Hypernatremia in Pediatric patients is less common than other electrolyte abnormalities occurring in <1% of hospitalized patients. The most common cause is water loss, either from poor absorption in the cases of vomiting, diarrhea, malabsorption or insensible losses, or via diabetes insipidus. Congenital disorders may cause decreased thirst receptors resulting in inadequate intake. Finally, excess sodium intake can occur via hypertonic fluids, ingestions or hyperaldosteronism or hypercortisolism.
Symptoms are often nonspecific- including fatigue, vomiting, hypertonia or hyperreflexia in lower states, but may result in lethargy, mental status changes or seizures as levels approach and exceed 160mmol/L
Treatment is similar to adults - free water deficit should be calculated:
Total body water (%) x weight (kg) x [(serum Na)/140 - 1]
Total Body Water (TBW) varies by age:
24-31 weeks- 90%
32-35 weeks - 80%
Term - 12 months - 70%
12 months and up - 60%
IV fluids should be started with a goal of decreasing the sodium level by 0.5 mmol/L/h with close monitoring of sodium levels.
This study looked at the success rates of femoral vs proximal tibial IOs in the prehospital setting. Over a 9 year period, there were 163 pediatric patients who received either a tibial or femoral IO. Femoral IOs were introduced into the EMS protocol in this study area in 2015 as a location option and were the recommended site starting in 2019. The success rate of femoral IO placement was 89% and for proximal tibial sites was 84.7%. After further data analysis the study found an adjusted odds ratio of 2 for successful IO placement in the distal femur compared to the proximal tibia. The complication rates for both sites were similar.
Bottom line: This study suggests that the distal femur is a reasonable site for IO access in the pediatric population.
Continuing with the electrolyte derangements in children: Hyponatremia
Hyponatremia is defined as a Sodium of less than 135 mmol/L and does not depend on patient age.
This is the most common electrolyte abnormality in pediatric patients. Excessive free water is often the culprit and is usually thought of in the neonate or infant whose guardians are mixing formula incorrectly. * Additional causes include inappropriate ADH (Antidiuretic hormone) secretion, or in the case of dehydrated patients appropriate ADH secretion. Sodium wasting is rare.
Total body water (TBW) is important to consider, and preterm neonates have higher TBW (80%) than full term (70%) and 1 year old infants (~60%) putting them at higher risk of hyponatremia.
Recognizing the volume status of the patient aids in determining the etiology of the hyponatremia and allows for appropriate treatment. This may require obtaining urine sodium.
Treatment:
Hypertonic saline should be used only for patients with severe neurologic complications including seizures or altered mentation. In these patients, a hypertonic saline bolus should be given at 3-5 ml/kg of 3% NaCl over 10-15 minutes.
In hypovolemic patients without neurologic symptoms, fluid resuscitation is the mainstay with caution to increase sodium levels by no more than 6-8mmol/L/day. For euvolemic or hypervolemic patients, fluid restriction is advised.
Prevention:
Importantly, when children receive IV fluids, the choice should be made to select isotonic fluids (0.9% NaCl) rather than hypotonic fluids (0.45% NaCl) to avoid iatrogenic development of hyponatremia.
*Reminder: 2 ounces (about 60 ml) of water should be placed in the bottle, and then 1 full scoop of formula, unless directed to have higher caloric content by their doctor- in which case the amount of formula in the mixture should be higher
Autism Spectrum Disorder (ASD) can often be a diagnosis that complicates usual ED evaluation and management. One of the frequently asked questions is “what medications work well for patients with autism?” It is often said, although with quite variable evidence in the literature, that benzodiazepines should be avoided in patients with ASD due to the risk of paradoxical reaction.
This study was a meta-analysis that included 20 different studies that looked at efficacy and adverse effect of various medications and medication combinations for procedural sedation for a variety of painful and nonpainful procedures. Although the heterogeneity of the indications, medications, and other details of study design of the studies included precludes a definitive recommendation as to the best medication or regimen, it does suggest overall reasonable efficacy of midazolam both as a single agent as well as in combination with dexmedetomidine, especially when balanced against adverse effects noted with some of the more efficacious regimens.
