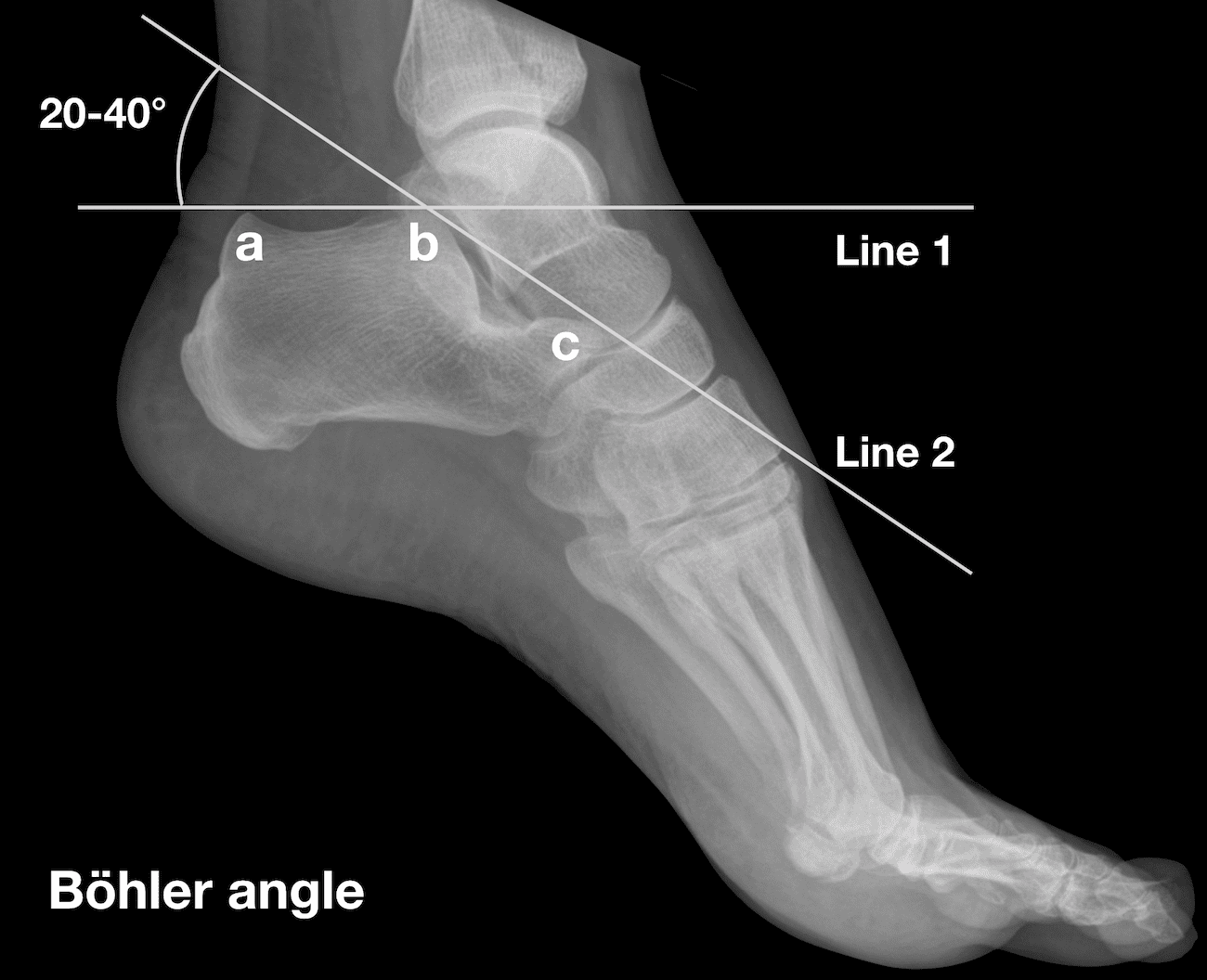
"The normal value for the Böhler angle is between 25° and 40° 1. Although there is wide variation between individuals, there is relatively little variation between the left and right feet of a single individual 2. A reduced Böhler angle can be seen in displaced intra-articular calcaneal fractures. The degree of reduction in the Böhler angle is an indicator of the severity of calcaneal injury, and the degree to which the Böhler angle is restored at surgery is correlated with functional outcome 3."
