Pes Anserine Bursitis is an inflammatory condition of the medial knee
Occurs at the bursa of the pes anserinus which overlies the attachment of the 1) Sartorius 2) gracilis and 3) semitendinosis tendons
Note the location is 2-3 inches below the knee joint on the medial side
http://kneespecialistsurgeon.com/images/uploaded/Pes%20anserinus%20bursitis%20image.jpg
http://eso-cdn.bestpractice.bmj.com/best-practice/images/bp/en-gb/575-27_default.jpg
Patients complain of pain (especially with stair climbing)
PE: Tenderness to palpation of the bursa with mild swelling
DDx: MCL tear, medial meniscus injury, medial (knee) compartment arthritis
Treatment: Cessation/modification of offending activities, Icing and ice massage, NSAIDs, hamstring stretching and physical therapy. Failure of the above should prompt referral for bursal steroid injection.
Kocher Criteria for Septic Arthritis in Children:
Septic arthritis should be suspected in children that have a painful joint especially if they do not want to weight bear. Orthopedics uses the Kocher Criteria to determine the probability of whether the joint is infected.
Four elements make up the criteria:
If only one sign is present there is a 3% chance the child has a septic joint.
Kienbock’s disease is a rare entity involving collapse of the lunate due to avascular necrosis and vascular insufficiency.
Occurs most commonly in young adults aged 15 to 40 years.
Cause is unknown but believed to be due to remote trauma or repetitive microtrauma in at risk individuals.
Patients complain of wrist pain, stiffness and swelling
On exam, limited range of motion, decreased grip strength and passive dorsiflexion of the 3rd digit produces pain.
Dx: plain film in the ED and with MRI as an outpatient.
Tx: Wrist immobilization with splint and refer to orthopedics. Ultimate treatment is individualized and there is no clear consensus.
Lunate sclerosis seen on plain film
http://orthoinfo.aaos.org/figures/A00017F02.jpg
AVN of the lunate seen on MRI
http://www.assh.org/Public/HandConditions/PublishingImages/KeinbocksMRI_figure3.JPG
Transient brachial plexopathies aka Burners and Stingers
Brachial plexus injuries are the most common peripheral nerve injuries seen in athletes.
49-65% of all college football players have experienced at least one burner with a 87% recurrence rate.
Injuries most commonly occur at C5-C6 but may involve any root level.
3 Mechanisms: Commonly due to
1) Traction caused by lateral flexion of the neck away from the involved side
2) Compression of the upper plexus between shoulder pads and scapula
3) Nerve compression caused by neck hyperextension and ipsilateral rotation.
CC: Burning or numbness in the neck, shoulder and/or arm
Symptoms are UNILATERAL and tend to usually last seconds to minutes
Symptoms are reproduced by the Spurling maneuver.
Function gradually returns from the proximal muscle groups to the distal muscle groups.
Because most burners are self-limited, the most important goal is to rule out an unstable cervical injury.
Iliopsoas tendonitis and Iliopsoas Syndrome
Meralgia Paresthetica - caused by entrapment of the lateral femoral cutaneous nerve (LFCN)
The LFCN is responsible for sensation of the anteriorlateral thigh.
http://www.chiropractic-help.com/images/Meralgia-Paresthetica.jpg
NOTE* It has no motor component!
Associated with pregnancy, wearing tight pants, belts, girdles, and in diabetic and obese patients.
Symptoms include numbness, paresthesias and pain (not weakness). Worse w walking, standing. Better w sitting.
Diagnosis is clinical but may be confirmed with nerve conduction studies
Treatment includes, NSAIDs, injection and surgery for refractory cases.
Tendon Lacerations:
A reasonable approach to all tendon lacerations is to close the wound and splint in the hand in the position of function until the patient can be seen by a hand surgeon in the next 1-3 days. These injuries do not require immediate surgical repair.
Tendon Lacerations:
Hand lacerations need to be carefully explored in order to determine whether there is an associated tendon laceration. These can be be difficult to find unless a systematic approach is followed:
Future pearls will cover techniques on how to repair tendon lacerations. Stay tuned.
Gout treatment considerations
Treatment is directed to relieve pain and inflammation
NSAIDs, steroids and narcotics are the mainstays of treatment. All 3 should be used in combination.
Aspirin should be avoided as it may increase uric acid levels
Note: not in prevention doses (81mg) in treatment doses (325-650mg q4h)
NSAIDs and steroids take time to be effective. Provide appropriate analgesia with oral narcotic medication for short term relief
Don't forget the benefit of splinting a "hot" joint (the ankle or wrist for example)
NSAIDs: Use may be limited in the elderly and in those on coumadin or with peptic ulcer disease. 5-7 days of treatment is usually sufficient. Indomethacin is most commonly used (50 mg TID, which may be tapered to 25 mg TID after 3 days)
Steroids: Likely more effective than NSAIDs. Oral prednisolone is more effective than naproxen (1). Use prednisone 30-50 mg for 3-5 days without tapering (as we use for asthma). May be useful to supplement with NSAIDs on the tail end to prevent a rebound flare. If tapping the joint consider intraarticular steroids. If there is concern for medical noncompliance with oral steroids consider IM steroids (triamcinolone 60mg or methylprednisolone).
Gout Part 2
Knee dislocations are uncommon, and prosthetic knee dislocations even rarer. Some general facts about prosthetic knee dislocations are:
GOUT part 1
Gout is an inflammatory arthritis that classically affects the first metatarsal phalangeal joint
Gout prefers cool ambient temperature hence gouty tophi prefer the great toe (one of the coldest parts of the body) and avoids "warmer" joints such as the hip and shoulder.