Take Home Point: Medication choice for patients with ASD should be individualized to the patient based on prior experiences, parental or patient input, and prescriber experience given proven efficacy of multiple regimens. Benzodiazepines should be considered within the toolkit.
This was an observational study where ultrasound was used to evaluate if the diaphragm came into view at the 5th intercoastal space (ICS) at the midaxillary line in pediatric patients during maximal respiration. A convenience sample of pediatric patients who presented to the an academic pediatric emergency department was used.
In 10.3% of patients, the diaphragm crossed the 5th ICS during normal respirations and 27.2% crossed during maximal respirations. This was a more common occurrence on the right compared to the left. An increase in body mass index was also associated with an increased risk of the diaphragm crossing the during both tidal respiration and maximal respirations.
Bottom line: Using a blind insertion of a chest tube at the 5th ICS, midaxillary line in the pediatric patient poses a not insignificant risk of piercing the diaphragm. this study recommends using ultrasound prior to chest tube placement.
Hyperkalemia is less common than hypokalemia in pediatric patients, though it is not uncommon to have hemolysis in patients who receive heel stick lab work.
The age of the patient is critical to determining the cutoff for hyperkalemia:
Typically, levels up 6.0mmol/L are well tolerated in children, unless the shift is rapid. For any child meeting age related hyperkalemia or who have a known lower prior potassium level should receive an ECG.
Treatment for hyperkalemia is similar to adults
Calcium Chloride (20mmg/kg - Max 1g) or Calcium Gluconate (0.5ml/kg - Max 20ml) is given for cardiac stability.
Albuterol can be given based on weight
Insulin and dextrose can be used with extreme caution and close monitoring for hypoglycemia. (Dextrose should be given as D10% in children under 5 years of age, D25% can be used if > 5 years old)
Emergency department visits for pediatric mental health and behavioural concerns have been increasing. This study attempted to further characterize medications, both home and for sedation, that were given to these patients.
This study included 670,911 youth with a mental or behavioral health diagnosis over a 9 year inclusion period. The most common diagnses were depressive disorder, suicide or self injury and disruptive, impulse control and conduct disorder. During this time, a total of 12.3% of patients had a psychotropic medication given while in the ED. The percentage and odds of administering these medications increased from 7.9% in 2013 to 16.3% in 2022. Those with intellectual disability and autism spectrum disorder had the highest frequency of medication administration.
Bottom line: As mental health visits in pediatrics continue to increase along with boarding times, clinicians should become more familiar with psychotropic medications used in this population and become comfortable in making sure that these patients have their home medications and have a plan for chemical sedation if other areas of de escalation fail.
Hypokalemia is a common electrolyte abnormality found in pediatric patients. The cut off for low potassium is based on age, with young infants having higher baseline levels of potassium when compared to older children and adults. The most common cause of hypokalemia in children is GI losses (diarrhea), though other considerations include malnutrition, congenital adrenal hyperplasia, renal abnormalities and medication effects.
Typically, hypokalemia is well tolerated, and the focus of management is based on treating the underlying cause, rather than repleting the potassium.
Medications should ONLY be initiated in patients who have potassium levels < 3.0 mmol/L OR with those with levels < 3.5 mmol/L with ECG changes.
In patients receiving treatment, oral potassium administration is typically recommended unless any of the following criteria are met:
In these patients IV potassium should be given (typically KCl at 0.5-1mEq/kg/DOSE - Max of 40 mEq/dose).
Just like in adults, ALL patients require continuous cardiac monitoring when receiving potassium infusions.
Teaching has circulated that a temperature of 40 degrees Celsius or above (hyperpyrexia), was associated with a greater incidence of serious bacterial infection. However, this teaching originated in a time prior to the availability of childhood vaccinations. In fact, the largest retrospective study to support this used data from 1966-1974.
2565 WELL APPEARING patients between the ages of 61 days and their 18th birthday who presented to a single tertiary care pediatric emergency department with the chief complaint of fever were included. The prevalence of serious bacterial infection was compared to the presence of hyperpyrexia, age, chronic conditions, gender and vaccination status.