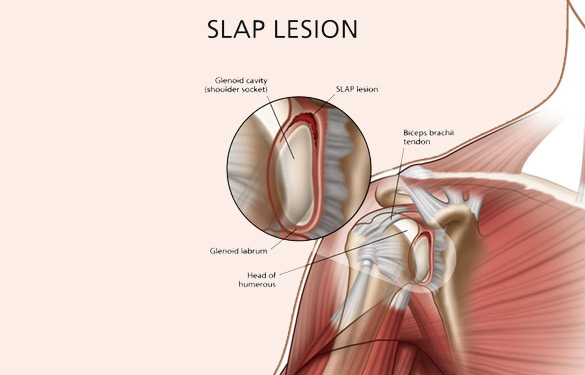
SLAP tear/lesion – Superior labral tear oriented anterior to posterior
Glenoid labrum – A rim of fibrocartilaginous tissue surrounding the glenoid rim, deepening the “socket” joint.
Integral to shoulder stability.
https://aosm.in/storage/2019/05/ch-shoulder-slap.jpg
O’Brien’s test aka active compression test for superior labral pathology.
2 parts – generally performed with the patient standing.
The patient’s shoulder is raised to 90 degrees with full elbow extension and approximately 30 degrees of adduction across the midline.
Resistance is applied, using an isometric hold.
Test in both full internal and external rotation
-This alters the position and rotation of the humerus against the glenoid
A positive test is when pain is elicited when the shoulder is in internal rotation with forearm pronation (thumb to floor) and much less or no pain when in external rotation (supination).
Note: AC joint pain may test similarly but will localize to different area of shoulder
The presence of similar, reproducible deep and diffuse glenohumeral joint pain is most indicative of a true positive test.
https://i0.wp.com/musculoskeletalkey.com/wp-content/uploads/2020/03/f50-02-9780323287845.jpg?w=960
Multiple vision disorders may occur after concussion including injury to the systems that control binocular vision including: Convergence insufficiency and Accommodation insufficiency
In order to obtain a single binocular vision, simultaneous movement of both eyes in opposite directions is required.
To look at an object close by such as when reading, the eyes must rotate towards each other (convergence).
Convergence insufficiency is the reduced ability to converge enough for near vision and is a common visual dysfunction seen after concussion.
One of both eyes may also turn outward.
May lead to complaints with reading such as diplopia, blurry vision, eyestrain, and skipping words or losing one's place.
Patient or parent may also report other difficulties such as becoming more easily fatigued when reading, needing to squint and/or having disinterest in reading.
Take home: consider testing convergence in patients with some of these complaints in setting of acute or subacute head trauma.
The use of a fascia iliaca compartment block has been shown to reduce pain, decrease length of stay and decrease the opiate requirements for patients with hip fractures.
Check out this page on how to perform this procedure.
Fascia iliac blocks can be challenging to implement routinely in the emergency department. Studies show that 2.5% of eligible patients, despite departmental implementation, receive a block.
One recently published article showed that large scale multi-disciplinary implementation can increase the use of fascia iliac blocks. After implementation, the study team found that 54% of eligible patients received a fascia iliac block.
This article is interesting as it provides helpful resources including physician and nursing protocols for performing this block.
Adhesive capsulitis aka frozen shoulder
Definition: Gradual development of global limitation of both active and passive shoulder motion, characterized by severe pain and lack of radiographic findings
Idiopathic loss of BOTH active and passive motion (significant reduction of at least 50%)
Motion is stiff and painful especially at the extremes.
Occurs due to thickening and contracture of the shoulder capsule.
Affects up to 8-10% of people of working age.
Affects patients between the ages of 40 and 60.
Peak age mid 50s
Onset before 40 is rare (consider other diagnosis).
Affects women more than men.
Diabetes is the most common risk factor.
