Category: Orthopedics
Keywords: knee pain, running injury (PubMed Search)
Posted: 3/25/2023 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Patellofemoral anatomy and disease (part 1)
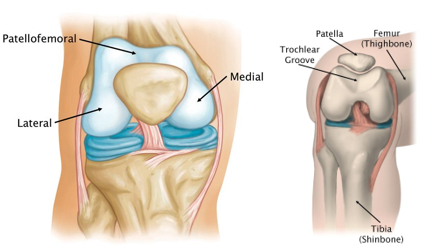
During normal knee flexion, the patella slides within the trochlear grove. Both (patella and the trochlear groove) are lined with articular cartilage at the patellofemoral articulation.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint2.jpg
Multiple forces act on the patella which can affect proper tracking: Proximately, by the quadriceps tendon, distally, by the patellar tendon, medially, by the medial retinaculum/vastus medialis and laterally by the lateral retinaculum and the vastus lateralis.
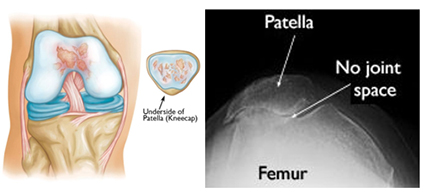
Patellofemoral OA can occur when this cartilage starts to wear and can be seen in skyline/sunrise/notch or equivalent views. OA here rarely occurs in isolation (<10%) and is usually part of medial or lateral knee OA.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint3.jpg
Patellofemoral pain is usually from overuse/training overload or malalignment.
Contributors to overuse involve total joint load which may have influence from training volume (total miles), intensity (competitive sports) in addition to BMI (>25) in addition to overall fitness level.
Malalignment aka abnormal patellar tracking involves both static (leg length discrepancy, hamstring tightness, etc.) and dynamic components (hip weakness, gluteus medius weakness, excessive foot pronation, etc.).
Patients with anterior knee pain should have activity modification, ice, NSAIDs (not steroids) and long-term engagement in physical therapy (>6 months) with a focus on flexibility and strengthening of lower extremity kinetic chain including the vastus medialis, gluteus medius, hip external rotators and core.
Also, consider looking for hyper supination or pronation. Foot orthotics can be of help with this.
{kind=link}
{kind=link}