ICU admission rates for all acute PEs vary wildly across the country (<5% to ~80%).
To predict which hemodynamically stable, normotensive PE patients should be admitted to the ICU, a single-center retrospective analysis of 7 years’ data sought to describe the reasons why normotensive patients with PE required vasopressors within 48 hours of admission to the ICU. The authors studied 293 patients admitted to the ICU at Beth Israel Deaconess in Boston and found only 8 patients (2.7%) who decompensated within the first 2 days. Of MANY variables studied, only respiratory rate was significantly different between those who decompensated and those who did not (mean RR 29 with range 26-32 in the decompensated group vs mean 21 with range 17-24).
Bottom Line: cost control experts may lean on you to admit fewer PE patients to the ICU. There is no perfectly reliable way to predict which normotensive patient with a PE will decompensate. The PESI score has been validated but even the low risk cohort had 1.6% mortality at 3 days. The BOVA score has been validated but its endpoint of mortality at 30 days is less useful for planning admission. Tachypnea should concern you.
The Critically Ill Geriatric Patient with Sepsis
Synthetic turf playing surfaces have been growing in popularity over the last decade and seem to have become a new standard.
Due to the need for durable fields that can accommodate multiple teams/activities, in addition to the high cost of maintaining grass and the need to conserve water, many parks and schools have switched from grass to turf. Turf is advertised as maintenance free but ….this is not the case.
Locally, at M&T Bank Stadium, groundskeepers drive a LitterKat turf sweeper across the field for 4 hours 2-3 times a week to ensure that the synthetic rubber is cleaned and distributed evenly. The field is also repainted every 4 games because the paint may become hard. The cost of this level of maintenance is beyond what many parks and local high schools can afford.
A recent study examined high school concussion data at almost 2000 high schools with over 14,000 recorded concussions. Researchers concluded that more concussions occurred in games than practices. Interestingly, they also found that playing surface was significantly associated with concussion. Almost 90% of all injuries occurred on turf-based surfaces. Turf outweighed all other mechanisms of injury, including helmet-to-helmet hits and grass playing surface. Between 10 and 15.5% of concussions occur from helmet to ground contact. In the NFL, this mechanism accounts for about 1 in 7 concussions.
Attempting to limit total exposure time in practice and games on turf surfaces may be beneficial until more study is needed.
The rate of suicide attempt has been increasing over the past decade. A recently published article investigated the temporal trend of suicide attempts in adolescent/young adult population (10 – 25 years old) from 2000 to 2018.
Methods
Results
Top 5 substance involved in suicide attempt
Agents associated with serious medical outcome (after 2011)
Conclusion
Rationale: Data regarding temperature management in patients suffered from cardiac arrest with nonshockable rhythm was inconclusive.
Objective: whether moderate hypothermia at 33C, compared with normothermia at 37C would improve neurologic outcome in patients with coma after cardiac arrest with nonshockable rhythm.
Outcome: survival with favorable 90-day neurologic outcome (Cerebral Performance Category scale 1-2/5)
SummaryThere was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
This randomized multicenter trial involved 581 patients with cardiac arrest and nonshockable rhythm. Hypothermia group included 284 patients vs. 297 in the normothermia group. Median GCS at enrollment = 3.
Majority of patients was cooled with the use of a basic external cooling device: 37% for hypothermia and 50.8% for normothermia group.
There was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
Limitation:
A. The study used strict enrollment criteria:
B. normothermia group had higher proportion of patients with temperature at 38C.
C. Hypothermia group underwent temperature management of 56 hours vs. 48 hours for normothermia patients.
Take home points:
In a selected group of patients with cardiac arrest and nonshockable rhythm, moderate hypothermia at 33C may improve neurologic outcome.
E-cigarette (vaping) use has become increasingly popular over the past 10 years, especially among adolescents. Intentional exposure (i.e. ingestion in self harm) of nicotine (e-cigarette liquid) can be life threatening where it can produce mixture of stimulatory (early), cholinergic toxicity and muscle paralysis/respiratory failure by blocking the neuromuscular junction. However, the severity of clinical toxicity in unintentional exposure can vary widely depending on the dose/route/circumstance of their exposure.
A recently published study investigated the characteristics of e-cigarette liquid exposure between Jan 1, 2010 to Dec 31, 2018 using the National Poison Data System
Result
Top 4 clinical/demographic characteristics are listed below.
Age group:
Route of exposure
Level of care:
Clinical effects - overall
In <5 years group
Conclusion
Blood Transfusion Thresholds in Specific Populations
Sepsis - 7 g/dL
Acute Coronary Syndrome - no current specific recommendations pending further studies
Stable Cardiovascular Disease - 8 g/dL
Gastrointestinal Bleeds
Acute Neurologic Injury - Traumatic Brain Injury - 7 g/dL
Postpartum Hemorrhage - 1:1:1 ratio strategy
Intersection Syndrome
De Quervain’s is a common tenosynovitis is involving the the 1st dorsal compartment of the wrist/forearm.
