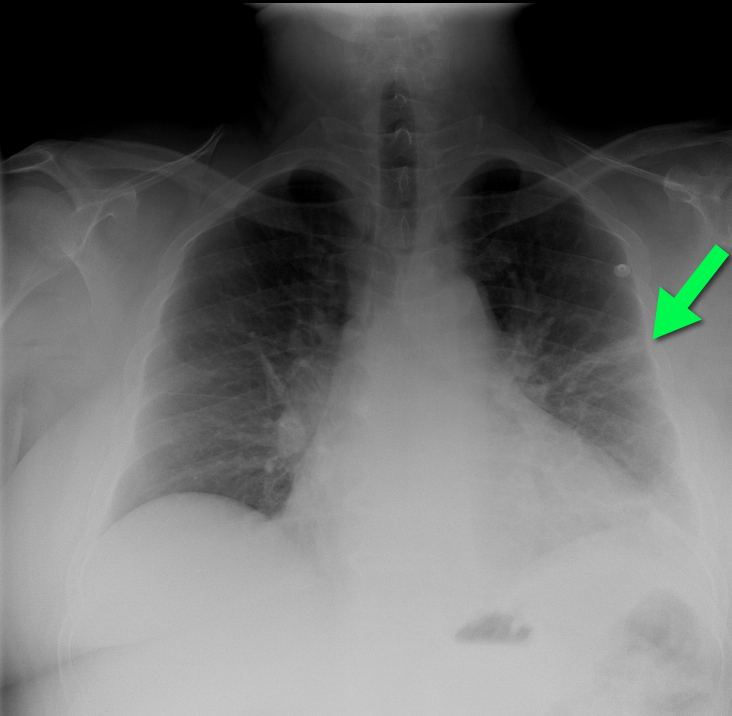
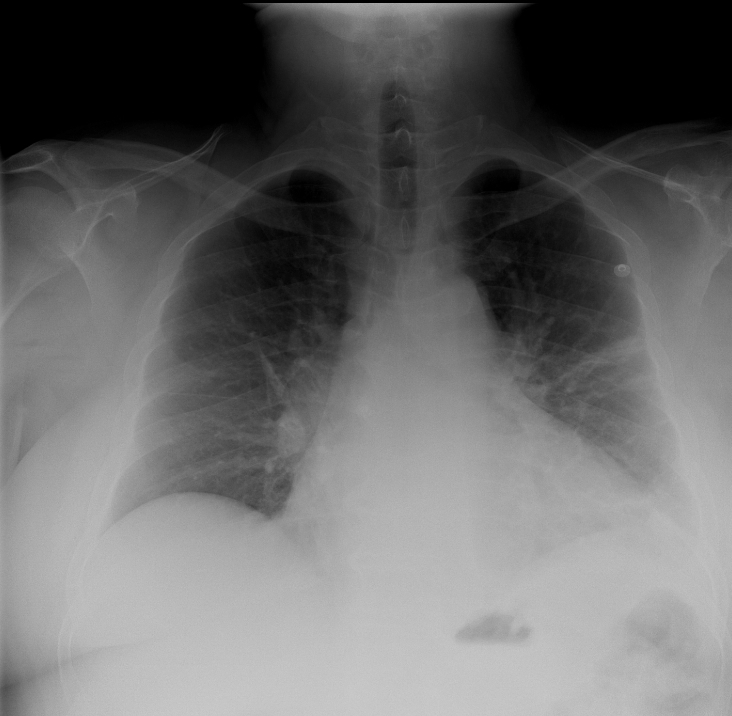
50 year-old man with presents with acute-onset sharp left-sided chest pain and dyspnea. What's the diagnosis and the name of the abnormality on chest x-ray?
Epistaxis can be a difficult thing to control in the ED, but there are several techniques you can learn that will make your life easier.
The majority of epistaxis cases are from kiesselbach's plexus therefore you can control it with:
Direct Pressure: Can be held with two fingers pinching the nares, or you can tape 4 tongue blades together and make your own "clothes pin" that can then be used to pinch the nares.
Vasoconstrictor and Anesthesia: A 1:1 mixture of topical lidocaine 4% and oxymetazoline can often be mixed together in the same oxymetazoline spray container enabling you to just spray it into the nares. This will often slow or stop the bleeding and provides anesthesia in case you need to cauterize the bleeding site. Some IV/IM narcotic pain medication will also help increase patient cooperation.
Visualize the bleeding site: Use a HEAD LAMP with an appropriate sized nasal speculum. You may look like Marcus Welby, MD but nothing works as well to see into the nose.
Cauterization It is best to cauterize circumferential around the bleeding site prior to directly cauterizing the actual site. Be careful with electrical cautery so has not to perforate the septum.
Nasal Packing: Instead of using surgilube to lubricate the packing; use Muprion, Bactroban or Bacitracin ointment to lubricate the packing. This will reduce the chance of Toxic Shock Syndrome.
The more well known causes of toxin-induced hyperthermia include sympathomimetics and anticholinergics. In addition, neuroleptic malignant syndrome, serotonin syndrome, and malignant hyperthermia are high on the differential.
Several other xenobiotics can cause hyperthermia in overdose as well:
In general, benzodiazepines should be considered first-line therapy, followed by barbiturates, propofol, or other sedative hypnotics. Phenytoin rarely has a role in the management of toxin-induced seizures. Extrenal cooling measures are also warranted. Specifically for isoniazid, pyridoxine should be administered immediately with a benzodiazepine.
Background:
Dengue is the most rapidly expanding mosquito-borne virus with an increasing incidence and geographical area. It is most commonly found in the tropics, but there are occasional outbreaks in other places, including Texas and Hawaii.
Clinical:
Three Phases:
1. The febrile phase lasts 2-7 dyas and is similar to other viral syndromes, often with high fever and nausea/vomiting. Petechiae may also be present which can be induced by the application of a tourniquet.
2. The critical phase occurs after defervescence and lasts only 24-48 hours. IT is marked by increased capillary permeability and can lead to severe pulmonary edema, shock, and multisystem organ failure.
3. The recovery phase is marked by hemodynamic improvement. Some patients have a rash described as "isles of white in a sea of red."
Some patients will develop bradycardia. Most patients have a self-limited form of the illness that is not severe, and consists of symptoms seen in the febrile phase. The patients that develop severe dengue can have markers in the febrile phase that are associated with organ dysfunction, GI bleeding, and increased capillary permeability. Other concerning symptoms early are abdominal tenderness and persistent vomiting.
Treatment:
Treatment is supportive, mostly consisting of IV fluids, which is very effective when started early in the patient's illness. For more information and maps of endemic areas check out the CDC or WHO websites: http://www.cdc.gov/travel/notices/in-the-news/dengue-tropical-sub-tropical.htm or http://www.who.int/denguecontrol/en/
University of Maryland Section for Global Emergency Health
Author: Jenny Saltzberg
Ultrasound-Guided Pericardiocentesis