Serious bacterial infections (SBIs) included: deep space infections, appendicitis, pneumonia, mastoiditis, lymphadenitis, acute bacterial rhinosinusitis, urinary tract infection, pyelonephritis, cholecystitis, tubo-ovarian abscess, septic arthritis, osteomyelitis, bacteremia or bacterial meningitis.
There was NO statistically significant association between hyperpyrexia and SBIs. Older age and make sex were associated with a higher risk of SBIs.
Bottom line: In well appearing children 61 days and older, having a temperature >/= to 40 degrees was not associated with serious bacterial infections.
The supracondylar fracture is one of the most common pediatric fractures. It typically occurs due to a FOOSH injury and is a result of fracture through an area of high growth (and therefore weaker bone structure) in the pediatric distal humerus. Appearance on x-ray depends on the degree of displacement, however in cases without obvious displacement, providers must look for more subtle signs on x-ray. For example, a “sail sign” of the anterior fat pad and appearance of a posterior fat pad indicate a joint effusion and are suggestive of a fracture. However, there are often still equivocal x-rays in children with notable tenderness on exam, and failure to appropriately immobilize these fractures can result in pain and higher risk of injury resulting in displacement.
In 2021, Varga et al, looked into the ability to assess for supracondylar fractures with ultrasound. This prospective study evaluated 5 locations in the pediatric elbow for signs of fracture. Ultimately, this was able to identify more fractures than x-ray alone, and was a useful tool for equivocal cases. This is not an isolated study, but one of the most comprehensive, looking into ultrasound as a tool for supracondylar fracture identification.
It may be time to grab that ultrasound probe to look for fractures in pediatric patients with pain but an unclear elbow x-ray.
Histamine is present in mosquito saliva contributing to itch with bites, however, certain populations – including children – can experience an exaggerated reaction. Skeeter syndrome is a large, localized inflammatory reaction secondary to a mosquito bite that presents with warmth, swelling, and itching. There can occasionally be associated lymphadenopathy and fever as well. The rapid onset is what best differentiates it from cellulitis. Treatment is primarily symptomatic in nature, focused on relieving itch, with antihistamines and topical therapy. There may also be a role for prophylactic antihistamine usage at times when mosquito bites will be unavoidable in a patient known to have developed Skeeter syndrome previously. Other patients who may be affected include those with immunologic and autoimmune phenomena, those with underlying atopy, outdoor workers with frequent exposure, and those with new exposure to indigenous mosquitos.
Take Home: Consider insect (mosquito bite) when evaluating for cellulitis/infection in pediatric patients, with impressive skin findings but otherwise unremarkable exams. They present with rapid onset and itching instead of pain. This can be especially prominent in periorbital and auricular presentations.
This was a cross sectional study examining insurance data to determine if there is seasonality related to ED visits and psychiatric hospitalizations related to suicidality.
Suicidality includes both suicidal ideation and suicide attempts (but not suicide). One survey showed that up to 12% of US adolescents reported serious thoughts of suicide. This study included 73,123 patients where 19.4% were direct inpatient admissions and 80.6% were ED visits, 44% of whom were subsequently admitted.
Metrics for suicidality in 10-18 year olds peaked in April and October with a nadir in June. Incidentally, in the Spring of 2020 when US schools closed due to COVID, there was a decrease in both ED visits and hospitalizations with April and May having the lowest rates across the study period.
School is believed to increase stress with risk factors such as bullying and peer pressure, academic and extracurricular stressors and poor sleep hygiene.
Bottom line: There has been an increase in adolescent suicidality over the recent years, many of whom present to the ED for evaluation. More mental health resources are needed, especially during the school year.
Intranasal medications are an increasingly popular option for pediatric patients, particularly for analgesia and anxiolysis, with an increasing number of medications being used via the intranasal route of administration.
Fentanyl has been shown in prior studies to be a safe and effective pain management strategy for children, but is likely under utilized. In sickle cell patients, studies have shown that time to analgesia may improve outcomes including hospitalization.
In 2023, Rees et al. showed that in the sickle cell patient population IN fentanyl can be a very effective tool for patient's experiencing a Vaso-occlusive episode (VOE). This study looked at 400 children with a mean age of 14.6 years. Of these 19% received IN fentanyl.