Patients with DM, suffer a more prolonged course and are more resistant to therapy
Also associated with thyroid disease and prolonged immobilization
Increased risk following trauma to shoulder region (rotator cuff tear, following shoulder surgery, fracture of proximal humerus)
Presents unilaterally (other shoulder may become involved in next 5 years)
Slight increased risk of non-dominant shoulder
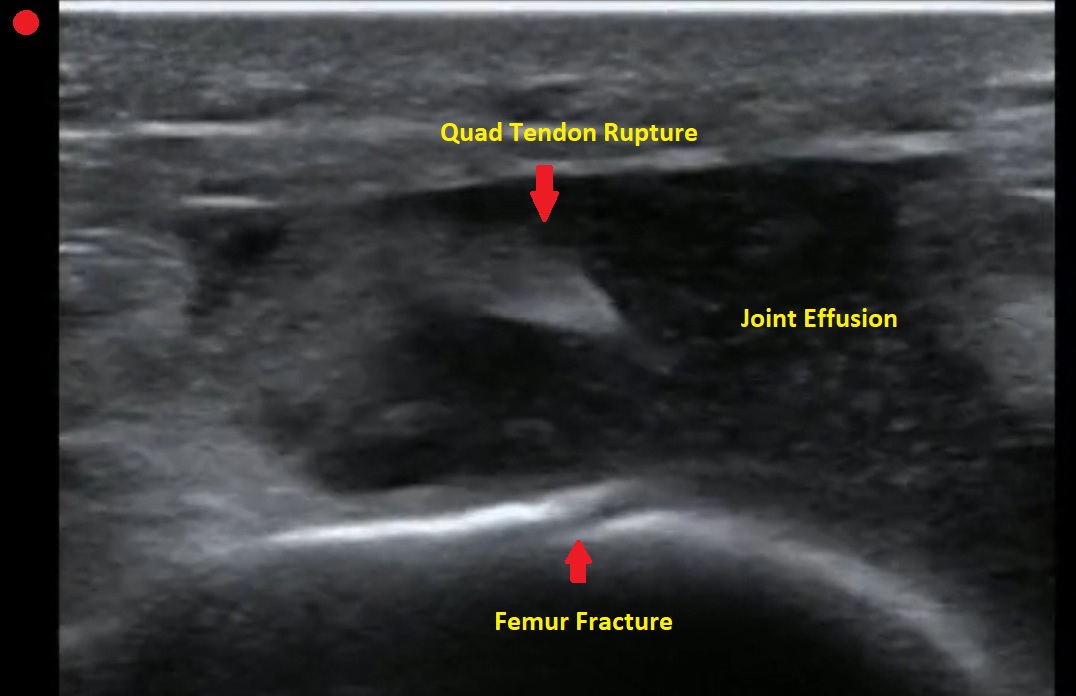
Pt presents to the emergency department with knee pain.
You decide to ultrasound the proximal knee. You place your ultrasound probe in the midline of the knee with your probe marker towards the patient's head.
What is the diagnosis?
-
--
---
--
-
The answer is a quadriceps tendon rupture with femur fracture.
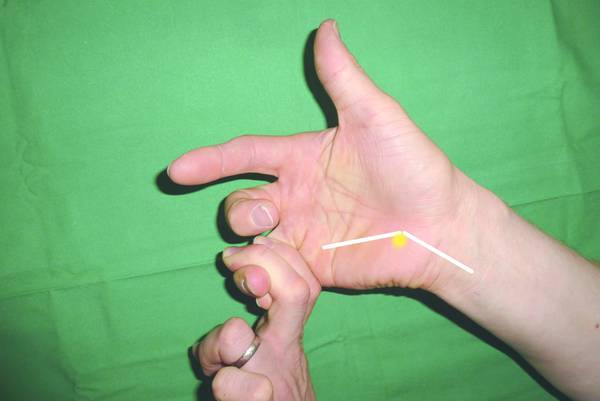
Intersection syndrome
Intersection syndrome is an overuse injury of the forearm.
Pain is located approximately 2 finger breaths (4cm) proximal to the wrist joint.
https://www.sportsmedreview.com/wp-content/uploads/2020/11/intersectionsyndrome.png
Mechanism: friction is caused by repetitive wrist extension activities
Commonly: Rowing, skiing, tennis, canoeing and weightlifting
Friction may cause crepitus with finger/wrist extension.
