This study was a retrospective review of restraint use at a level 1 trauma center in the Midwest.
It found the following were factors in a patient encounter associated with an increased risk of restraint usage:
This study found a decreased OR of restraint use with Black or Hispanic race, which was in contrast to other studies
This was a single center, retrospective study, so it was already limited in what it could tell us. In addition, they didn't see the reason for the restraints being ordered in the first place. Nonetheless, it does show that people in certain marginalized groups have a higher likelihood of ending up in restraints. Please think twice when ordering restraints in the ED, especially for behavioral reasons
Since 2014, Medicare has payed for inpatient services for Medicare patients who’s admitting physician noted that hospital stay required at least 48 hours (measured as 2 midnights) or required specialty care that could not be performed as an out patient. This rule now will apply to Medicare Advantage insurance patients as well. Physicians will need to document their reasoning why a patient’s stay will likely require two midnights.
As the calendar flips to a new year, consider not setting goals or resolutions. Studies show unmet goals or having too many half finished projects leads to increased stress, anxiety and depression. Instead, consider approaching the new year looking for growth, introspection, and striving to achieve excellence. Understanding the why and what motivates you will lead to the correct what and how. Here are some questions to get you thinking about the why. May your New Year be filled with growth and excellence!
A recently published study of ED APPs, residents, attendings, and nurses attempted to assess clinician's perspectives on how ED boarding impacts ED staff and patients. Authors performed a survey followed by focus group sessions to obtain qualitative insignts from participants.
All respondents associated boarding with feelings of burnout and self-reported poor satisfaction with communication and the process of boarding care.
Several key themes emerged which are outlined below:
This publication highlights the negative workforce and patient safety effects of ED boarding. It amplifies the voices of our colleagues who work towards change to improve both the health of our wrokforce as well as that of our patients and the communities that we serve.
Takeaway Points - A 10 percent reduction in ED volume reduces an ED patient's chance of dying by 24% at 30 days and by 17% at six months
The author of this study conducted a unique natural experiment. They identified cases in which a new emergency department opened near one or more existing departments. Then, they confirmed that the opening of the new department was the only substantial change that occurred (e.g. the staff in the existing EDs were unchanged, the types of complaints were unchanged etc.). The author then determined the impact of the new ED on the existing ED's patient volume and compared death records from the existing EDs before and after the new ED opened.
Simply offloading 10 percent of patients from the existing ED to the new ED, significantly reduced the 30 day and six month risk of death for the existing ED's patients.
The Bottom Line: Many studies have attempted to determine the impact of boarding and to tie boarding to morbitiy and mortality. This author's unique approach to the problem serves to reinforce the need for comprehensive solutions to the problem of patient boarding. Even a modest reduction in emergency department volume has a measureable impact on patient outcomes
Physician Workforce Diversity in EM
Health inequities along racial, ethnic, and socioeconomic lines are a brutal reality of the current state of health care in the US. One way to attempt to address these inequities is to make a concerted effort to diversify our physician workforce. As authors have noted, “Having physicians from diverse backgrounds as colleagues and role models can promote understanding and tolerance in nonminority physicians, ultimately improving medical care for patients who are part of these racial and ethnic groups. Increasing the population of underrepresented minority (URM) physicians in the workforce also directly improves health care for medically underserved populations from all racial and ethnic backgrounds, as studies have shown that physicians from URM backgrounds are more likely to work with these patients.”
Administrators are often tasked with the difficult job of creating a cohesive group of emergency physicians to meet the needs of the community they serve. Strategies to diversify that workforce would benefit from a multi-level approach, including the following:
Small steps can create big changes.
Since the switch from fee for service to value based care in the US, there has been a marked push to improve our documentation to expand our MDM and differential considerations. We are all here becoming adept at the medical documentation (thanks Dr. Adler!), but may not be adequately documenting our patients' social determinants of health using the social Z codes, a subset of ICD-10 coding language
This study wanted to look at the overall prevelance of social Z code utilization. They used the Nationwide Emergency Department Sample (NEDS), a nationwide database of ED visits, to look at this particular documentation. They examined 35 million (!) ED visits and found that only 1.2% had any social Z code included in the documentation. Given how many resources are linked to a verified (eg documented) need, this raises the idea that if Z codes are better documented, this may lead to increased funding for things like food, housing and transportation insecurities.