Ultimately, the IN fentanyl patient population had a shorter time to initial administration of analgesia and a lower chance of admission to the hospital.
Notably, this was not a randomized study, so there is limitations in assessment of the causality of the lower discharge rates. However this is a tool that could likely be used more regularly in the pediatric sickle cell patient population to allow for more rapid pain management in the emergency department.
This was a multicenter, randomized double blind, placebo controlled, non inferiority trial looking at children aged 2 months to 10 years with a diagnosis of urinary tract infection to see if the antibiotic course could be shortened from 10 days to 5 days in those patients who have clinically improved by day 5.
Children were prescribed amoxicillin/clavulanic acid, cefixime, cefdinir, cephalexin or trimethoprim-sulfamethoxazole and on day 6, after an in person visit were switched to placebo or continued the same antibiotic course.
A urine sample was collected on days 11-14 and treatment failure was defined as symptomatic urinary tract infection at or before this visit, asymptomatic bacteriuria, positive urine culture or gastrointestinal colonization with resistant organisms.
693 children were randomized in this trial. Children who received 5 days of antibiotics were more likely to have asymptomatic bacteriuria or a positive urine culture on days 11-14 (0.6 vs 4.2%). 28 children would need to be treated with a 10 day course to prevent one treatment failure with the 5 day course.
Bottom line: 10 days is still the ideal duration of treatment for a urinary tract infection, but the rate of failure of a 5 day course was low and the clinical significance of asymptomatic bacteriuria or a positive urine culture in an otherwise asymptomatic child is unknown.
In early 2023 Newgard et al published an article in JAMA which looked at pediatric readiness in ED's across the county. This study showed that there was a significant increase in pediatric mortality in patients who presented to EDs with lower readiness scores (<87 out of 100) when compared to those with higher readiness scores. And this translated to not just the time in the ED, but up to a year after they are seen in an ill-prepared ED. This number equated to an estimated total of 1,500 preventable deaths in children in the US each year.
Notably this does NOT look at what designation your hospital has for pediatrics (so being a level 1 pediatric trauma center does not automatically give you any points). This is based on having the physical materials needed for each age group, plans in place for specific patient age groups and evaluations (lower radiation doses for children in CT, using an US before CT for appendicitis evaluation, etc), and a person/people in place to review cases and ensure everyone is up to date on pediatric related training.
Want to check YOUR score? Go to https://www.pedsready.org/
Sepsis remains a leading cause of mortality in the pediatric population, and we have long been overdue for an update in recognizing and risk stratifying our pediatric patients.
Until now, pediatric sepsis screening guidelines have followed a framework modeled after the adult screening criteria from 2001 (Sepsis-2): Systemic Inflammatory Response Syndrome (SIRS). While attempts were made in 2005 to adjust these criteria to the pediatric population, data has shown poor specificity correlating to PICU admissions, need for critical interventions, end organ damage, and mortality.
As a reminder: Pediatric SIRS criteria: Temp >38.5 C or <36 C, tachycardia (or bradycardia if <1yr old), Tachypnea, leukocytosis/ leukopenia or >10% bandemia
In 2016, Sepsis-3 revised the criteria for sepsis and septic shock for the adult cohort by placing the focus on the presence of life-threatening organ dysfunction, which led to adopting criteria such as the SOFA and qSOFA scores to predict mortality risk.
Enter: The Phoenix Sepsis Score
An international, multidisciplinary task force convened by the Society of Critical Care Medicine in 2019 used evidence from an international survey, systematic review and meta-analysis to develop and validate a scoring tool intended to identify life-threatening organ dysfunction in children. Scoring tool was derived and validated retrospectively using an international, multi-center electronic medical record review of 3 million pediatric hospital encounters (excluding pre-term infants born <37 weeks and birth hospitalizations).
