Bleeding Dialysis Fistula?
Ever see a patient in the ED c/o "my fistula won't stop bleeding"? If you haven't, you probably will in the future.
Here are some helpful tips on getting these bad boys to stop oozing:
Impingement Syndrome and the Diagnostic Accuracy of 5 Common Tests
It is also reported that subacromial impingement syndrome (SAIS) is the more frequent cause of shoulder pain.
The authors of this study attempted to determine the diagnostic accuracy of the following 5 tests for SAIS:
The study demonstrated that any 3 positive tests out of the 5 has a sensitivity of 0.75 (0.54-0.96) , specificity of 0.74 (0.61-0.88), positive likelihood ratio of 2.93 (1.60-5.36) and negative likelihood ratio of 0.34 (0.14-0.80). See the table below for the individual test characteristics. No single test was deemed accurate enough to make the diagnosis by itself.
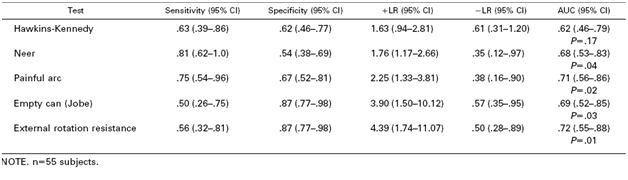
So in the end you should be familiar with most of these tests in order to use a combination of them to make the diagnosis of impingement syndrome. Future pearls will review how to perform these tests.
With all of the post-transplant patients we see in the ED, a refresher on the toxicities associated with the most common immunosuppressant medications is warranted.
Cyclosporine (Sandimmune® and Neoral®/Gengraf®) and tacrolimus (Prograf®) are both calcineurin inhibitors that inhibit activation and proliferation of T-lymphocytes and IL-2.
- Major concerns: Nephrotoxicity, drug interactions (CYP3A4)
- Adverse Effects:
o Electrolyte abnormalities: K+, ¯Mg+, glucose
o CNS: HA, tremor (statistically higher with tacrolimus)
o CV: HTN, lipids (increased with cyclosporine)
o End organ: hepatotoxicity, nephrotoxicity
o Cosmetic (cyclosporine specific): hirsutism, gingival hyperplasia, acne
Sirolimus/Rapamycin (Rapamune®) is an M-tor inhibitor that inhibits T-lymphocyte activation and proliferation.
- Major concerns: Drug interactions (CYP3A4)
- Adverse Effects:
o Delayed wound healing
o Leucopenia, thrombocytopenia
o Hypercholesterolemia
There are several conditions that alter ionized calcium levels, including:
The bottom line is to measure ionized calcium, and consider all other factors that can be contributing to hypocalcemia in addition to repleting it.
Altered Mental Status-Does Your Patient Have Non-Convulsive Status Epilepticus?
Ever intubated a patient in status epilepticus and wondered if they were still seizing after sedation and paralysis? Ever taken care of an altered patient and wondered if you should consult neurology and attempt to get an EEG?
NCSE is defined as continuous seizure activity without obvious outward manifestations of a seizure. This is important for emergency physicians to consider because it has to be detected early to prevent morbidity and mortality.
When to consider NCSE:
Scaphoid Fractures:
For suspected scaphoid fractures with negative radiographs it is common practice to put a person in a short arm thumb spica splint until followup up radiographs can be obtained in 10-14 days.
However, there is evidence that a short arm thumb spica splint is not enough for people that have a true scaphoid fracture. Gellman et al demonstrated that long arm thumb-spica cast immobilization for six weeks followed by short arm thumb-spica cast immobilization decreased time to union by 25% when compared to short arm thumb-spica casting alone.
The theory is that the short arm splint still allows for forearm rotation that can cause shearing motion of the volar radiocarpal ligaments. A long arm splint prevents this shearing action. The disadvantage of a long arm splint though is potential elbow joint stiffness and muscle atrophy that can occur during the prolonged period of immobilization.
So for your next patient with a scaphoid fracture seen on radiographs place them in a long arm thumb spica splint.
CARBAPENENEMS
TIGECYCLINE
AMIKACIN
COLISTIN
The Rapid Ultrasound in Shock (RUSH) Exam
Pulmonary Embolism-Myths and Misconceptions
Just wanted to mention a few myths/misconceptions about acute PE that I have recently heard discussed in the ED.
