A 2020 meta-analysis attempted to estimate the frequency of radiographically occult hip fractures in the elderly population.
26 studies evaluated the rate of surgical hip fractures with no obvious findings on plain film.
Median age 80.3 years (67-82 years).
MRI used as gold standard.
The overall rate of radiographically occult hip fracture requiring surgery was 39%.
This percentage is higher than reported in other studies which may have included non-elderly patients, retrospective bias or other issues.
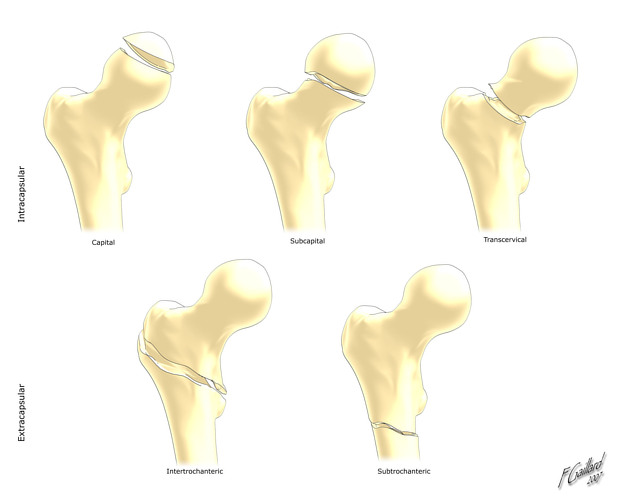
Overall, 18% had femoral neck fractures, 17% had intertrochanteric fractures and 1% had subtrochanteric fractures.
Elderly patients with acute hip pain and negative or equivocal findings with initial plain film imaging have a high frequency of occult hip fractures. Strongly consider advanced imaging in this population
Hip Fractures
Femoral neck and intertrochanteric fractures occur most commonly among patients aged 65 and over
Major risk factors for hip fractures include osteoporosis and falls.
Patients with a low body mass index (BMI <22) appear to be at higher risk
Isolated trochanteric fractures occur more often in young active adults
In-hospital mortality rates are approximately 5% (range 1-10%)
In addition to making the diagnosis and consulting orthopedic surgery, ED providers must remember to provide adequate analgesia as elderly patients are often under medicated.
-Up to 72% receive no prehospital analgesia.
Extracapsular fractures cause more pain than intracapsular fractures due to the greater degree of periosteal trauma.
Poor pain control predisposes hip fracture patients to delirium
Retrospective studies indicate that patients at higher risk for significant bleeding have at least 2 of the following risk factors:
Age over 75 years, initial Hgb below 12 g/dL and peri trochanteric fracture location.
A recent study attempted to investigate the relationship between a history of strength training with symptomatic and structural findings of knee osteoarthritis (OA).
For comparison, previous studies have shown that duration of football participation increases risk of radiographic knee OA.
Methods: Retrospective, cross-sectional multicenter study
2,607 participants without OA. Community population. 44% male. Mean age 64.3 years. Mean BMI 28.5.
Strength training (via self-administered questionnaire) defined as those exposed (n=1789 ) and not exposed (n=818). If exposed, groups were divided into low, medium and high.
Outcomes were 1) Radiographic OA. 2) Symptomatic radiographic OA. 3) Frequent knee pain
Results: Strength training at any point in life vs no strength training was associated with lower incidence of all outcome measures:
Odds ratio1) 0.82, 2) 0.83 and 3) 0.77.
Conclusions: Strength training is beneficial for future knee health
However, when separated by groups (low, medium and high), only the high-exposure group had significantly reduced odds of less frequent radiographic OA, symptomatic radiographic OA, and frequent knee pain.
Findings were similar for different age ranges
The association between strength training and less frequent radiographic OA, symptomatic radiographic OA, and frequent knee pain was strongest in the older age groups.
A recent study in Annals of EM investigated the use of topical Diclofenac in the treatment of lower back pain.
Small studies have shown topical NSAIDs to be effective for single joint OA and tendinopathies.
Currently, NSAIDs are first-line treatment for ED patients with acute low back pain.
Theoretically, topical NSAIDs deliver medications directly to the injured tissue while minimizing systemic side effects.
-Topical NSAIDs provide similar concentrations of the drugs in muscle tissue but much lower plasma concentrations than oral formulations
Design: Randomized, double-blind, placebo-controlled trial.