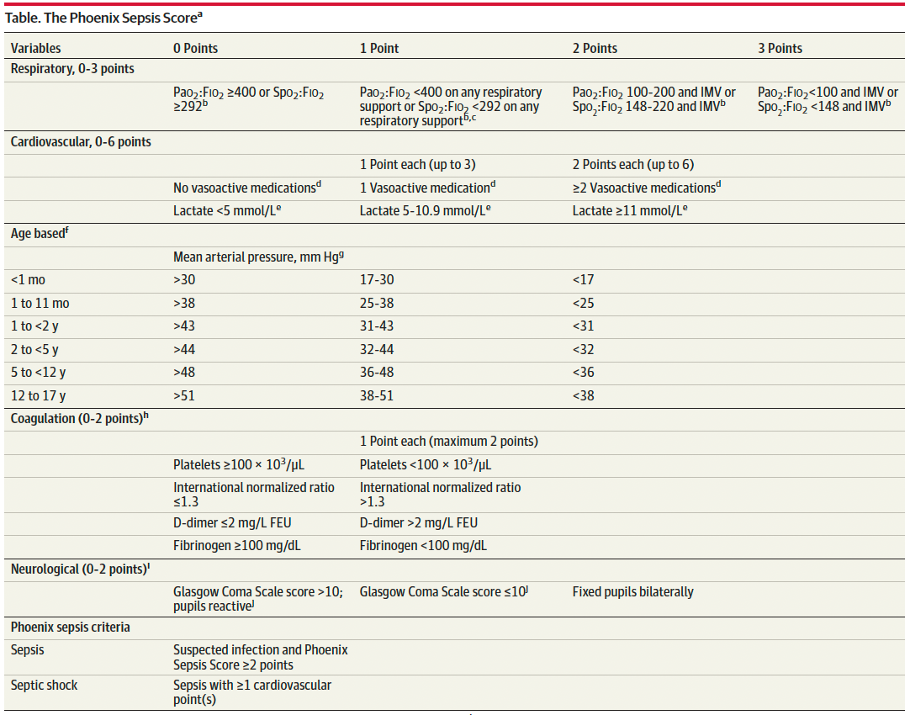
A Phoenix score of at least 2 carried a 7.1% risk of in-hospital mortality (in higher resource settings such as the USA).
Children with sepsis and organ dysfunction remote from the primary site of infection (eg respiratory failure in a child with meningitis) carried the highest mortality burden (8%) in this study.
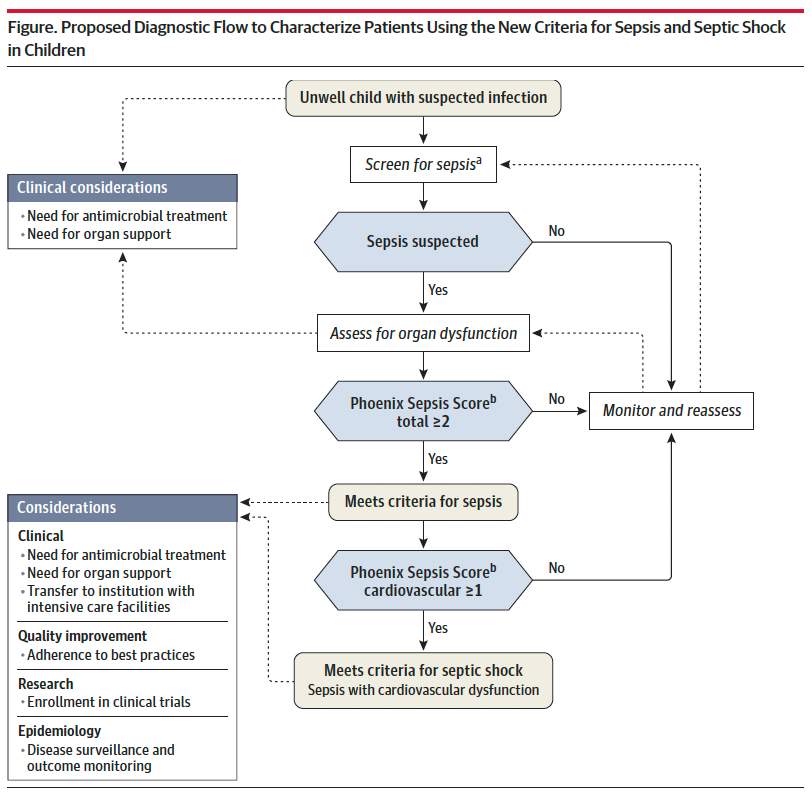
Sepsis is identified in children with suspected infection and an overall Phoenix score of 2 or more points, as this indicates potentially life-threatening organ dysfunction and thus carries higher mortality risk. Septic shock is identified by a score of 1 or more point(s) in cardiovascular dysfunction.