Remember that gout can affect other joints as well (elbow, wrist, knee and ankle) and can cause painful bursitis and tendonitis
Multiple joints can be involved simultaneously (leading to confusing with RA and OA)
The involved joint will often be red, hot, swollen and very painful leading to easy confusion with cellulitis and or a septic arthritis
Diagnose gout by demonstrating monosodium urate crystals in the synovial fluid.
**Remember previous pearl by Dr. Bond regarding the coexistence of gout with septic joint**
Serum uric acid levels are commonly elevated but can be normal or even low
Use caution with this test because asymptomatic hyperuricemia is much more common than gout
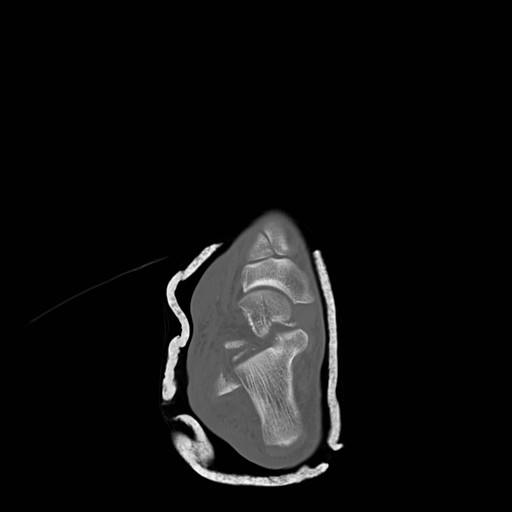
Talar Neck Fractures
Have a high rate of avascular necrosis (AVN), nonunion, and arthritis. Almost all require ORIF


Cubital Tunnel Syndrome aka Radial Tunnel Syndrome
Sever's disease ,aka calcaneal apophysitis, is a common overuse injury in the pediatric and adolescent population.
Occurs secondary to traction of the calcaneus that most often occurs in young athletes (8-12 yo)
-Avg. age of presentation is 11 years 10 months in boys & 8 years 8 months in girls
-Repetitive traction to the weaker apophysis, induced by the pull of the Achilles on its insertion
Hx: Heel pain that increases with activity (running, jumping).
-May involve one (40%) or both (60%) feet
PE: Tenderness of the posterior heel at the Achilles tendon insertion and ankle dorsiflexor weakness
Imaging: Radiography is often normal. When positive, show fragmentation and sclerosis of the calcaneal apophsis. NOTE: These findings are nonspecific and also are observed in asymptomatic feet.
http://t0.gstatic.com/images?q=tbn:ANd9GcQ9R-fx1iyhbhNJpNL2W72bWdK72_mRBLNX5DUDtcMfnDli-x7Ong
DDx: Includes osteomyelitis and tarsal coalition.
Tx: Rest from aggravating activities, NSAIDs, ice (both pre and post sport). When pain free a program of stretching (gastrocnemius-soleus), strengthening (dorsiflexors) and shoe inserts (heel cups, lifts, pads, or orthotics) can provide significant pain relief.
Distal Radius Fractures
Typically distal radius fractures are treated with closed reduction and splinting in the ED, followed by operative repair. This is done because it is felt that patients will have the best functional outcomes if the bones are restored to their normal anatomic alignment. However, two studies published in 2010 suggest differently.
The study by Neidenbach showed that after one year there was no difference in functional outcomes between patients that were just splinted in the ED in the position the fracture was found versus those that had closed reduction with splinting.
The second study by Ego showed that there was no difference in outcomes between those that underwent conservative treatment with closed reduction and splinting versus those that underwent operative repair.
The take home point from these studies for the EM physician is that most distal radius fractures can be splinted in the position found with them following up with an orthopaedist. There is probably little advantage to performing a closed reduction in the ED knowing that this procedure can use a lot of valuable time and resources.
Iliotibial band syndrome (ITBS)
http://footcarexpress.com/foot-orthotics/wp-content/uploads/2009/01/iliotibial-band-syndrome.jpg
Hx -
PE-
Tx
FARES Method for Reduction of Anterior Shoulder Dislocations.
This method that was recently highlighted in a publication had a ~78% success rate with the authors able to reduce the shoulder in an average of 2.36 ±1.24 minutes without having to give the patients any analgesics or sedatives. The technique is done by:
Consider trying this with your next shoulder dislocation. No single method of reduciton is 100% successful, but methods like this that only require a single provider and do not require analgesics are extremely helpful in improving patient flow as they do not utilize a lot of ED resources..
Involves an avulsion of the flexor digitorum profundus (FDP) tendon from its insertion on the distal phalanx.
Ring finger is most commonly involved.
Usually occurs from a grabbing attempt (resulting in forced DIP extension during maximal FDP contraction) as would occur while attempting to grab someone’s jersey such as in football or rugby.
Clinically, there is normal passive DIP ROM with loss of active flexion. Examine this by asking the patient to flex the fingertip at the DIP while the PIP joint is held in extension.
*Remember that patients with a 90% full-thickness tendon laceration may still have normal (albeit painful) range of motion. The examiner must evaluation the strength of the tendon against resistance. This injury is commonly missed as it is diagnosed as a “jammed” finger.
Plain films may show a bony avulsion, but are often negative.
Treatment is primary repair especially with large bony fragments. Partial ruptures can be treated nonoperatively at the discretion of the hand surgeon.
Peroneal Tendon Subluxation: The Other Ankle Sprain
{kind=link}
{kind=link}