Tenderness, mild swelling may be present
A Baker's cyst is a common incidental finding on ultrasound reports and bedside physical exam.
Clinically, these cysts are commonly found in association with intra-articular knee disorders. Most commonly: osteoarthritis, RA and tears of the meniscus.
Sometimes Baker's cysts are a source of posterior knee pain.
In an orthopedic clinic setting, Baker’s cysts are frequently discovered on routine MRI in patients with symptomatic knee pain. They tend to occur in adults from ages 35 to 70.
Over 90% of Baker’s cysts are associated with an intraarticular knee disorder. While most frequently associated with OA and meniscal tears, other knee pathologies that have been associated include inflammatory arthritis and tears of the anterior cruciate ligament.
DDX: DVT, cystic masses (synovial cyst), solid masses (sarcoma) and popliteal artery aneurysms.
Based on cadaveric studies, a valvular opening of the posterior capsule, proximal/medial and deep to the medial head of the gastrocnemius is present in approximately 50% of healthy adult knees.
Fluid flows in one way from knee joint to cyst and not in reverse. This valve allows flow only during knee flexion as it is compressed shut during extension due to muscle tension.
Most common patient complaint is that of the primary pathology, meniscal pain for example. At times, symptoms related to the cyst are likely due to increasing size as they may report fullness, achiness, stiffness.
In one small study, the most common symptoms were 1) popliteal swelling and 2) posterior aching. Patients may complain of loss of knee flexion from an enlarged cyst that can mechanically block full flexion.
If the Baker cyst is large enough the clinician will feel posterior medial fullness and mild tenderness to palpation. The cyst will be firm and full knee extension and softer during the flexion (Foucher’s sign).
This may help with differentiation from other popliteal masses (hematoma, soft tissue tumor, popliteal artery aneurysm).
With cyst rupture, severe pain can simulate thrombosis or calf muscle rupture, (warmth, tenderness, and erythema). A ruptured cyst can also produce bruising, which may involve the posterior calf starting from the popliteal fossa and extending distally towards the ankle.
Treatment: initial treatment for symptomatic Baker cysts is nonoperative unless vascular or neural compression is present (very unlikely)
Treatment involves physical therapy to maintain knee flexibility. A sports medicine physician may perform an intraarticular knee corticosteroid injection as this has been found to decrease size and symptoms of cysts in two-thirds of patients.
For patients that fail above, refer for surgical evaluation. Inform patients that they are not undergoing ED drainage of this symptomatic cyst due to the extremely high rate of recurrence which, as a result of the ongoing presence of the untreated intraarticular pathology, results in the recurrent effusion.
Acute lower back pain is a very common emergency department presenting complaint. Over the last several years there has been impetus to move away from opioids in the management of lower back pain.
A recent systematic review investigated the pharmacologic management of acute low back pain. This review looked at RCTs investigating the efficacy of muscle relaxants, NSAIDs, and acetaminophen for the treatment of acute nonspecific lower back pain of fewer than 12 weeks duration in patients > 18 years of age. Studies that investigated the use of opioids were not considered.
18 RCTs, totaling 3478 patients were included. 54% were women. The mean patient age was 42.5 ± 7.3 years. The mean length of follow-up was 8.0 ± 5.6 days. The mean duration of symptoms before treatment was 15.1 ± 10.3 days.
Results: Muscle relaxants and NSAIDs were effective in reducing pain and disability in acute LBP at approximately 1 week.
The combination of NSAIDs and acetaminophen was associated with a greater improvement than the sole administration of NSAIDs.
However, acetaminophen alone did not promote any significant improvement. Placebo administration was not effective.
Limitations: Most patients with acute LBP experience spontaneous recovery or at least reduction of symptoms, therefore, the real impact of most medications is uncertain. The present study wasn't able to distinguish among different classes of NSAIDs. A best practice treatment protocol cannot be extrapolated from this study.
Take home: In my practice, patients are treated with NSAIDs and Acetaminophen first line. I also include Licocaine patches for all patients. If there is a contraindication to NSAIDs, I treat with muscle relaxants alone.