Limitations- the authors only examined the ED visits for ICD-10 codes, they didn't specifically look at the notes themselves which may have contained SDOH information. They also found that the social Z codes were more often documented in visits coded for mental health diagnoses, potentially indicating bias. There is also the concern that patients may not want the social z codes included, given the stigma around things like homelessness.
Overall, social Z code documentation could potentially unlock better resources for our patients by documenting a specific need in a population. More will come as documentation continues to evolve.
The WHO and the US Department of Health and Human Services, among other groups, recommend between 150-300 minutes of moderate intensity or 75 to 150 minutes of vigorous intensity physical activity per week.
This could add up to almost 45 minutes a day!
Who has the time for that?
This is an extremely challenging goal with work and other life responsibilities.
Some recent studies asked whether routinely cramming the recommended weeks’ worth of physical activity into a couple of days, weekend warriors (WW), leads to the same life-extending benefits as distributing the exercise load throughout the week.
In a retrospective analysis of almost 90,000 individuals (56% women), providing a week of accelerometer-based physical activity data: Three activity patterns were compared: active weekend warrior (active WW, ≥150 minutes with ≥50% of total achieved in 1-2 days), active regular (≥150 minutes and not meeting active WW status), and inactive (<150 minutes).
A weekend warrior (WW) pattern of physical activity was associated with similarly lower risks of cardiovascular outcomes (incident atrial fibrillation, myocardial infarction, heart failure, and stroke) compared with more evenly distributed physical activity.
Another large prospective cohort study of over 350,000 US adults (51% women) did not find any significant difference in mortality rates between weekend warriors and regularly active participants. Compared with physically inactive participants, active participants (both weekend warrior and regularly active) had lower all-cause and cause-specific mortality rates.
Take home: Any exercise is better than none. Adults who perform 150 minutes or more of moderate to vigorous physical activity (or 75 minutes of vigorous activity) per week may experience similar health benefits whether the sessions are spread throughout the week or concentrated in a weekend.
Note: Being a weekend warrior can increase the risk of MSK complications and injury..
Future studies should include the use of wearable devices and not rely on self-reporting exercise behavior.
In a recent study of emergency physicians (EPs) who left the workforce between 2013 and 2020, authors sought to investigate their age and number of years since residency graduation for males and females.
A total of 25,839 (70.2%) male and 10,954 (29.8%) female EPs were included.
Female gender (adjusted odds ratio 2.30) was significantly associated with attrition from the workforce.
Of those who left the workforce, the median number of years after residency that males left was 17.5, as compared with only 10.5 years for females.
Furthermore, among those who exhibited attrition, one in 13 males and one in 10 females exited clinical practice within 5 years of residency graduation.
As authors emphasize, these data identify widespread gender-based disparities regarding EM workforce attrition that are critical to address to ensure stability, longevity, and diversity in the EP workforce.
Substance use disorder is now known to be a function of brain disease and not a moral failure. Patients with substance use disorder are highly complex and often use the ED at a higher frequency than those without the disorder. However, these patients are also frequently the target of implicit bias and stigmatizing behavior from the healthcare team that can lead to worsened outcomes. Add on top of that a racial disparity, and we can see how this group of patients can have really bad health outcomes.
This study looked at the length of time to treatment of patients with SUD, to see if there was a difference within this group based on racial or ethnic differences. It did find that black patients with SUD did wait on average 35% longer in the ED before being seen or treated. This difference was statistically significant.
While this study wasn't designed to identify the causes of such a disparity, it does raise concern for implicit bias being in effect among not only the healthcare workers, but ingrained into the healthcare systems themselves.
Patient's with SUD are a vulnerable group of patients, and black patients with SUD are experiencing a disparity in time to treatment. This should remind us all to seek out ways to remove these biases and disparities from the systems where we work.
Author- Steve Schenkel, MD MPP Professor of Emergency Mediciner at UMEM:
A recent Annals of Emergency Medicine Publication (here https://www.annemergmed.com/article/S0196-0644(22)01276-8/fulltext) tested a predictive rule for Likelihood to Occupy an Inpatient Bed associated with a common Electronic Health Record.
At the individual patient level, the score performed ok. Depending on the chosen threshold, it traded off sensitivity and specificity and generally became more accurate the longer the patient was in the ED.
