Acute Disseminated Encephalomyelitis (ADEM) is primarily a pediatric disease and can cause a wide variety of neurologic symptoms. As such, should always be in the differential for pediatric patient presenting with vague neurologic symptoms including altered mental status. It is an immune-mediated, demyelinating disease that can affect any part of the CNS; usually preceding a viral illness or rarely, immunizations.
The average age of onset is 5-8 years of age with no gender predilection. It usually has a prodromal. That includes headache, fever, malaise, back pain etc. Neurological symptoms can vary and may present with ataxia, altered mental status, seizures, focal symptoms, behavioral changes or coma.
MRI is the primary modality to diagnose this condition. Other possible indicators may be mild pleocytosis with lymphocyte predominance, and elevated inflammatory markers such as ESR, CRP. These findings, however, are neither sensitive nor specific.
First-line treatment for ADEM is systemic corticosteroids, typically 20-30 mg/kg of methylprednisolone for 2-5 days, followed by oral prednisone 1-2 mg/kg for 1-2 weeks then 3-6-week taper. For steroid refractory cases, IVIG and plasmapheresis may be considered.
ADEM usually has a favorable long-term prognosis in the majority of patients. However, some may experience residual neurological deficits including ataxia, blindness, clumsiness, etc.
Take home points:
Take home naloxone (THN) programs have been expanded to help reduce the opioid overdose-related deaths. A study was done in Australia to characterize a cohort of heroin overdose deaths to examine if there was an opportunity for a bystander to intervene at the time of fatal overdose.
235 heroin-overdose deaths were investigated during a 2 year study period in Victoria, Australia.
Conclusion
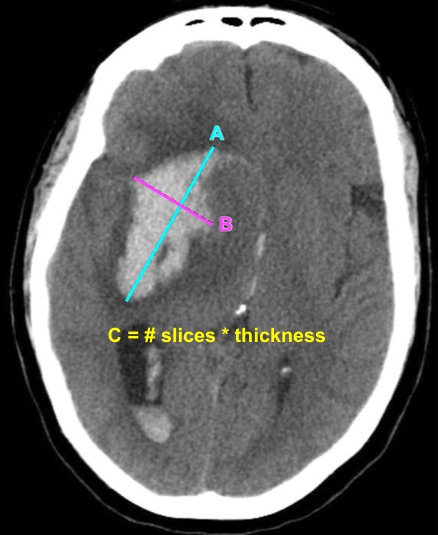
Bottom Line: EPs can reliably estimate ICH volume using the ABC/2 formula. Communicating ICH volume to neurosurgical and neurocritical care consultants can help direct treatment decisions.
Critically Ill Renal Transplant Patients
---Early antiviral treatment can shorten the duration of fever and illness symptoms, and may reduce the risk of some complications from influenza.
---Early treatment of hospitalized adult influenza patients with oseltamivir has been reported to reduce death in some observational studies.
---Clinical benefit is greatest when antiviral treatment is administered within 48 hours of influenza illness onset.
Antiviral treatment is recommended for patients with confirmed or suspected influenza who:
---are hospitalized;
---have severe, complicated, or progressive illness; or
---are at higher risk for influenza complications. (See below for in-depth information)
Oral oseltamivir is the recommended antiviral for patients with severe, complicated, or progressive illness who are not hospitalized, and for hospitalized influenza patients.
Treatment:
Doses: Oseltamivir 75 mg twice daily
Renal Impairment Dosing
CrCl >60 mL/minute: No dosage adjustment necessary
CrCl >30 to 60 mL/minute: 30 mg twice daily
CrCl >10 to 30 mL/minute: 30 mg once daily
ESRD undergoing dialysis: 30 mg immediately and then 30 mg after every hemodialysis session
Duration of Treatment:
Recommended duration for antiviral treatment is 5 days for oral oseltamivir. Longer daily dosing can be considered for patients who remain severely ill after 5 days of treatment.
Dyspnea in the Intubated Patient
The European Society of Intensive Care Medicine (ESICM) recently released a review with recommendations from an expert panel for the use of IV fluids in the resuscitation of patients with acute circulatory dysfunction, especially in settings where invasive monitoring methods and ultrasound may not be available.
