This Canadian study looked at the safety of paramedics using the modified Canadian C-Spine Rule to determine which pre-hospital blunt trauma patients required immobilization. These were MVC and fall patients predominately. Bottom line: appropriately trained paramedics can use the modified Canadian C-Spine rule to clinically clear cervical spines in the field.

| Result of Application | Paramedics’ Interpretation | Investigators’ Interpretation |
|---|---|---|
| Injury | No Injury | Injury |
| --- | --- | --- |
| Immobilization required (N) | 10 | 1,342 |
| Immobilization not required (N) | 1 | 2,668 |
| Sensitivity, % (95% CI) | 90.9 (58.7–99.8) | 90.9 (58.7 to 99.8) |
| Specificity, % (95% CI) | 66.5 (65.1–68.0) | 68.2 (66.7 to 69.7) |
| Positive likelihood ratio, (95% CI) | 2.7 (2.2–3.4) | 2.9 (2.4 to 3.5) |
| Negative likelihood ratio (95% CI) | 0.1 (0.0–0.9) | 0.1 (0.0–0.9) |
This meta analysis looked for studies involving community EMS (CEMS) interventions trying to reduce falls. The authors found:
“CEMS fall prevention interventions reduced all-cause and fall-related emergency department encounters, subsequent falls and EMS calls for lift assist. These interventions also improved patient health-related quality of life, independence with activities of daily living, and secondary health outcomes.”
Further, prospective work needs to be done to look at this on a larger scale. We know falls in elderly patients lead to significant morbidity and mortality. This could be one way to improve fall mortality.
The use of seizure prophylaxes in moderate to severe head injury has been recommended for 7 days post-injury. In general, levetiracetam is used for seizure prophylaxes in this group of patients. This study looked retrospectively at high (over 500 mg BID) vs. low (500 mg bid) dosing and found there was no difference in seizure events in either group. Overall 6% of patients had a seizure in this seven day window even with medication given.
Predicting which blunt abdominal trauma patients have mesenteric or bowel wall injuries early in their ED course will decrease morbidity and mortality. It is also a challenge even in the age of advanced CT imaging. This study from India looks at the Bowel Injury Prediction Score as a possible means to catch these injuries early in the course of care. The score uses white blood cell count over 17,000 (1 point), abdominal tenderness at the time of presentation(1 point), as well as a McNutt's scoring scale grade 4 (1 point) (table). The study found those with a score greater than 2 (out of 0-3) were much more likely to have bowel or mesenteric injury at time of laparotomy. Tenderness and CT findings were more likely to be predictive of bowel injury than WBC greater than 17,000. “BIPS had 94.5% sensitivity, 72% specificity, 88% PPV, and 86% NPV for identifying patients with sBBMI.”
My take away is an abnormal CT scan or significant tenderness of presentation warrant concern for mesenteric or bowel wall injury and surgical evaluation is appropriate for these patients. An elevated or normal white blood cell count isn't helpful in these patients. Surgeons may use this scale to help them decide if a patient warrants a trip to the operating room
| GRADE | FINDING |
|---|---|
| 1 | Isolated mesenteric contusion without associated bowel wall thickening or adjacent interloop fluid collection |
| 2 | Mesenteric hematoma?<?5 cm without associated bowel wall thickening or adjacent interloop fluid collection |
| 3 | Mesenteric hematoma?>?5 cm without associated bowel wall thickening or adjacent interloop fluid collection |
| 4 | Mesenteric contusion or hematoma (any size) with associated bowel wall thickening or adjacent interloop fluid collection |
| 5 | Active vascular or oral contrast extravasation bowel transaction or pneumoperitoneum |
In this systemic literature review of orthopedic injuries identified in intimate partner violence (IPV) the authors remind us that finger, hand, and especially isolated ulnar fractures are very commonly associated with IPV. When we see these injury patterns extra effort is required to determine if IPV is involved.