Lastly, it is important to recognize that this scoring criteria is NOT a sepsis screening tool, but rather should be applied when there is clinical suspicion for significant infection in the unwell child, or meeting sepsis screening criteria per your institutional criteria. Screening pediatric patients remains a clinical challenge, and there is not yet a reliable tool to apply to this population.
Bottom Line: Sepsis remains a significant cause of pediatric morbidity and mortality. The Phoenix Sepsis Score should be applied to the unwell child with suspected infection to identify sepsis and septic shock, thereby providing risk stratification and improving clinical care. Sepsis is defined by a Phoenix score of 2 or more and septic shock by a score of 1 or more in the cardiovascular category.
Standard practice regarding various pediatric fractures has started to shift over the last several years, often to less restrictive means of treatment. Torus (buckle) fractures of the distal radius are one of the most common pediatric fractures and tend to heal very well with minimal intervention.
The FORCE study (FOrearm fracture Recovery in Children Evaluation), a multicenter study out of the UK, was conducted to compare rigid immobilization (splinting) to a soft bandage used as needed per family discretion for treatment of these fractures. There was no different in outcomes of self-reported pain, function, quality of life, complications, or school absences. UK orthopedic guidelines have been updated to reflect a recommendation against rigid immobilization as well as against any need for specialist follow-up. American guidelines are slower to follow suit, but in recent years have transitioned to an approach of a removable brace.
Take Home: Pediatric torus fractures of the distal radius likely do not require immobilization and can be managed with self-limited activity instead. Practice in the US is in flux, but it is reasonable to manage with a removable brace or soft dressing as well as pediatrician follow up.
The gold standard for confirming ETT position is a chest xray, but this can often be delayed while the patient is stabilized. Many physicians will estimate ETT insertion depth to be 3x the ETT size, but this is based on selection of the correct tube. There are several other published formulas, including the PALS guidelines [age in years/2 + 12] which applies to children older than one year. In 1982, there was an article published that cited the formulas of [Height (cm) x 0.1 +5] or [Weight(kg)/5 + 12].
This was a retrospective study where the ideal position of cuffed ETT (from the front teeth) was determined by looking at post intubation xrays of 167 patients between 28 days and 18 years. The individual optimal ETT insertion depth was plotted against age, weight and height for all children. This study showed that there is not a fully linear relationship between age, height or weight which is a flaw of all of these formulas. Calculations using the patients’ weight performed the worst. Age based and height formulas performed the best.
You've heard of one kill pills such as calcium channel blockers, beta blockers, sulfonylureas, anti-malarials, but less commonly known is benzonatate, or tessalon perles.
Tessalon perles are not recommended for children under the age of 10. 1-2 capsules of benzonatate in children <2 years old have been reported to cause serious side effects including restlessness, tremors, convulsions, coma and even cardiac arrest rapidly after ingestion (within 15-20 minutes and death within a couple of hours). It is attractive to young children as it somewhat resembles a jelly bean.
Pearls on Tessalon Perles:
BACM stands for benign acute childhood myositis which is typically a benign, viral induced self limiting illness. This was a retrospective study looking at 65 patients in Italy to further characterize the characteristics of the disease.
In this study, the median patient age was 6 years with a male predominance. The incidence of BACM peaked in winter with a second peak in the fall. Patients presented with prodromal symptoms including fever, cough, coryza, sore throat and vomiting. The exam showed difficulty walking and myalgias with reproducible calf tenderness and preserved reflexes. Influenza B and A, COVID and other viral pathogens have been detected in these patients.
Lab work may show an elevated creatinine kinase, AST and potassium. WBC and CRP may also be elevated. The median CK value was 943 U/L and on average normalized within one week. Other studies have shown median CK values in the 3300s. Treatment includes hydration to promote CK clearance and prevent complications including acute kidney injury related to rhabdomyolysis. Recurrent myositis or CK values > 5000 U/L should have screening tests for muscular dystrophy and metabolic disorders.