Points made by the panel include:
Recommendations from the panel include:
Bottom Line: Utilize all the information you have about your patient to determine whether or not they require IVF, and reevaluate their physical and biochemical (lactate) response to fluids to ensure appropriate IVF administration and avoid volume overload.
Taking a double-dose of a single medication is presumed to be safe in most cases. However, there is limited data to support this assumption.
A retrospective study of the California Poison Control System was performed to assess adverse effects of taking double dose of a single medication. During a 10-year period, 876 cases of double-dose ingestion of single medication were identified.
Adverse effects were rare (12 cases). However, medication classes that were involved in severe adverse effects included:
Conclusion:
A previous pearl discussed medication-overuse headache (MOH).
MOH is also known as analgesic rebound headache, drug-induced headache or medication-misuse headache.
It is defined as headache… occurring on 15** or more days per month in a patient with a preexisting headache disorder who has been overusing one or more acute treatment drugs for headache with symptoms for three or more months.
The diagnosis is clinical, and requires a hx of chronic daily headache with analgesic use more than 2-3d per week.
The diagnosis of MOH is supported if headache frequency increases in response to increasing medication use, and/or improves when the overused medication is withdrawn.
The headache may improve transiently with analgesics and returns as the medication wears off. The clinical improvement after wash out is not rapid however, patients may undergo a period where their headaches will get worse. This period could last in the order of a few months in some cases.
The meds can be dc’d cold turkey or tapered depending on clinical scenario.
Greatest in middle aged persons. The prevalence rages from 1% to 2% with a 3:1 female to male ratio.
Migraine is the most common associated primary headache disorder.
** Each medication class has a specific threshold.
Triptans, ergot alkaloids, combination analgesics, or opioids on ten or more days per month constitute medication overuse.
Use of simple analgesics, including aspirin, acetaminophen and NSAIDS on 15 or more days per month constitutes medication overuse.
Caffeine intake of more than 200mg per day increases the risk of MOH.
Consider MOH in patients in the appropriate clinical scenario as sometimes doing less is more!
Historically uncuffed endotracheal tubes were used in children under the age of 8 years due to concerns for tracheal stenosis. Advances in medicine and monitoring capabilities have resulted in this thinking becoming obsolete. Research is being conducted that is showing the noninferiority of cuffed tubes compared to uncuffed tubes. Multiple other studies are looking into the advantages of cuffed tubes compared to uncuffed tubes.
The referenced study is a meta-analysis of 6 studies which compared cuffed to uncuffed endotracheal tubes in pediatrics. The pooled analysis showed that more patients needed tube changes when they initially had uncuffed tubes placed. There was no difference in intubation duration, reintubation occurrence, post extubation stridor, or racemic epinephrine use between cuffed and uncuffed tubes.
Bottom line: There is no difference in the complication rate between cuffed and uncuffed endotracheal tubes, but uncuffed endotracheal tubes did need to be changed more frequently.
Selective serotonin reuptake inhibitors are the most common anti-depressant used today. However, the use bupropion in adolescents is increasing due the belief that it has fewer side effects than TCAs.
Using the National Poison Data System (2013 – 2016), the adverse effects of bupropion were compared to TCA in adolescents (13 – 19 years old) with a history of overdose (self harm).
Common clinical effects were:
TCA: n=1496; Bupropion: n=2257
| Clinical effects | TCAs | Bupropion |
| Tachycardia | 59.9% | 70.7% |
| Drowsiness/lethargy | 51.5% | 18.1% |
| Conduction disturbance | 22.2% | 15.6% |
| Agitation | 19.1% | 16.4% |
| Hallucination/delusions | 4.2% | 23.9% |
| Seizure | 3.9% | 30.7% |
| Vomiting | 2.7% | 20.0% |
| Tremor | 3.7% | 18.1% |
| Hypotension | 2.7% | 8.0% |
| Death | 0.3% | 0.3% |
Conclusion:
Bupropion overdose results in significant adverse effects in overdose; however, death is relatively rare.
Bottom Line: Consider using pre-procedural ultrasound-assistance for all lumbar punctures.