| Citation | **Bhandari et al.**3 | **Khurana et al.**18 | **Loder et al.**12 | **Porter et al.**13 | **Kavak et al.**7 | **Thomas et al.**17 |
|---|---|---|---|---|---|---|
| Division of injury locations | Fingers, wrist, shoulder dislocation, humerus fracture | Finger, hand, wrist, forearm, elbow, humerus, shoulder | Finger, hand, wrist, forearm, elbow, humerus, shoulder | Radius/ulna, humerus, upper extremity, right/left | Phalanx, radius, ulna (diaphysis/metaphysis, distal/proximal) | Phalanges (distal/medial/proximal), hand/finger, forearm, arm/shoulder right/left |
| Most common UEF location | Fingers (n = 11) | Finger (34.3%) | Finger (9.9%) | Radius and ulna (n = 80; 5.9%) | Ulna (14.5%) | Finger (46%) |
| Most common injury type‡ | Musculoskeletal sprains (all n = 21; 28% back n = 7; neck n = 6) | UEF (27.2%) | Contusions/abrasion (43.4%) | Rib fracture (17.5%) | Soft-tissue lesions (n = 1,007, 82.2%) | UEF (52%) |
* IPV = intimate partner violence, UEF = upper extremity fracture, and UEI = upper extremity injury.
† Summary table demonstrating the location prevalence of UEIs caused by cases of IPV. Fractures were quantified separately from other UEIs in this specific table.
‡ In all included articles the most common injury type was an injury to the head or neck; these are excluded because of the study aim.
This retrospective study of Swiss trauma patients looked at blood gas oxygen levels within 3 hours of arrival to the trauma bay in severely injured patients over age 16. When comparing hypoxic, hyperoxic and normo-oxic patients there was no difference in 28 day mortality. Those with above normal oxygen levels tended toward longer hospital stays. The above normal oxygen cohort also were more likely to be intubated in the field.
This study fits with others showing around 20% of trauma patients arrive to our trauma bays over oxygenated. More research is needed to see the impact this has on care. Be mindful of over oxygenation especially in intubated trauma patients.
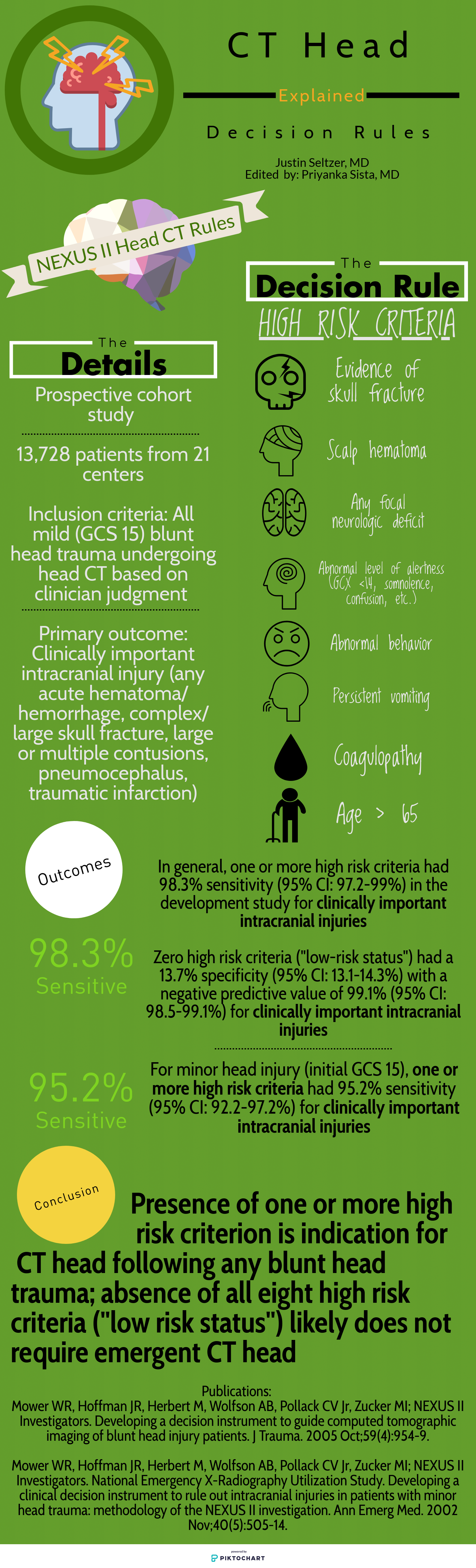
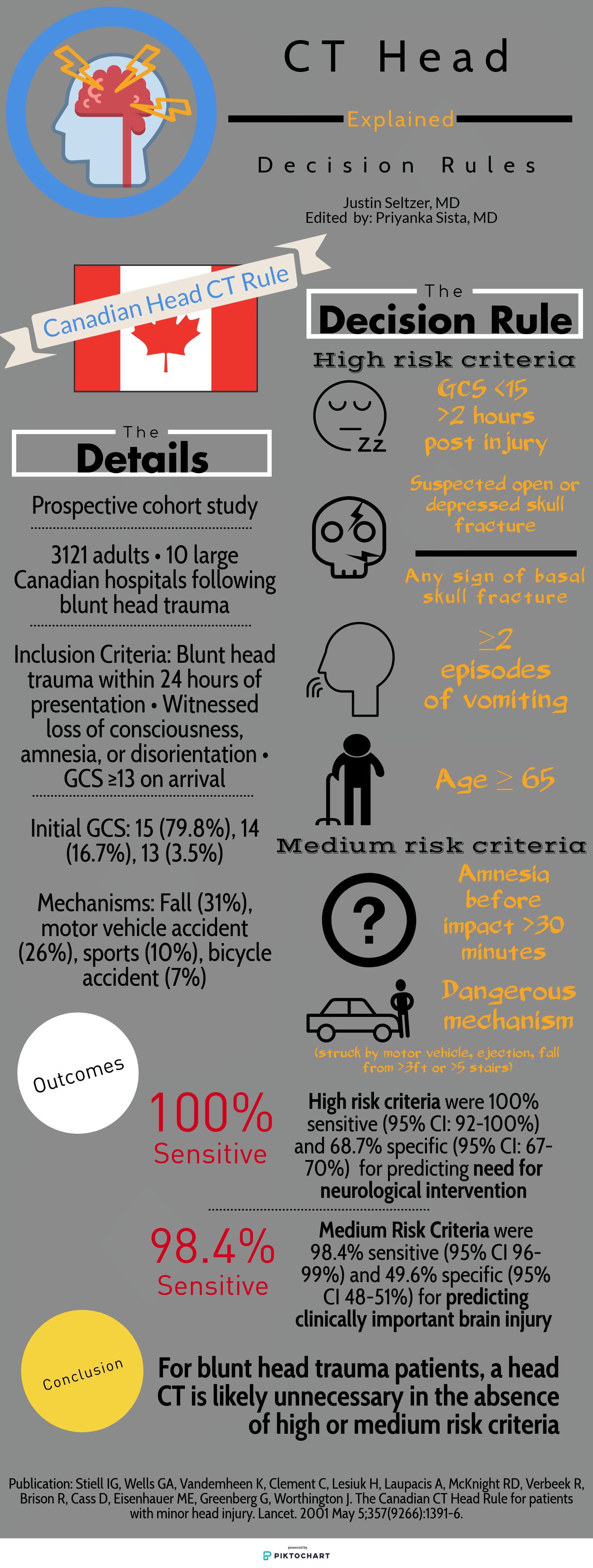
Deciding who needs exposure to radiation after blunt head injury has been looked at by both the Canadian Head Injury Guidelines as well as NEXUS. This website has excellent graphics outlining the rules. Note age over 65 alone is predictive of significant intracranial injury. All recent studies indicate age over 65 even with a low suspicion mechanism such as fall from standing is still a significant risk for intracranial pathology.
A study looking at patients over age 65 with head injuries from falls assessed the association of alcohol use with severity of injury. The alcohol use was self-reported which does limit the findings. The study found “Of 3128 study participants, 18.2% (n = 567) reported alcohol use: 10.3% with occasional use, 1.9% with weekly use, and 6.0% with daily use.” Those daily drinkers had a higher incidence of intercranial injuries.
The authors concluded: “Alcohol use in older adult emergency department patients with head trauma is relatively common. Self-reported alcohol use appears to be associated with a higher risk of ICH in a dose-dependent fashion. Fall prevention strategies may need to consider alcohol mitigation as a modifiable risk factor.”
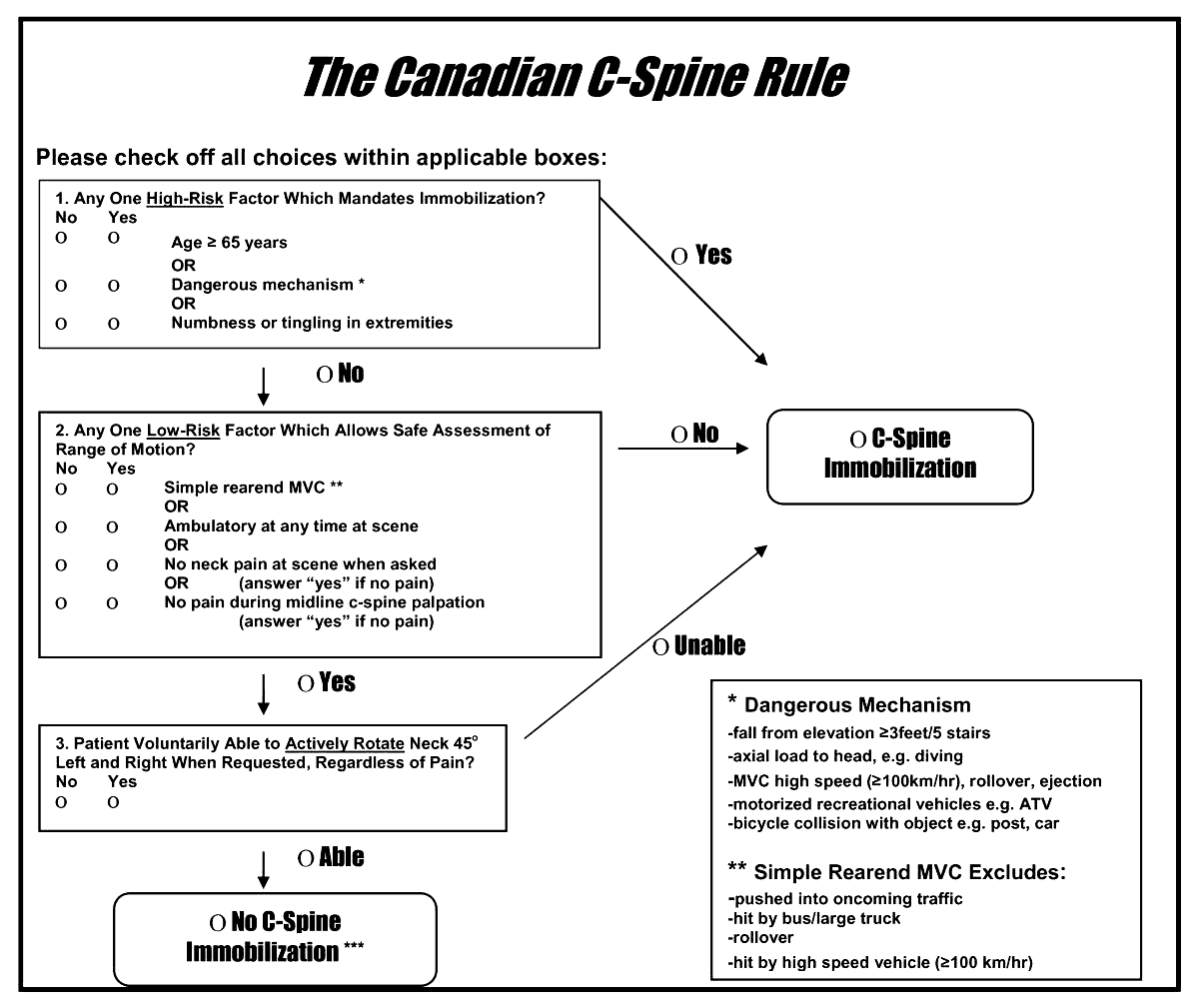
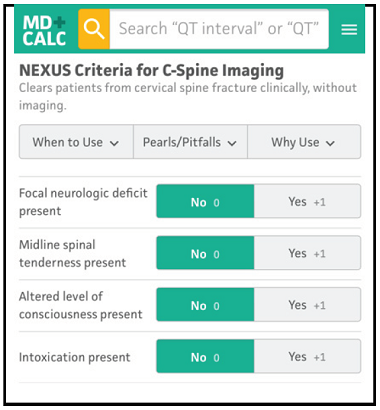
A reminder of two validated tools used to determine the need for cervical spine imaging in adult blunt trauma patients. A recent meta analysis concluded:
“Based on studies, both CCR and NEXUS were sensitive rules that have the potential to reduce unnecessary imaging in cervical spine trauma patients. However, the low specificity and false-positive results of both of these tools indicate that many people will continue to undergo unnecessary imaging after screening of cervical SCI using these tools. In this meta-analysis, CCR appeared to have better screening accuracy.”
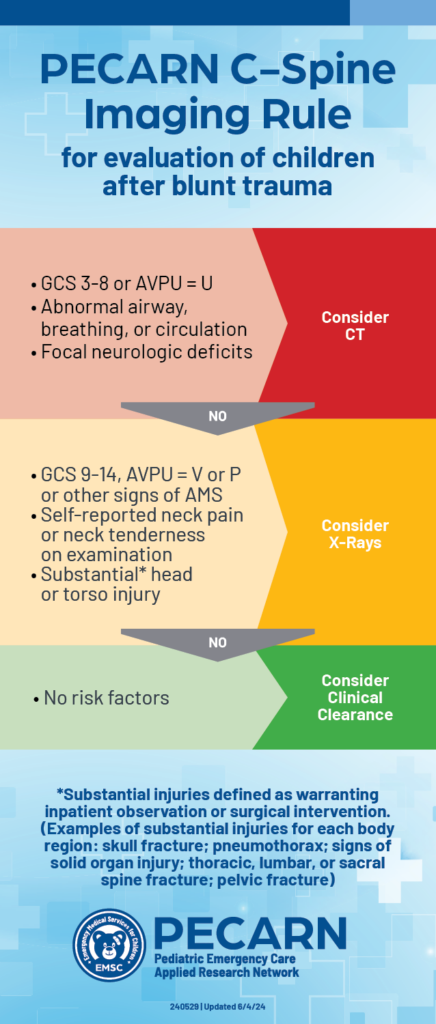
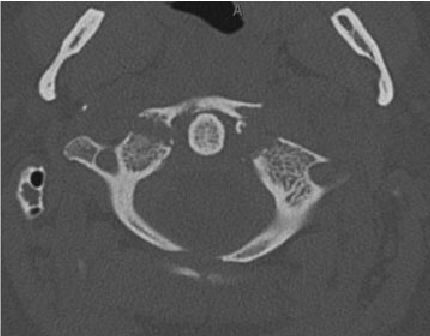
A just released study published in the Lancet gives us guidance on which pediatric blunt trauma patients need cervical spine imaging. Age range was 0-17 years.
“Out of 22,430 children included in the study, 433 (1.9%) were found to have Cervical spine injury (CSI). The study identified 4 high risk factors for CSI to be used to triage children to CT (12% risk for a cervical spine injury):
In children without high-risk findings, 5 additional findings identified children with intermediate, non-negligible risk of CSI (3.6% risk of a cervical spine injury):
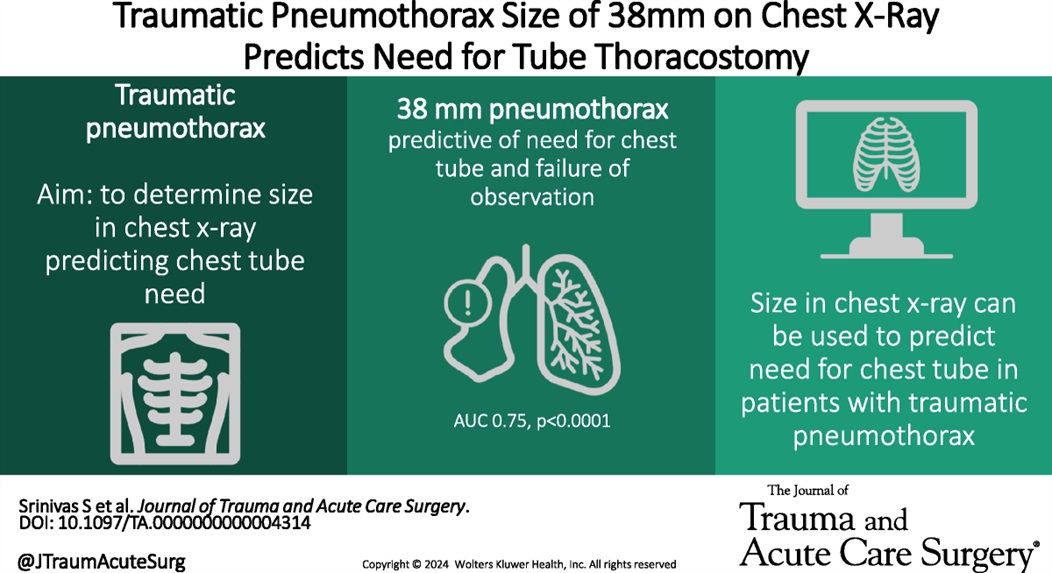
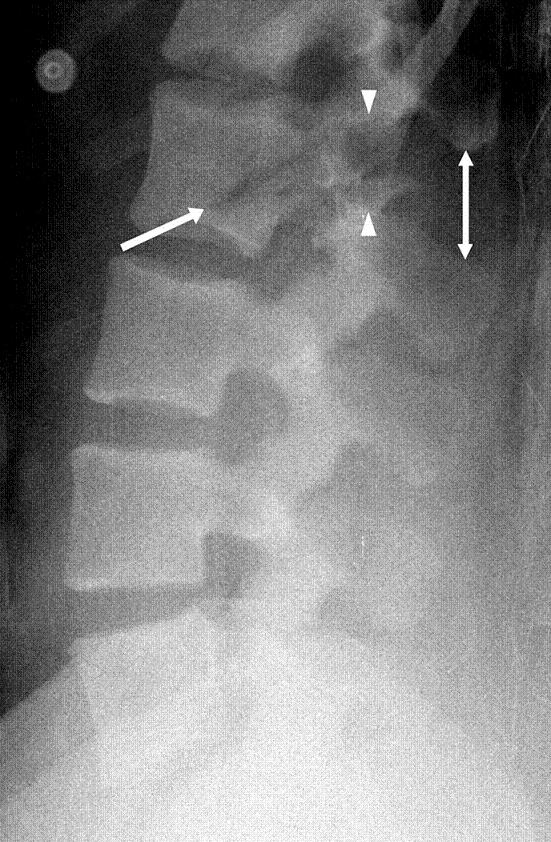
A cut-off of 35mm on CT scan has been shown to be predictive of which traumatic pneumothoracies require thoracostomy tube placement vs. safety of observation. This retrospective study looked at chest X-ray findings to see if there was a similar size cut-off where patients could be safely observed rather than undergo this invasive procedure. They found 38mm was the size over which observation failed. Of note, lactic acidosis and need for supplemental oxygen also predicted the need for chest tube placement
In this prospective, observational study of trauma patients with isolated head trauma, 62% of patients developed post-intubation hypotension. Comparing patients receiving hypertonic saline, vasopressors, crystalloid, or blood those receiving hypertonic saline and vasopressors had less post-intubation hypotension.
TBI patients who develop hypotension have worse outcomes. This study reminds us the use of vasopressors in trauma patients to maintain blood pressure is appropriate in the correct circumstances.
According to this study, no TXA 2g bolus was not found to increase the number of seizures in TBI pts.
TXA has been shown to improve mortality in inter cranial hemorrhage trauma patients if given within 2 hours. TXA is also known to lower seizure threshold. This study was a secondary analysis of a larger study comparing placebo to 1 g TXA bolus plus 8 hour infusion or 2g bolus TXA in the prehospital setting. There was no difference in the number of pts experiencing seizure or outcome in those receiving the 2g bolus of TXA.
Patient struck in left eye. The patient was asked to look up during exam and this is the finding. What imaging modality would you order if so inclined, what is the injury, and what is the disposition/plan?

192 trauma patients who were receiving pre-hospital fentanyl for moderate to severe pain were randomized to placebo or intranasal 50 mg ketamine as an adjunct for pain control. There was no difference between the two groups in decrease in pain scale.
The authors concluded: “In our sample, we did not detect an analgesic benefit of adding 50 mg intranasal ketamine to fentanyl in out-of-hospital trauma patients.”
A prospective European study of patients over age 65 presenting with a ground level fall obtained troponin levels to ascertain if myocardial infarction was a cause of the ground level fall. Troponin levels were elevated in a majority of patients however only 0.5% were defined as having a myocardial infarction. Of the 3% who died within 1 year, troponin was found to be higher than those that survived the one-year study period. The authors concluded “Our data do not support the opinion that falls may be a common presenting feature of MI. We discourage routine troponin testing in this population. However, hs-cTnT and hs-cTnI were both found to have prognostic properties for mortality prediction up to 1?year.”
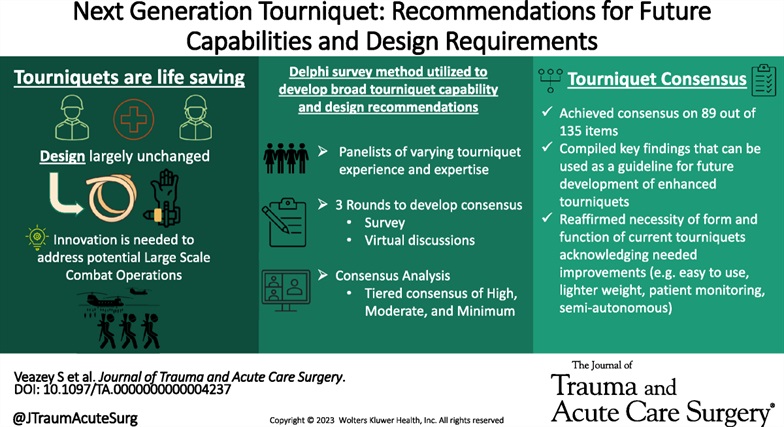
Appropriately, a great deal of time and energy is being expended to educate on the use of tourniquets to prevent mass hemorrhage. Are the current generation of tourniquets the best that we can have? These authors performed a Delphi study to assess needs with tourniquet design.
They concluded the next generation of tourniquets should have the following: “Capable of being used longer than 2 hours, applied and monitored by anyone, data displays, semiautomated capabilities with inherent overrides, automated monitoring with notifications and alerts, and provide recommended actions.”
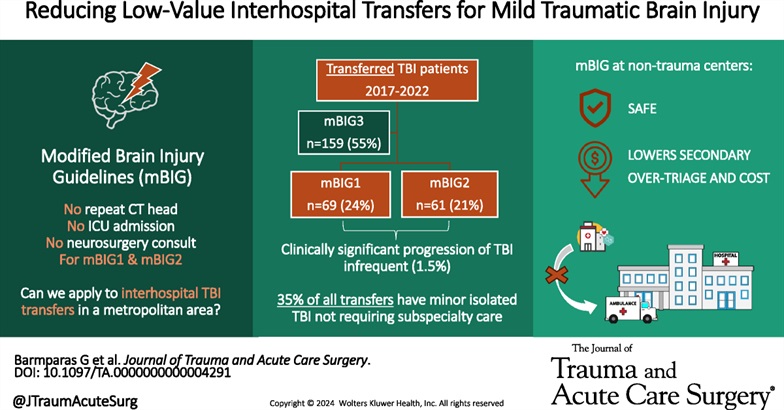
This study used the modified Brain injury Guidelines retrospectively to assess whether the guidelines would have saved transfers to their level one facility safely. They concluded the guidelines would have effectively prevented unnecessary mBIG 1 and mBIG2 transfers with no patient harm.
TABLE 1 - Modified Brain Injury Guidelines Radiologic Stratification, as per Kahn et al.
| mBIG 1 | mBIG 2 | mBIG 3 | |
|---|---|---|---|
| Skull fracture | No | Non-displaced | Displaced |
| SDH | ?4 mm | 4–7.9 mm | ?8 mm |
| EDH | No | No | Yes |
| SAH | ?3 sulci and <1 mm | Single hemisphere or 1–3 mm | Bihemisphere or >3 mm |
| IVH | No | No | Yes |
| IPH | ?4 mm | 4–7.9 mm | ?8 mm or multiple |
EDH, epidural hematoma; IPH, intraparenchymal hemorrhage; IVH, intraventricular hemorrhage; SAH, subarachnoid hemorrhage.
-668ade5e780f0.jpg)