ED patients aged 18 to 69 years with non-radicular, non-traumatic acute lower back pain.
Screened 3,281 and enrolled 198.
Study groups:
Patients received 2 days of meds. Follow up by phone at 2 and 7 days.
Investigators used the RMDQ score to measures pain and functional impairment.
Results: At the 2 day follow-up, all 3 groups showed an improvement in the mean RMDQ score compared to baseline as expected.
Participants had a mean RMDQ improvement of 10.1 in the ibuprofen group, 6.4 in the diclofenac gel group, and 8.7 in the ibuprofen + diclofenac gel group.
At the 7-day follow-up, participants had a mean RMDQ change compared to baseline of 12.2 in the ibuprofen group, 9.5 in the diclofenac group, and 10.7 in the ibuprofen + diclofenac gel group.
Conclusion: This study does not support the use of topical diclofenac among patients who can otherwise tolerate oral ibuprofen.
Because the study did not compare placebo gel to topical Diclofenac, we cannot infer whether topical medication is helpful for treatment in acute lower back pain in those patients who may not be able to take NSAIDs.
Concussion Visits to the Emergency Department
In a study looking at concussion discharge instructions in the ED:
A 2020 study looked at patients aged 6-18 years diagnosed with concussion on either first or subsequent ED visit.
Those patients with delayed diagnosis required more medical visits during recovery, had a significantly longer time to symptom resolution (21 vs. 11 days), and had a higher likelihood of having persistent concussion symptoms.
Take home: Consider printed concussion discharge instructions in the appropriate ED patients as this has downstream benefits for health and recovery.
New progress in head injury prevention in football
A Guardian Cap is a soft padded soft shell worn over football helmets.
Think of it like a shock absorber
It is intended to mitigate energy transfer to the head and neck during player impacts.
It retails for about $70 on amazon!
https://www.pinkvilla.com/pics/855x855/236466742_untitled-design-2024-04-27t133219-626_202404.jpg
Most NFL players have worn these caps during preseason practices for the past 2 years.
The NFL found a 52% reduction in preseason concussions (at the same position) between players who wore the cap versus those who did not.
In laboratory testing the Guardian cap reduced head impact forces by up to 1/3rd in certain impacts.
Per NFL analytics, the Guardian cap absorbs 10% of the traumatic force.
Additionally, if two players suffer a helmet to helmet hit in which each wears the cap, the impact force is reduced by 20%!
The NFL has allowed players to wear the caps this year
They will have the team logos on them
2024 season: Players will wear the caps or one of 6 approved helmets (position specific) that provide equal or better protection.
If your child plays football, consider investing in this product as a potential means to reduce head impact forces and concussion.
More data is needed during regular season games with full speed collisions.
Metacarpal fractures are frequently seen in the ED.
These are frequently non operative injuries.
For 4th and 5th metacarpal fractures, consider an ulnar gutter spilt.
For 2nd and 3rd metacarpal fractures, consider a radial gutter splint.
Splinting position (Intrinsic plus):
Wrist in approximately 20 degrees of extension (position of function)
MCP joint in 70 to 90 degrees of flexion
Slight flexion at the DIP and PIP and DIP joints.
-Important to prevent shortening of the collateral ligaments
The OPAL trial attempted to investigate the effectiveness of opioids in the acute management of neck and back pain.
346 adults presenting to the Emergency department or primary care provider with 12 weeks or less of lower back pain, neck pain or both (of at least moderate intensity).
51% male. 49% female.
Location: Sydney, Australia
All participants received guideline care (advice to stay active, reassurance of a positive prognosis, avoidance of bed rest, and, if required, other non-opioid analgesics).
Patients were then randomly assigned to an opioid (oxycodone, up to 20 mg PO qD) or and an identical placebo, for up to 6 weeks*.
*Trial used a combination oxycodone/naloxone to reduce risk of opioid induced constipation and assist with blinding.
*Trial used a modified release formulation that could be dosed q12h rather than q4-6h to increase adherence.
*Recommended regimen was oxycodone 5mg every 12 hours, with titration as necessary, max dose 20mg total per day.
*Trial physicians were able to individualize the prescription to suit the patient’s needs.
* Mean prescribed dose was approx. oxycodone 10mg total daily.
*Most patients only treated for 2 weeks
Primary outcome: Pain severity at 6 weeks
Results: Mean pain score at 6 weeks was identical between groups.
Trend towards faster recovery in the placebo group in the first 2 weeks.
Take home: Consider the likely benefit vs harm of prescribing opioids for acute back and neck pain in the ED.
Acetaminophen and low back pain.
Acetaminophen has been a traditionally recommended first line intervention for acute low back pain.
Cochrane reviews in 2016 and 2023 found that acetaminophen showed no benefit compared to placebo in patients with acute low back pain.
A 2020 study investigated whether the addition of acetaminophen to short term NSAID therapy was beneficial.
A randomized double-blind study conducted in two urban emergency departments.
Patients randomized to a 1-week course of ibuprofen plus acetaminophen versus ibuprofen plus placebo.
Population: patients presenting with acute, non-radicular, non-traumatic lower back pain of fewer than two weeks duration.
Authors compared pain and functional outcomes at one week following discharge.
Conclusion: there was no outcome benefit from the addition of acetaminophen to ibuprofen.
Axial neck pain is a dull aching “soreness” pain from the posterior neck muscles with radiation to the occiput, periscapular and shoulder regions.
Associated with headaches, stiffness and muscle spasm.
Patients with cervical radiculopathy, however, usually present with unilateral pain discomfort.
Patients may complain of pain radiation into the ipsilateral arm. Though frequently difficult to describe, this may be in a dermatomal distribution. Patients may also report decreased sensation in a dermatomal distribution or weakness along the corresponding myotome.
The most affected nerve roots are C7 (C6-7 herniation), followed by C6 (C5-6 herniation) and C8 (C7-T1 herniation).
Cervical Spondylosis (degenerative change) is the most common ideology.
As discs breakdown with age and lose height, increased force loads are transmitted to bony regions of the spinal segment leading to bone hypertrophy which creates foraminal stenosis and resultant radiculopathy.
Cervical radiculopathy, like lumbar radiculopathy, is largely a self-limited condition. Several older studies following this diagnosis revealed that a majority of patients were either asymptomatic or mildly symptomatic at time of follow-up.
Improvement is seen over the initial four to six months following diagnosis.
Reducing musculoskeletal injury and concussion risk in schoolboy rugby players with a pre-activity movement control exercise programme: a cluster randomised controlled trial
Intro: Musculoskeletal injuries and concussion are prominent reasons for time loss from sport for adolescent rugby players.
Injury patterns in rugby differ from other team sports,
-Greater frequency of concussion, upper body and contact-related injuries
Increased concussion risk is associated with lower neck strength, highlighting this characteristic as a potentially modifiable risk factor.
Enhancing neck muscle strength may prevent concussion by improving the dissipation of impact forces transmitted to the brain.
The aim of study was to determine the efficacy of a movement control exercise program in reducing injuries in youth rugby players.
Methods: In a cluster-randomized controlled trial, 40 independent schools (118 teams, 3188 players aged 14-18 years) were allocated to receive either the intervention or a reference program, both of which were to be delivered by school coaches.
The intervention comprised balance training, whole-body resistance training, plyometric training, and controlled rehearsal of landing and cutting maneuvers. This also included a neck strengthening component.
Time-loss (>24 hours) injuries arising from school rugby matches were recorded by coaches and medical staff.
Results: When trial arm comparisons were limited to teams who had completed three or more weekly program sessions on average, clear reductions in overall match injury incidence (RR=0.28) and concussion incidence (RR=0.41) were noted in the intervention group.
Conclusion:
Wrist pain in golfers
70% of amateur golfers will experience a sport related injury in their lifetime.
The hand/wrist is the third most common body area injured by golfers after the back and elbow.
Studies fail to include multi trauma from golf cart accidents:)
Wrist injuries are 3x more frequent than hand injuries.
Wrist injury affects 13 to 20 percent of amateur golfers.
Injury is most likely to occur at the point of ball impact.
Injury most commonly affects the lead wrist rather than the trail wrist.
The lead wrist is left sided for right-handed players and right sided for lefties
Due to many differences in grip and wrist position there are several injury patterns.
Most causes of wrist pain in golfers are tendinopathies.
Due to impact stress and repetitive swinging movements
If pain is primarily radial, consider DeQuervain's tenosynovitis
Poor swing mechanics such as premature wrist uncocking in the early downswing places the wrist in ulnar deviation thereby stressing the first dorsal compartment.
Significant ulnar deviation of the lead wrist at time of ball impact may also stress the tendons of the first dorsal compartment.
If pain is primarily ulnar consider Extensor Carpi Ulnaris tendonitis & subluxation
A strong golf grip (more knuckle’s visible) is associated with greater ECU stress during the swing
The height of hand position can also stress the ECU tendon
Differential diagnosis:
TFCC injury
Hook of hamate fracture
Carpal Tunnel Syndrome
Ulnar Tunnel Syndrome
Estimating the size of knee effusions
While this size range is typically easily detectable on exam. This may not apply to patients who are either very muscular or obese.
If the detection of a small to moderate sized effusion would change patient management
Consider ultrasound:
As compared to MRI (sensitivity of 81.3 % and a specificity of 100 %)
https://prod-images-static.radiopaedia.org/images/626179/d58f35a8aa4a0a6750a6adce4087a4_gallery.jpg
"I was kicked in the inside of my knee while it was straight (extended). Look at the x-ray and tell me if its bad"
The objective of a recent study was to analyze the injury and illness characteristics in Iron Man distance triathletes. This information is important for emergency providers who may be asked to directly assist or help coordinate race day medical care.
Intro: The Iron Man distance triathlon is one of the most challenging ultra endurance competitions in the world. 80,000 Iron Man triathletes compete internationally each year to qualify for the Ironman world championship. The race totals 140.6 miles across three legs, beginning with a 2.4 mile swim, followed by a 112 mile cycle, and is completed with a 26.2 mile run.
Retrospective cross-sectional study of medical records from Iron Man distance championship races across a 30-year period (1989-2019). The study population (10,533) consisted of all triathletes treated at mobile medical units along the race route or who presented to the medical tent for evaluation during and immediately after the event.
Mean population age of 37 with a range of 18 to 87 years.
Results: Female athletes were found to present to the medical tent more than males (P < 0.001).
The total incidence of medical encounters by age was found to be higher in both younger athletes (18 to 34 years old) and older athletes (greater than 70 years old) versus middle-aged athletes (35-69 years old) (P < 0.001).
Professional athletes have similar overall medical encounters compared with other athletes.
The busiest hours of the medical tent were between approximately 9 and 14 hours after start time (afternoon and early evening) in which approximately 73% of athletes presented for evaluation and treatment.
Once inside the medical tent 71% of athletes were discharged within an hour and 87% were discharged within 1.5 hours. Athletes were dispatched to the hospital from the medical tent area at a rate of 17.1/1000 athletes (most athletes presenting to the medical tent finished the race and few required hospital transfer).
The most common medical complaints were dehydration and nausea followed by dizziness, exhaustion, muscle cramps, and vomiting.
Blood work was collected for 30% of athletes who entered the medical tent. Of these athletes, hyponatremia was the most prevalent diagnosis and most of whom were symptomatic with symptoms such as confusion, stupor, gait disturbance, muscle weakness, headache, dizziness, fatigue, nausea and vomiting.
Beyond basic medical care, intravenous fluids were the most common medical treatment.
Conclusion: Medical events were more frequent among female athletes as well as both younger and older age categories. Gastrointestinal and exertional related symptoms were the most common complaints in the medical tent. Besides basic medical care, IV infusions were the most common treatment. Most athletes presenting to the medical tent finished the race and only a small percentage were transferred to the hospital.
The role of exercise in patients with asthma is complicated.
Asthma symptoms can worsen or be triggered by physical activity. This can lead to avoidance response. Patients with asthma are less physically active than their matched controls.
Recently, however, the role of exercise and physical activity as an adjunct therapy for asthma management has received considerable attention. There is an emerging and promising role of physical activity as a non-pharmacologic treatment for asthma. Exercise reduces inflammatory cytokines and increases anti-inflammatory cytokines thereby reducing chronic airway inflammation.
Physical activity can help improve lung function and boost quality of life. As fitness improves, asthma patients report better sleep, reduced stress, improved weight control, and more days without symptoms.
The Global Initiative for Asthma recommends twice-weekly cardio and strength training. Strength training requires short periods of exertion allowing for periods of rest and recovery. High-intensity interval training (HIIT) is a promising option for people with asthma. These types of workouts allow ventilation to recover intermittently vs conventional cardio exercises.
A 2021 study in adults with mild-to-moderate asthma found that low volume HIIT classes (three 20-minute bouts/week) significantly improved asthma control. Patients also had improved exertional dyspnea and enjoyment of exercise which will, in turn, increase the odds of further exercise.
A 2022 study compared constant-load exercise versus HIIT in adults with moderate-to-severe asthma. Exercise training lasted 12 weeks (twice/week, 40 minutes/session). Both groups showed similar improvements in aerobic fitness however the HIIT group reported lower dyspnea and fatigue perception scores and higher physical activity levels.
Conclusion: Patients with asthma should be encouraged to safely incorporate exercise in their daily lives bother for overall health benefits but also as an effective non-pharmacologic asthma treatment.
Sport related concussion has been estimated to affect almost 2 million children and adolescents in the United states annually
Patients who take longer than four weeks to recover are considered to have persistent post concussive symptoms
This diagnosis is associated with poor educational, social and developmental outcomes in pediatric patients
Following sport related concussion, patients are recommended to have an individualized aerobic exercise program
Prior studies have found that sub symptom threshold aerobic exercise safely and significantly speeds recovery from sport related concussion.
Purpose: This study attempted to answer whether there is a direct relationship between adherence to a personalized exercise prescription and recovery or if initial symptom burden effects adherence to the prescription.
Design: Male and female adolescents aged 13 to 18 years old presenting within 10 days of injury and diagnosed with sport related concussion.
Almost all participants (94%) sustained concussion during interscholastic games or practices.
As it is known that physician encouragement can influence patient adherence to medical interventions, treating physicians in the study were blinded to study arm assignment.
Patients were given aerobic exercise prescriptions based on their heart rate threshold at the point of exercise intolerance on a graded treadmill test
Adherence to prescription was determined objectively with heart rate monitors. No participants exercised above their prescribed heart rate intensity.
Patients who completed at least 2/3 of their aerobic exercise prescription were considered to be adherent
Results: 61% of adolescents met the adherence criterion
Adherent patients were more symptomatic and were more exercise intolerant (worse initial exercise tolerance) at their initial visit.
These patients were also more adherent than those with fewer symptoms and with better exercise tolerance. This likely indicates a stronger motivation for those more symptomatic patients to engage in a potentially effective intervention.
Adherent patients recovered faster than those who were not adherent (median recovery time 12 days versus 21.5 days (P = 0.016)
Adherence during week one was inversely related to recovery time and to initial exercise tolerance but not to initial symptom severity
Conclusion: Adherence to individualized sub symptom threshold aerobic exercise within the first week of sport related concussion is associated with faster recovery. The initial degree of exercise intolerance (but not initial symptom severity) affects adherence to aerobic exercise prescription in an adolescent population with sport related concussion
29 yo baseball pitcher presents with right medial elbow pain. He felt a painful “pop” and could not continue to throw (due to loss of speed and control). Also notes mild paresthesias in 4th and 5th digits.
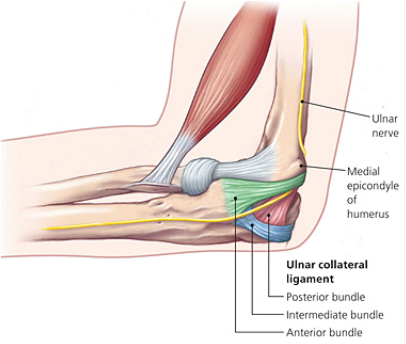
Ulnar collateral ligament (UCL) injury
Sprain of the UCL of the elbow can occur either as an acute injury or as the result of chronic excessive valgus stress due to throwing. This injury is seen in javelin throwers and baseball pitchers. Most recently, Angels superstar Shohei Ohtani suffered a torn UCL.
While traditionally this injury pattern was thought to occur in older, high-level pitchers (high velocity throwing), we are increasingly seeing this in younger athletes.
The repeated valgus stress of pitching leads to micro tearing and inflammation of the ligament. Over time, this leads to scarring and calcification and then ligament rupture.
This injury is more likely to happen in pitchers who “open up too soon” in their throwing motion. Fatigue related changes seen first in leg and core mechanics cause pitchers to open up earlier, increasing stress to the shoulder and the UCL of the elbow. Other risk factors include high velocity pitching, insufficient recovery time, and chronic overuse. The importance of proper pitching mechanics is very important as players whose pitching motion produces greater elbow valgus loads and shoulder external rotation torque are at increased risk for UCL tears.
Approximately one half of the torque generated during a fastball pitch is transmitted to the UCL. Well developed muscles about the elbow can dissipate enough energy that acute tearing is rare.
The athlete with a UCL sprain will complain of medial elbow pain that increases during the acceleration phase of throwing.
On examination, there is localized tenderness directly over the UCL:
http://www.texasshouldersurgeon.com/uploads/6/3/5/8/63580047/1446137856.png
Stress testing of the UCL causes both pain and demonstrates laxity.
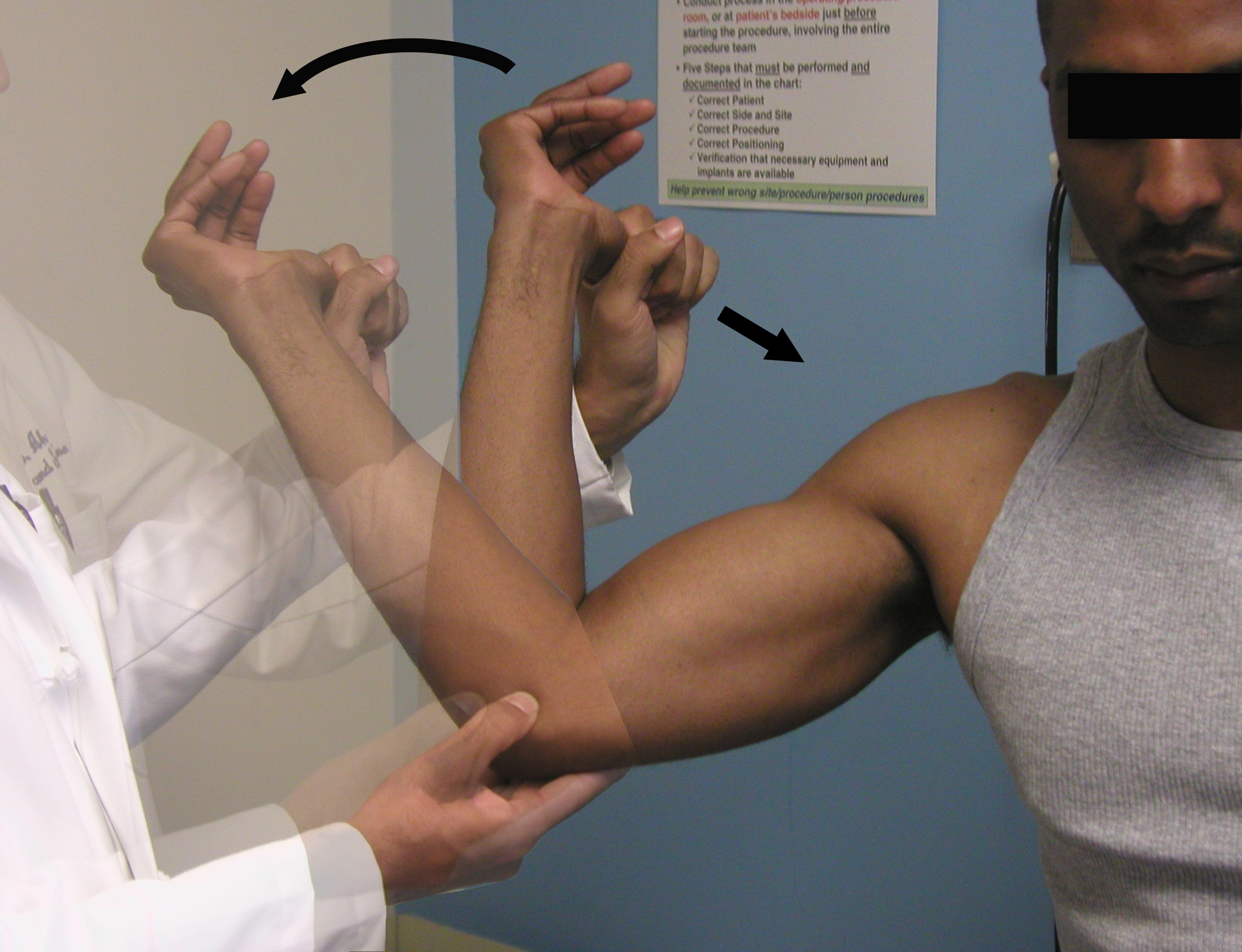
Moving Valgus Stress Test:
Place elbow in the “90/90” position. Apply a valgus stress while ranging elbow through full arc of flexion and extension. A positive test will reproduce apprehension, pain or instability at the UCL origin between 70 and 120 degrees.
https://www.youtube.com/watch?v=OnkkHpG3Dqg&ab_channel=RussHoff

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}