The authors and the associated editorial (here https://www.annemergmed.com/article/S0196-0644(22)01401-9/fulltext) suggest a different, potentially more beneficial use: to allow aggregate prediction of admissions across an entire department and therefore prompt earlier planning to prevent crowding on account of boarding.
The takeaway: Administrative prediction rules oriented toward individual patients may be more meaningfully used to predict resource needs, including in-patient beds, across the ED population.
How much screen time after concussion?
Adolescents spent more than 7 hours daily on screen time during the pandemic.
Historically, experts recommended screen time abstinence to various degrees after concussion.
Prior study: RCT of concussion patients (ages 12 to 25) found that those who abstain from screen time for the first 48 hours recovered 4.5 days sooner than those who were permitted screen time.
Population: 633 children and adolescents with acute concussion and 334 with orthopedic injuries aged 8 to 16, recruited from 5 Canadian pediatric emergency departments.
Post concussion symptoms were measured at 7 to 10 days, weekly for three months, and biweekly for three to six months post injury. Screen time was measured.
Results: Screen time was a significant predictor of post concussion symptom recovery with both parent reported somatic and self-reported cognitive symptoms.
There may be an effect of low to moderate screen time (Goldilocks effect) demonstrating that those in the 25th to 50th percentiles had less severe symptoms than those on the higher end of screen time use or those who minimally use of screens!
Low and high screen time were both associated with relatively more severe symptoms in the concussion group compared to the orthopedic injury group during the first 30 days post recovery but not after 30 days.
Conclusion: The association of early screen time with post concussion symptoms is not linear. Recommending moderation in screen time may be the best approach to clinical management.
Children need to strike a balance between avoiding boredom, deconditioning, isolation, and overexerting themselves physically or cognitively.
a 37 year old patient comes in with chest pain, you obtain the following ECG. Is this a STEMI or Pericarditis?
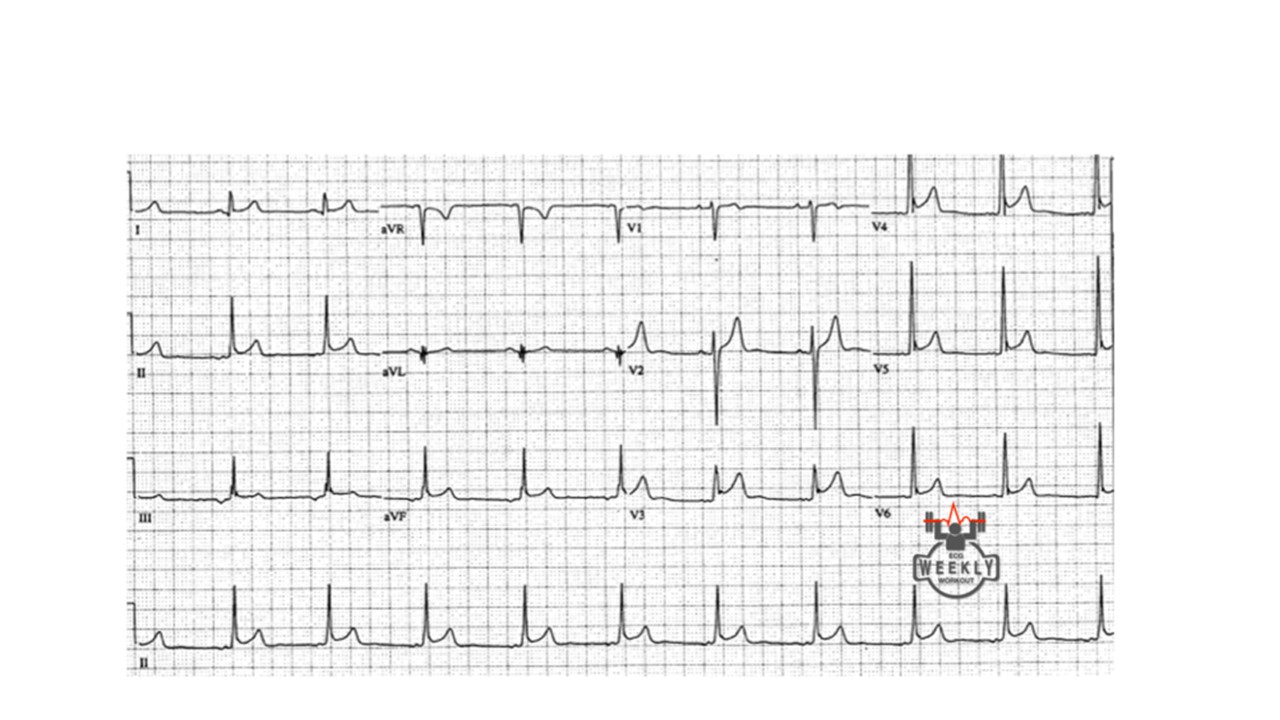
How can you tell? well, you follow the algorithm Dr. Mattu taught us....
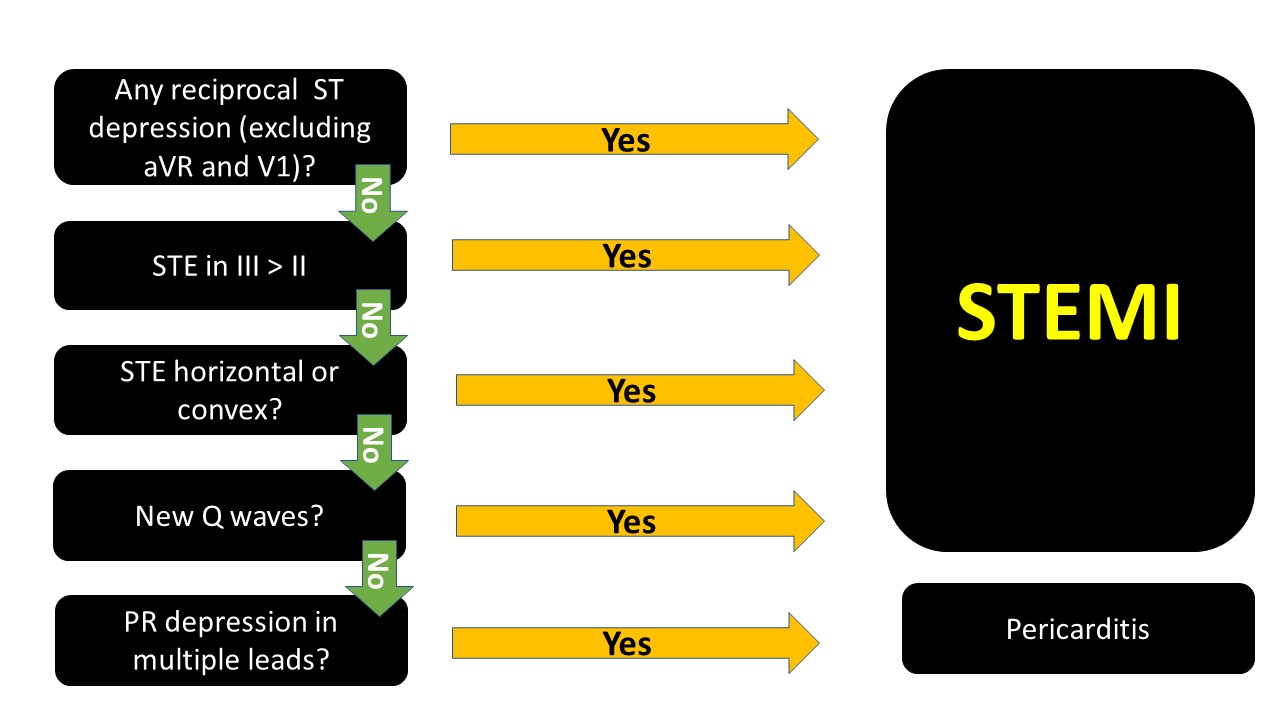
The ECG above, if you go through the algorithm you will see that it is most likely pericarditis.
note that PR depression can be transient and you might not see them.
When in doubt, it is not wrong to consult cardiology. Getting serial ECGs also is important, STEMIs will usually evolve.
We hope that you enjoy your Memorial Day!
Don't forget your Sandy Beach Sign vs Barcode Sign of Lung Ultrasound:
Normal lung will have good pleural sliding. When you image the lung with M-Mode it looks like a Sandy Beach.
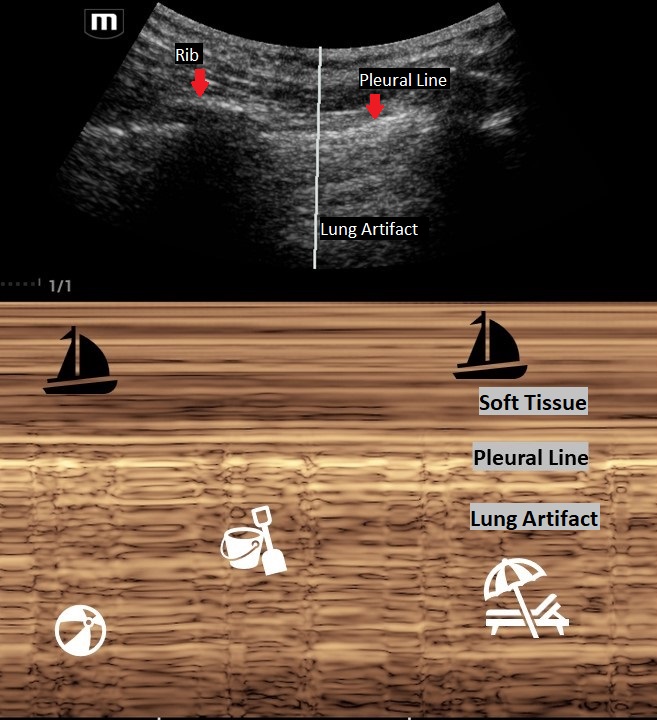
A lung with a pneumothorax will have poor lung sliding. When you image the lung with M-Mode it looks like a classic barcode or "stratosphere sign."
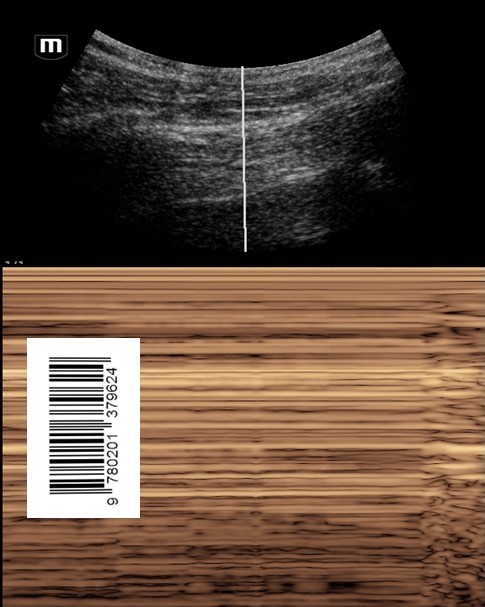
Make sure that you are on "Lung Mode" or decrease the gain to better image the movement of the pleural line. The negative predictive value for lung sliding on ultrasound is 99%. This means that if you see lung sliding you do not have a pneumothorax in that area. However, lung sliding is affected by certain conditions such as blebs, pulmonary fibrosis, pleural adhesions and right mainstem intubation. So, like any other radiology study, clinically correlate!
Thinking about placing a chest tube or have a patient with multiple rib fractures? Take a look at how to perform a Serratus Anteror Plane Block here: https://www.thepocusatlas.com/thoracoabdominal-blocks#Serratus
Clinician Well-Being and the Patient Experience
Did you know that most patient experience responses are overwhelmingly positive? Rather than focusing all our attention on the bad, let’s focus on the good to promote clinician well-being. See below for a few key points from a recent study on this:
Consider emphasizing positive patient experiences when providing feedback to emergency physicians. It will promote clinician well-being and help improve performance in your practice.
Did you know that you can use the linear probe with pulse wave (PW) doppler over the femoral artery to look for a pulse during CPR pauses?
Well, the researchers of this article took this skill one step further to evaluate if they could use the femoral artery PW doppler while CPR was in progress to look for signs of a pulse.
The authors found that:
- pulsations due to compressions were organized with uniform pulsations.
- when there was also native cardiac activity, the pulsations were nonuniform and may have an irregular cadence.
Although there were several limitations, Arterial doppler was 100% specific and 50% sensitive in detecting organized cardiac activity during active CPR.
Take Home Point: Take a look at your arterial doppler for signs of organized cardiac activity during a resuscitation.