Intersection syndrome is a tenosynovitis that occurs at the intersection of the 1st and 2nd dorsal compartments.
Pathology located at crossing point of the 1st compartment structures (APL and EBP) with the radial wrist extensors (ECRB and ECRL)
Occurs most commonly from repetitive wrist extension and is common in rowers, weight lifters, and in those playing racquet sports.
Occurs about 4 to 6cm proximal to the radiocarpal joint VERSUS De Quervain’s which occurs near the level of the radial styloid.
Pain worse with resisted wrist and thumb extension
Radiographs not required
Splint and start NSAIDs
Recalcitrant cases can be referred for corticosteroid injection
https://stemcelldoc.files.wordpress.com/2012/09/intersection-syndrome-referral-pain-pattern1.jpg
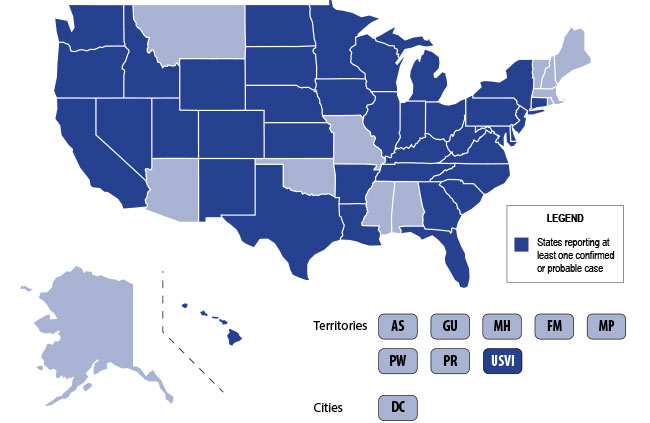
The U.S. is currently experiencing an epidemic of a severe lung disease termed Vaping-Associated Pulmonary Illness (VAPI), with over 500 cases and 7 deaths across 38 states and 1 U.S. territory since July 2019.
The clinical presentation of VAPI varies --
Diagnostics --
Treatment is supportive +/- steroids --
Bottom Line: Include vaping-associated pulmonary illness in your differential for patients presenting with acute lung disease.
- Tibial tubercle avulsion fractures are rare and pediatrics, accounting for less than 3% of all epiphyseal injuries in children ages 11-17 years.
- The typical mechanism is a sudden forceful quadriceps contraction. Patients present with sudden pain after sprinting or jumping with pain, bruising, deformity or swelling over the tibial tubercle and with a decrease ability to extend the leg.
- 10 to 20% of cases result in anterior compartment syndrome related to the rupture of the anterior tibial recurrent artery.
- Although directly measured intra-compartmental pressures can facilitate the diagnosis of compartment syndrome, interpretation of these values can be challenging with healthy children having higher average lower leg compartment pressures than adults. Treatment of subsequent compartment syndrome is often based on a high index of suspicion.
Cannabinoid hyperemesis syndrome [CHS] (i.e. cyclic/recurrent nausea, vomiting and abdominal pain) is associated with long-term and frequent use of marijuana. Patients with CHS often report temporary relief of symptoms with hot water/shower exposure. Emergency room providers may encounter a growing number of patients with CHS with increasing legalization of marijuana-containing products.
Topical capsaicin has been gaining interest as a potential adjunct to the conventional management of patients with CHS (e.g. antiemetics, opioids, benzodiazepines and antipsychotics).
A small retrospective study was performed involving 43 patients who had multiple visits, and were treated with and without capsaicin. The primary outcome was the ED length of stay (LOS).
Results
Conclusion
Most non-OB physicians experience some fear or anxiety over taking care of the average pregnant patient. There are two patients to consider when caring for these women. Critical illness adds another layer of complexity to an already challenging patient population. Due to the normal physiologic changes that occur during pregnancy there are specific and important factors to be aware of when considering and preparing for intubation.
Imaging of Lisfranc Injuries
Tarsometatarsal fracture-dislocation
Anatomy
3 Columns of the midfoot, divided by the tarsometatarsal joints
The Lisfranc ligament
- Extends from the 2nd MT to the medial cuneiform
- Critical to structure and stabilization of the 2nd MT and the midfoot arch
Imaging
Plain films: AP/lateral/oblique
Consider weight bearing view with contralateral comparison if high suspicion
CT: Can be useful to confirm abnormal plain films
MRI: not done in ED but can be used to diagnose pure ligament injuries
Below is a review of the lines of the foot which will ensure not missing this diagnosis. May be helpful to review with sample imaging.
Plain films findings: https://prod-images.static.radiopaedia.org/images/49189279/86408d5bae08ab80ae9ef377337ab7_big_gallery.jpeg
On AP view:
On Lateral view:
On the Oblique view:
Remember that the lateral margin of the 5th MT can project lateral to the cuboid (up to 3 mm)
Lines drawn on 2 view foot for review
https://radiopaedia.org/cases/lisfranc-ligament-normal-alignment
Question: In febrile children younger than 2 years, what combination of clinical and laboratory variables best predicts the probability of a urinary tract infection?
Given that urinary tract infections (UTI) are the most common source of serious or invasive bacterial infections in young febrile infants, early identification and treatment has the potential to reduce poor outcomes. Wouldn't it be great if there was an easy way to identify patients at highest risk?
Researchers from the Children’s Hospital of Pittsburgh formulated a calculator (UTICalc) that first estimates the probability of urinary tract infection (UTI) based on clinical variables and then updates that probability based on laboratory results.
Bottom line:
The UTICalc calculator can be used to guide to tailor testing and treatment in children with suspected urinary tract infection with the hope of improving outcomes for children with UTI by reducing the number of treatment delays.
Go ahead and give it a click!! https://uticalc.pitt.edu/
Breath analyzers are commonly used by law enforcment officers to test for alcohol intoxication. Breath analyzer uses ethanol partition ratio between blood:breath of 1:2100 = 1 gm of ethanol in 2100 mL of breath/air.
Mouth wash products are frequently used for oral hygiene, and at times, to "mask" odor of substances. These products are readily available in any grocery stores or pharmacy and contain upto 26.9% ethanol (e.g. Listerine) (18.9% - Scope; 14.0% - Cepacol).
Recently, a small study using healthy volunteers (n=11) was published to investigate the impact of limited ethanol exposure (mouth wash and ethanol vapor) on the breath-alcohol concentration (BrAC).
Method
Results
Blood: No or very low levels of ethanol (0.002 mg/g) were detected in blood at all collection time for both exposures.
BrAC - first collection -- seconds after exposure
Mean time to negative BrAC level (Swedish statutory limit of 0.1 mg/L = 0.01 mg/dL in air) (FYI: US limit = 80 mg/dL)
Conclusion
It's important to remember the differential for the patient with Ventricular Assist Device (VAD) difficulties, as these patients are likely to show up in your ED.
1) Assess the patient as you usually would (signs of life, mental status, breathing, arrhythmias on monitor, etc). Listen for a hum over the chest. Don't expect to feel a pulse.
2) Look at the VAD including controller, driveline, and power source for alarms, disconnections, signs of infection, and other obvious issues.
3) Look at the power (displayed flow), pulsatility index, and pump speed on the controller to help determine the cause of the issue (see attached chart). Once you have a suspected etiology, typical management of these issues is usually similar to non-VAD patients (i.e. gentle IVF for hypovolemia, vasodilators if low flow is due to afterload/hypertension, defibrillation/CPR for arresting pts, etc).
Don't forget to call your VAD coordinator when able. Consider a-line placement for precise evaluation of blood pressure (focus on MAP).
Bottom Line: Consider obstruction/thrombosis, bleeding, infection, hypovolemia, afterload/hypertension, arrhythmia, worsening LV function, and suction events when troubleshooting VADs. The power, pulsatility index, and pump speed help differentiate these conditions.
Droperidol is a butyrophenone with primary action as a dopamine D2 receptor antagonist. Historically, it has been used to treat a variety of conditions from nausea and headaches to acute agitation. In 2001, the FDA issued a black box warning for risk of cardiac arrhythmias. Following this warning, droperidol was on national shortage for several years, further limiting its use.
Several months ago, droperidol returned to the US market and is available at some institutions. Below is a refresher on dosing and monitoring. Similar to haloperidol, droperidol can cause extrapyramidal symptoms. Consider pre-treatment with diphenhydramine.
Dosing Recommendations:
Nausea and vomitting: 1.25 mg IV
Headache: 2.5 mg IV, 5 mg IM
Acute agitation: 5mg IM/IV
QTc prolongation is still a concern, especially at higher doses. If using doses > 2.5mg, or using repeated doses, obtain an ECG to ensure safe use of this medication. If the QTc is greater than 440 msec for males or 450 msec for females, droperidol is not recommended. There is little data regarding the risk with lower doses. Utilize clinical judgement and assess patient risk factors.
Numerous different household products can potentially be misused/abused. One such product is whipped cream charger/propellant that contains nitrous oxide.
Acute toxicity produce dose dependent response
Chronic toxicity causes myeloneuropathy (demyelination of the dorsal and lateral columns of the spinal cord) due to vitamin B12 deficiency
Management
{kind=link}
{kind=link}