This study highlights the lack of benefit of acetaminophen as mono therapy (which has been noted in other studies).
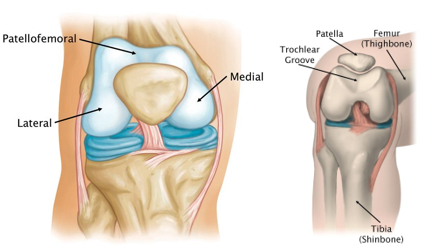
Patellofemoral anatomy and disease (part 1)
During normal knee flexion, the patella slides within the trochlear grove. Both (patella and the trochlear groove) are lined with articular cartilage at the patellofemoral articulation.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint2.jpg
Multiple forces act on the patella which can affect proper tracking: Proximately, by the quadriceps tendon, distally, by the patellar tendon, medially, by the medial retinaculum/vastus medialis and laterally by the lateral retinaculum and the vastus lateralis.
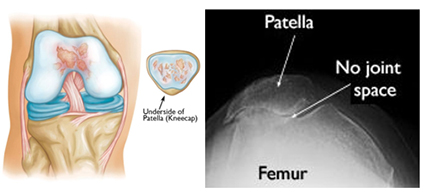
Patellofemoral OA can occur when this cartilage starts to wear and can be seen in skyline/sunrise/notch or equivalent views. OA here rarely occurs in isolation (<10%) and is usually part of medial or lateral knee OA.
https://www.stvincentsboneandjoint.com.au/images/patellofemoral-joint3.jpg
Patellofemoral pain is usually from overuse/training overload or malalignment.
Contributors to overuse involve total joint load which may have influence from training volume (total miles), intensity (competitive sports) in addition to BMI (>25) in addition to overall fitness level.
Malalignment aka abnormal patellar tracking involves both static (leg length discrepancy, hamstring tightness, etc.) and dynamic components (hip weakness, gluteus medius weakness, excessive foot pronation, etc.).
Patients with anterior knee pain should have activity modification, ice, NSAIDs (not steroids) and long-term engagement in physical therapy (>6 months) with a focus on flexibility and strengthening of lower extremity kinetic chain including the vastus medialis, gluteus medius, hip external rotators and core.
Also, consider looking for hyper supination or pronation. Foot orthotics can be of help with this.
21-year-old college softball player presents for evaluation of Left hand/wrist pain following batting practice.
She states her pinky is “tingly”
On exam, there is tenderness over her volar ulnar wrist.
You obtain an X-ray.
https://prod-images-static.radiopaedia.org/images/52314027/a662d8f338ec08ba56178463638d25_jumbo.jpeg
What’s the diagnosis?
Prolonged post-concussion symptoms are loosely defined as those lasting more than three or four weeks versus typical recovery, typically between 10-14 days.
Athletes who take longer than "typical” to recover have a challenging road of uncertainty. Medical providers are asked to make informed decisions about “normal” and expected return based on limited information.
Evaluating both athlete and parental expectations is challenging, especially when navigating difficult conversations about medical disqualification and permanently discontinuing their sport.
A 2016 study of approximately 50 patients with sports-associated concussion who had persistent symptoms lasting greater than one-month found that a collaborative multidisciplinary treatment approach was associated with significant reduction in post concussive symptoms at six months versus usual treatment.
A recent 2023 study in Neurology provides additional good news for athletes who are slow to recover from sports associated concussion. Approximately 1750 concussed collegiate athletes (diagnosed by team physician) were enrolled. In this study, slow recovery was defined as taking more than 14 days for symptoms to resolve OR taking more than 24 days to return to sport.
Approximately 400 athletes met the criteria for slow recovery (23%).
Male athletes participated primarily in football, soccer, and basketball.
Female athletes participated primarily in soccer, basketball, and volleyball.
Of the athletes who took longer than 24 days to return to play:
77.6% were able to return to play within 60 days of injury,
83.4% returned to play within 90 days, and
10.6% did not return to play at 6 months.
Slow to recover athletes averaged 35 days after injury for return to play.