1. Emergency physicians have to "get help" to give thrombolytic therapy. Sure it makes sense that we consult critical care and perhaps interventional radiology in some cases. But we do not need permission to use this drug by ourselves if indicated. Consider using lytics ESPECIALLY if the patient is unstable or if there is evidence of RV dysfunction (elevated troponin, echo criteria for dysfunction, or CT with large RV and bowing of the septum). What about the patient with RV dysfunction and a normal BP? Evidence is mounting that lytics are indicated to reduce the severity of pulmonary hypertension.
2. "Just get a d-dimer." Be very careful. Lots of false positives. D-dimer often clouds the picture more often than not.
3. "The mortality rate of missed PE is high." Often quoted as a 30%+ mortality rate if missed. Recent data suggests that it is < 5%.
Missed cases of ACS account for 10% of all malpractice cases in emergency medicine, yet account for 30% of all the money emergency physicians pay out in malpractice cases. This misdiagnosis is the biggest cause of monetary payout in the specialty.
Three main themes account for the majority of missed cases of ACS:
1. Failure to recognize atypical presentations (e.g. dyspnea)
2. Failure to recognize high-risk groups (e.g. women, diabetics)
3. Over-reliance on negative tests (e.g. negative troponin or recent stress test)
Temporal Arteritis (TA) is commonly associated with the sudden onset of a unilateral headache centered around the temporal region. The most devastating consequence of TA is blindness though this is only reported in up to 50% of cases though can be bilateral in up to 33% of patients.
According to the American College of Rheumatology criteria for classification of temporal arteritis this diagnosis can be made in the ED without a biopsy. You just need at least 3 of the following 5 items to be present (sensitivity 93.5%, specificity 91.2%) to make the diagnosis :
The umbilical site normally heals by 1 month of age.
Any fluid draining after this period suggests an abnormal connection between the surface of the abdomen and the underlying structures, and requires further investigation. Clear yellow fluid could represent a persistent connection of the bladder with the umbilicus called a patent urachus. The fluid that leaks is actually urine. The treatment is surgical closure of the connection.
Pus oozing from the umbilical stump would imply infection, especially if there is concomitant redness of the skin around the umbilicus. An omphalitis can be life-threatening, and requires admission for invtravenous antibiotics.
Umbilical hernias are common in infants, and are usually noted with diastasis of the rectus muscles. Most umbilical hernias resovle by school age, and do not require surgical intervention.
An umbilical granuloma is a small piece of bright red, moist flesh that remains in the umbilicus after cord separation. It is scar tissue, usually on a stalk, that did not become normally covered with skin cells. It contains no nerves and has no feeling. Most can be simply cauterised with silver nitrate.
Radiocontrast Induced Nephropathy (RCIN)
Patients in the Critical Care setting may develop HIT as a result of chronic pre-existing risk factors (malignancy, obesity, hypertension, diabetes or medications) or acquired factors secondary to their ICU stay (post-operative state, trauma, central lines or medications such as heparin).
Diagnosis of HIT:
Treatment of HIT:
Can you use a serum d-dimer to rule out aortic dissection?
The answer to the question, in 2010, is no.
There has been a flurry of recent literature about the use of serum d-dimer to rule out aortic dissection. Some studies have shown a sensitivity of nearly 100%, but other studies have shown sensitivities of only 60-70%....pretty abysmal sensitivities. And despite some of the authorities on the subject touting how good the test is, there is not firm literature to support it. Better yet, there are some active medical malpractice cases I am aware of in which the diagnosis of aortic dissection was missed based on a "negative d-dimer."
My suggestion, and the vascular pearl for the day, is to avoid using d-dimer as a aortic dissection rule out strategy until good evidence (if it ever becomes available) exists. I know that people are using this test to rule out the disease, just realize that EVERY time I have ever given a talk on acute aortic disasters, 2-3 people from the audience always share that they had a case of a "d-dimer negative dissection."
Be careful....
Women are more likely to be misdiagnosed than men when they present with acute coronary syndromes. There are several possible reasons for this:
1. Women are more often older and more often have diabetes, both of which are factors involved in atypical presentations.
2. Women present with chest pain less often than men. On the other hand, women are more likely to present with nausea, vomiting, indigestion, malaise, loss of appetitie, or syncope than men.
3. When women do have chest pain, they are more likely to report pain that has atypical features, such as radation to the right arm or shoulder, front neck, or back; and the pain is more often described as sharp, stabbing, or tansient.
The bottom line is something that I've believed since high school: women are confusing...!
[the references for this ACS information comes from many different sources, but if anyone needs a good review on this topic, just email me: amattu@smail.umaryland.edu]