Noninvasive Ventilation in De-Novo Respiratory Failure
Retrospective chart review at a headache clinic seeing adolescent concussion patients
70.1% met criteria for probable medication-overuse headache
Once culprit over the counter medications (NSAIDs, acetaminophen) were discontinued,
68.5% of patients reported return to their preinjury headache status
Take home: Excessive use of OTC analgesics post concussion may contribute to chronic post-traumatic headaches
If you suspect medication overuse, consider analgesic detoxification
Hyperoxia has been repeatedly demonstrated to be detrimental in a variety of patients, including those with myocardial infarction, cardiac arrest, stroke, traumatic brain injury, and requiring mechanical ventilation,1-4 and the data that hyperoxia is harmful continues to mount:
Bottom Line: Avoid hyperoxia in your ED patients, both relatively stable and critically ill. Remove or turn down supplemental O2 added by well-meaning pre-hospital providers and nurses, and wean down ventilator settings (often FiO2). A target SpO2 of >92% (>88% in COPD patients) or PaO2 >55-60 is reasonable in the majority of patients.8
Providing naloxone to patients at risk for opioid overdose is now standard of care. A retrospective study evaluated the rate of naloxone obtainment after standardizing the process for prescribing naloxone in the emergency department and dispensing from the hospital outpatient pharmacy.
55 patients were prescribed naloxone. Demographics: mean age 48 years old, 75% male, 40% primary diagnosis of heroin diagnosis, 45.5% were prescribed other prescriptions.
Outcomes:
Barriers identified included lack of ED dispensing program, cost of medication, even though cost is minimal and can be waived, and likely multifactorial reasons why patients did not present to pharmacy as instructed.
Take Home Points:
Alcohol withdrawal syndrome is frequently treated with benzodiazepines following CIWA-Ar (Clinical Institute Withdrawal Assessment of Alcohol scale). There are other medications that are used as either second line or as adjunctive agents along with benzodiazepines. A retrospective study compared the clinical outcomes between phenobarbital vs. benzodiazepines-based CIWA-Ar protocol to treat AWS.
The primary was ICU length of stay (LOS); secondary outcome were hospital LOS, intubation, and use of adjunctive pharmacotherapy.
Study sample: 60 received phenobarbital and 60 received lorazepam per CIWA-Ar.
Phenobarbital protocol:
Results
|
| Phenobarbital | CIWA-Ar |
| ICU LOS | 2.4 days | 4.4 days |
| Hospital LOS | 4.3 days | 6.9 days |
| Intubation | 1 (2%) | 14 (23%) |
| Adjunctive agent use | 4 (7%) | 17 (27%) |
Conclusion
Phenobarbital therapy appears to be a promising alternative therapy for AWS. However, additional studies are needed prior to adapting phenobarbital as first line agent for AWS management.
Diplopia can be a challenging complaint to address in the ED. Although not all patients will require imaging, use the simplified table below to help guide the imaging study needed:
| Clinical Situation | Suspected Diagnosis | Imaging Study | |
| Diplopia + cerebellar signs and symptoms | Brainstem pathology | MRI brain | |
| 6th CN palsy + papilledema | Increased intracranial pressure (e.g. idiopathic intracranial hypertension or cerebral venous thrombosis) | CT/CTV brain | |
| 3rd CN palsy (especially involving the pupil) | Compressive lesion (aneurysm of posterior communicating or internal carotid artery) | CT/CTA brain | |
| Diplopia + thyroid disease + decreased visual acuity | Optic nerve compression | CT orbits | |
| Intranuclear ophthalmoplegia | Multiple sclerosis | MRI brain | |
| Diplopia + facial or head trauma | Fracture causing CN disruption | CT head (dry) | |
| Diplopia + multiple CN involvement (3,4,6) + numbness over V1 and V2 of trigeminal nerve (CN5) +/- proptosis | Unilateral, decreased visual acuity | Orbital apex pathology | CT orbits with contrast |
| Uni- or bi-lateral, normal visual acuity | Cavernous sinus thrombosis | CT/CTV brain | |
C.N.: cranial nerve
A few (out of 10) tips for the care of sick patients with liver failure: