The recent Baltimore City Marathon served as a nice reminder in a few cases that long-distance running and other ultra-endurance events can produce elevations in troponin levels. To review the non-cardiac-disease causes of troponin elevations:
sepsis, PE, COPD, carbon monoxide, intracranial abnormalities (including SAH, stroke, IC hemorrhage, seizures), ESRD, rhabdomyolysis, eclampsia and preeclampsia, extreme endurance exercises, UGI bleeding, LVH, catecholamine toxicity
Reimburshment Pearls:
Often charts are down coded as it is not clear from the documentation that your medical decision making was complex.
For instance, if your final diagnosis is GERD, and you do not document that you were also concerned about angina or a pneumothorax your level 5 chart could be coded as a level 3, since the final diganosis does not seem that complex. In order to prevent this document:
I realize that when you are busy this might be the last thing on your mind, but the difference between a level III chart and a level V chart is about $100, and the only additional work is the 3 minutes it would take to document what you did for the patient.
More to come...
While it is often ok to defer removal of pesky nasal foreign bodies until ENT follow up, if the foreign body may be a button battery, emergent identification and removal is indicated.
Damage can occur in 3 hours, and by 24 hours, near complete necrosis of turbinates and ala has been described.
A 34 y/o m presents to the ED agitated and combative with the following vitals signs: T 104.6, P 136, BP 198/124. His urine toxicology screen is positive for amphetamines.
Damage Control Resuscitation
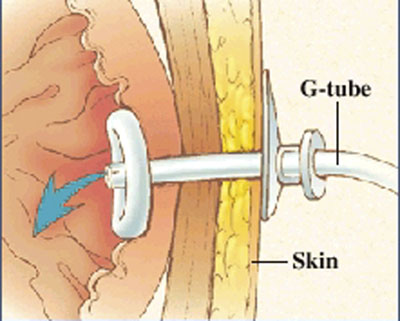
I am sure everybody has received a patient from a nursing home that had a malfunctioning PEG tube. Now if they would only crush the tablets before putting them down the tube, or better yet use liquid medications our life would be easier.
But what do you do if it is Friday and the GI lab is not open to Monday. The answer is that you can remove the PEG and replace it with another PEG tube or even a foley catheter will do for the weekend. The original PEG tube has a semi-rigid plastic ring (as shown in photo) and does not have a balloon that can be default. You can pull these out by placing counter traction on the abdominal wall and pulling with steady firm pressure. This may take a little more force than you are initially comfortable with.
Please see the attached photo of a PEG tube, and remember the other option is to admit these patients for IV fluids until the GI lab opens.
While breastfeeding is still the preferred source of infant nutrition by the AAP, a little-known fact is that breastfeeding may expose the nursing infant to environmental pollutants to which they might not normally be exposed. If you have a mother that appears ill due to exposure to any of these agents, don't forget to have the infant examined as well for signs of intoxication.
Severe mitral regurgitation (MR) after MI, accompanied by cardiogenic shock carries a poor prognosis.
Severe MR in many cases is due to infarction of the posterior papillary muscle, and in these cases the area of infarction tends to be less extensive than in those with MR due to severe left ventricular dysfunction.
Take Home Pearl:
The presence of pulmonary edema and/or cardiogenic shock in a patient with an inferior STEMI should prompt consideration for acute MR due to papilary muscle rupture. Get an echo as fast as you can to confirm or r/o the diagnosis. Treatment is afterload reduction, inotropic support, and urgent surgical repair.
Don't forget about pheochromocytoma as a possible cause of severe hypertension...especially in those patients that are recalcitrant to "normal" medications. A few important points:
1. Incidence may be as high as 0.2% of patients with hypertension...sounds very rare, but statistically we'll all see some during our career.
2. Mortality may be as high as 10% if unrecognized; but if recognized and treated, excellent prognosis.
3. Suspect this in patients with intermittent episodes of flushing, palpitations, diaphoresis, headaches, and hypertension.
4. Treatment with beta blockers alone (including labetalol) may induce unopposed alpha-activity and worsen BP.
5. Treat with nitroprusside or phentolamine (an alpha blocker). Phentolamine is 5 mg IV, can be repeated every 5-10min as needed.
6. After phentolamine is given, there may be reflex tachycardia. NOW you can add beta blockers.
The most important thing is to keep the diagnosis in mind. It's out there! But you'll miss 100% of the diagnoses you don't consider.
AC Joint Dislocations
The acromioclavicular (AC) Joint is commonly injured when a person falls onto their shoulder.
The AC Joint consists of three ligaments:
Injuries to this joint are classified as Type I – Type VI and involve sprain or tears of the AC or CC ligaments
Aripiprazole (Abilify): a new atypical antipsychotic partially agonizes D2 and serotonin receptors though its compelte mechanism is not known. Used in schizophrenia, in overdose you may see the following symptoms (from a retrospective study done over 4 years worth of calls to a PCC):
The study was with over 255 patients. Though QT prolongation is listed, it is not common with this medication.
Mechanically Ventilated ED Patients and Secretion Mobilization
Herpes Encephalitis-When to Consider
Herpes encephalitis is a potential lethal condition with high morbidity. Obviously our job in the ED is to rule-out bacterial meningits. So, when should we consider the diagnosis of herpes encephalitis?
Although no great guidelines exist, consider ordering a herpes PCR when sending studies on the "rule-out meningitis" patient. What about emperically treating a patient with Acyclovir? Again, no great data. Consider treating with 10 mg/kg IV q 8 hours for patients with abnormal CSF (in addition to the Ceftriaxone/Vanc, etc.) if you are worried about them, if they are altered (or encephalopathic), and if the CSF is abnormal (elevated wbc) with a negative gram stain. Acyclovir can always be discontinued when the PCR returns negative.
Systemic lupus erythematosus produces a significant predisposition towards premature atherosclerosis. Although the exact mechanism for what causes this is uncertain, premature CAD is at least partially (or largely) caused by systemic inflammation, which can produce endothelial damage and initiates the process of atherogenesis.
The literature indicates that there is a 9X increased risk of CAD in patients with lupus, and the risk increases to 50X higher in women 35-44 years of age! In general, patients with lupus develop their first MI 20 years earlier than age-matched non-lupus counterparts.
[Mattu A, Petrini J, Swencki S, et al. Premature atherosclerosis and acute coronary syndrome in systemic lupus erythematosus. Am J Emerg Med 2005;23:696-703.]
Beware of your online contributions, they can come back to hurt you in legal settings. You must remember that there is a digital trail of everything you post online. Discovery rules vary state to state. It is best to practice save surfing. What you may perceive as paranoia is really just good practice.
The following guidelines apply to:
General guidelines
Assume that whenever you hit send, your message will be available to a plaintiff attorney who will twist it to suit his/her needs. The only potential exception is direct email communication to your personal legal counsel. Please verify that local laws protect this form of communication before making an assumption of privacy.
[This pearl is a review of published general recommendations on privacy practices and should not be interpreted as, or replace competent legal advice.]