This study provides valuable information for medical providers: There is an overall favorable prognosis for slow to recover concussed athletes for return to school and sport.
"The Tortoise and the Hare" fable has been used as a metaphor for the epidemiological differences between slower, low-intensity exercise versus faster, high-intensity physical activity.
"Current physical activity recommendations are predicated on the idea that both the hare and the tortoise can win the race for better health, but the provocative studies give an edge to the hare's higher-intensity approach,"
Regular physical activity is associated with significant health benefits, including decreased risk of cardiovascular disease, cancer, and all-cause mortality.
Traditional research has focused on exercise volume (150 minutes/week) over intensity.
Two recent studies looked at the benefits of shorter bouts of vigorous activity at higher intensities.
A recent large population-based cohort study of middle-aged adults used objective measurement of activity (wrist accelerometer) over self-reporting to investigate the role of exercise intensity and CV health.
Higher intensity physical activity is associated with lower rates of incident CVD.
This makes theoretical sense as greater stimulation will result in greater physiologic CV adaptations resulting in overall improved CV fitness.
For example. the authors extrapolate that an ambling 14-minute stroll has roughly the same cardiovascular benefits as an up-tempo 7-minute walk at a brisk pace.
Increasing the total amount of activity is not the only means of achieving health goals which can be met with raising overall intensity.
Vigorous physical activity is a time-efficient means to achieve overall health benefits of exercise.
A recent study (Ahmadi et al., 2022) involved 71,893 older adults with a mean age of 62.5. Authors found that quick bursts of vigorous physical activity throughout the day can lower older adults' risk of premature death by 16% to 27%, depending on daily frequency and weekly totals (from 15-20 min/week up to 50-57 min/week).
For example, doing one two-minute burst of high-intensity exercise every day for a total of 14 minutes per week was associated with an approximately 18% lower risk of all-cause mortality. The authors also found that doing as little as one to nine minutes per week of vigorous activity in quick bursts versus doing no vigorous activity was associated with significantly lower all-cause mortality risk over five years.
Exercise may not need to be a planned hour-long session at the gym for our middle-aged and older population. Accruing small amount sporadically over the day/week is an attractive option to reap the CV benefits of exercise. Existing exercise guidelines will need to be modified with future research to pinpoint the optimal exercise intensity and duration for adults in different stages of life.
Dog ownership has become more common especially during the pandemic.
Almost 70% of US households own a pet and almost half own ≥1 dogs.
There are many health benefits associated with dog ownership including: reduced risk of asthma and allergic rhinitis in children exposed to pets during early ages, improvement in symptoms of PTSD, overall wellbeing & alleviation of social isolation in elderly individuals and increased physical activity.
The main positive impact of dog ownership seems to be in relation to cardiovascular risk including an association with lower blood pressure levels, improved lipid profile, and diminished sympathetic responses to stress.
Study: A systematic review and meta-analysis (10 studies, over 3 million participants) to evaluate the association of dog ownership with all-cause mortality, with and without prior cardiovascular disease, and cardiovascular mortality. Mean follow up 10 years.
Results: Dog ownership was associated with a 24% risk reduction for all-cause mortality as compared to non-ownership (relative risk, 0.76; 95% CI, 0.67–0.86) with 6 studies demonstrating significant reduction in the risk of death.
In individuals with prior coronary events, dog ownership was associated with an even more pronounced risk reduction for all-cause mortality (relative risk, 0.35; 95% CI, 0.17–0.69). When authors restricted the analyses to studies evaluating cardiovascular mortality, dog ownership conferred a 31% risk reduction for cardiovascular death (relative risk, 0.69; 95% CI, 0.67–0.71).
The cause of this benefit is unclear. Though some activities such as the act of petting a dog has been observed to lower blood pressure levels, the mechanism for the longer survival is likely through enhanced physical activity provided by dog walking.
Conclusion: Dog ownership is associated with reduced all-cause mortality likely driven by a reduction in cardiovascular mortality. Dog ownership as a lifestyle intervention may offer significant health benefits, particularly in populations at high-risk for cardiovascular death.
Finally, meet Winston, a French bulldog who, last night, won the National Dog Show!
Opioids & NSAIDs for MSK pain in the ED: Effectiveness and Harms
Study selection: A recent systematic review in Annals of Internal Medicine attempted to evaluate the effectiveness and harms of opioids for musculoskeletal pain in the emergency department.
Included were RCTs of any opioid analgesic as compared with placebo or a nonopioid analgesic.
Conditions studied: bone injuries, soft tissue injuries, spinal pain, and mixed presentations.
Out of 2464 articles, they included 42 trials (n=6128).
Effectiveness data: Opioids were statistically but not clinically more effective in reducing pain in the short term (approximately 2 hours) versus placebo and Tylenol but were not clinically or statistically more effective than NSAIDs.
Take home: Opioids and NSAIDs may have about the same pain outcomes.
Harm data: The results on harms were very mixed. Overall, there were fewer harms with NSAIDs than opioids. However, many studies showed less of a difference. The benefit with NSAIDs due to fewer harms may be less in patients with mixed musculoskeletal conditions.
Opioids may carry higher risk for harms than placebo, Tylenol, or NSAIDs. Authors also found that an increased opioid dose may increase harms from opioids.
Limitations: Limited data on long-term outcomes and longer-term pain management
Developmental dysplasia of the hip (DDH)
Exericse as preventative medicine!
A recent cohort study of over 2,000 adults (mean age approx. 45) over approximately 11 years of follow-up investigated the association of step count with mortality.
This study found that those participants taking at least 7,000 steps per day compared to those taking fewer steps had a 50%-70% lower risk of mortality. They did not find an association with step intensity.
Another recent study investigated the dose-response association between daily step count and intensity and the incidence of all-cause dementia.
Uk based study of >78,000 adults aged 40 to 79 years with approximately 7 years of follow-up. Data from wrist accelerometer and registry-based dementia diagnoses.
Optimal step dose was 9826 steps. Minimal dose was 3826 steps (value at which the risk reduction was 50% of the observed max).
In this study, steps performed at higher intensity (112 steps/min) resulted in stronger associations.
Conclusions: A great exercise goal for middle aged and older adults is just under 10,000 steps per day to decrease risks of both overall mortality and dementia.
Limited data are available to guide recommendations re screen time after concussion.
A recent ED study looked at screen time effects on concussion recovery.
Population: 125 patients aged 12 to 25 years presenting to the ED <24h after injury. Mean age 17. Approximately 51% male.
Intervention: Patients were placed in a screen time allowed group and a screen time not allowed group for the first 48 hours. Total minutes reported after the study were 630 minutes vs 130 minutes.
Outcome: Time to symptom resolution. Patients took daily symptom scoring tests for 10 days.
Result: Screen time allowed group had a significantly longer time to recovery (8 days) vs screen time not allowed (3.5 days).
Strength: Good attempt at quantifying effects on early screen time exposure on symptom recovery in an ED population.
Weakness: This was a small study. Many patients (>25%) were lost to follow-up and it relies on symptom self-reporting.
The hip joint is a very strong and stable structure requiring great force to produce a dislocation
Most hip dislocations are posterior (80-90%)
Mechanism: MVC generating force onto an adducted flexed hip (most commonly)
Associated injuries occur both locally (acetabular fx) and distant (knee bone and ligamentous)
Significant associated injuries in >70%
The hip joint has a very precarious blood supply.
One of the risk factors for AVN is total dislocation time
<6 hours - 5% incidence
>6 hours – up to 53% incidence
Examine the sciatic nerve carefully with posterior dislocations (10% incidence)
Motor – EHL/ankle dorsiflexion
Sensory – sensation dorsum of foot
There are many reduction maneuvers including the East Baltimore Lift technique
https://www.youtube.com/watch?v=1zvelGbVn04
Demonstrated at 30 seconds in above video
Place patient supine with affected leg flexed to 90 degrees at knee and hip. 2 providers position themselves on opposite sides of the patient and each places their arm under the patient’s calf/popliteal region and their hand on the opposite providers shoulder. A 3rd person is required to stabilize the pelvis. Axial traction is generated by the providers slowly standing up. Gentle internal and external rotation can facilitate successful reduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}