Lead is a ubiquitous metal in the environment partly due to decades of using leaded gasoline (organic lead) and lead-based paint (inorganic lead). Outside of occupational exposure, children are disproportionately affected from environmental lead exposure.
Common route of exposure are:
Majority of the absorbed lead are stored in bone (years) > soft tissue (months) > blood (30-40 days) (half-life). Thus blood lead level does not accurately reflect the true body lead burden.
Incidence of elevated blood lead level (EBLL > 5 microgram/dL) in children increased from 2.9 to 4.9% in Flint, MI before and after water source change. In the area with the highest water lead level, the incidence increased by 6.6%.
Clinical manifestation in children
| Clinical severity | Typical blood lead level (microgm/dL) |
| Severe
| > 70 – 100 |
| Mild to moderate
| 50 – 70 |
| Asymptomatic
| > 10 |
Evaluation for lead poisoning
Management of children with EBLL
The three-bag IV acetylcysteine regimen for acetaminophen overdose is complicated and can result in medication/administration errors. [1] Two recent studies have attempted simplifying the regimen using a two-bag approach and evaluated its effect on adverse effects. [2, 3]
Study 1 [2]
Prospective comparison of cases using a 20 h, two-bag regimen (200 mg/kg over 4 h followed by 100 mg/kg over 16 h) to an historical cohort treated with the 21 h three-bag IV regimen (150 mg/kg over 1 h, 50 mg/kg over 4 h and 100 mg/kg over 16 h).
The two-bag 20 h acetylcysteine regimen was well tolerated and resulted in significantly fewer and milder non-allergic anaphylactic reactions than the standard three-bag regimen.
Study 2 [3]
Prospective observational study of a modified 2-phase acetylcysteine protocol. The first infusion was 200 mg/kg over 4-9 h. The second infusion was 100 mg/kg over 16 h. Pre-defined outcomes were frequency of adverse reactions (systemic hypersensitivity reactions or gastrointestinal); proportion with ALT > 1000 U/L or abnormal ALT.
The 2-phase acetylcysteine infusion protocol resulted in fewer reactions in patients with toxic paracetamol concentrations.
Final word: Two-bag regimens seem to offer advantages compared to the traditional three-bag regimen with regard to reduced adverse drug reactions. Look for more data, particularly on effectiveness, and a potential transition to a two-bag approach in the future.
Caffeine is the most commonly used psychoactive substance in the world. It is widely available in coffee, tea, chocolate,soft drinks, OTC medicines, and energy drinks. The vast majority of people consuming caffeine appear to suffer no harm while enjoying it's stimulating effects. This has led to the widely held perspective that caffeine is a completely benign substance with no adverse health effects exists.
Although, children and adolescents are at particular risk, many caffeine containing products are specifically marketed at them. Alarmingly, statistics demonstrate that caffeine intake among children and adolescents has increased by 70% in the last 30 years. Energy drinks are of special concern as they represent the fastest growing component of the beverage industry, contain significant quantities of caffeine as well as high levels of sugar, and can place children at high risk for caffeine intoxication.
There are many negative health consequences documented with caffeine use which occur in a dose dependent manner with individuals differing in their susceptibility to caffeine-related adverse effects:
Chronic Effects:
The American Academy of Clinical Toxicology's Lipid Emulsion workgroup has published its first of 4 systematic reviews on the use of lipid emulsion in toxicology, this one on lipid's effect on laboratory analyses. [1] As expected, administering a fat bolus can significantly alter labs drawn subsequently.
The key point: If you are considering lipid for overdose, draw labs prior to giving it.
Which labs are affected? Most. Here's a helpful mnemonic courtesy of Dr. Kyle DeWitt.
Also remember to give lipid in its own line. It isn't compatable with most resuscitation drugs. [2]
Carbon monoxide (CO) is a colorless, odorless, tasteless toxic gas produced by incomplete combustion in fuel-burning devices and is a leading cause of poisoning morbidity and mortality.
Symptoms can be easily misinterpreted (e.g., headache, nausea, dizziness, or confusion) thus victims may not realize they are being poisoned.
CO detectors use an audible alarm and are effective in alerting potential victims of presence of CO. Some versions offer a digital readout of the CO concentration. Detectors are not a simple alarm level (as in smoke detectors) but are a concentration-time function.
In the UL 2034 Standard, Underwriters Laboratories specifies response times for CO alarms:
Current Occupational Safety and Health Administration permissible exposure limit for CO is 50 parts per million as an 8-hour time-weighted average concentration.
CO detectors have a limited lifespan of up to 7 years.
Forty percent of residential detectors studied failed to alarm in hazardous concentrations, despite outward indications that they were operating as intended.
CO detectors 10 years and older had the highest failure rates.
Electronic cigarettes have been gaining popularity in the U.S. as a smokeless delivery system for nicotine. These devices require liquid nicotine (e-liquid) that are vaporized and inhaled (vaping).
E-liquid can have nicotine concentration as high as 100 mg/mL, which are diluted prior to use. When ingested in high concentration and in sufficient volume (1 vial = 15 mL) patients can develop significant nicotinic toxicity. Recently a case of cardiac arrest has been reported after ingesting two 15 ml vial (100 mg/mL).
Nicotine mimics the effects of acetylcholine (Ach) release by binding to nicotinic receptors located in:
Clinical manifestation of toxicity (similar to cholinergic toxidrome) is biphasic with early central stimulation followed by depression. (see table below)
|
| GI | Respiratory | Cardiovascular | Neurologic |
| Early (1 hr) | Nausea Vomiting Salivation Abdominal pain | Bronchorrhea Hyperpnea | Hypertension Tachycardia Pallor | Agitation Anxiety Dizziness Blurred vision Headache Hyperactivity Tremors Fasciculation Seizures |
| Late (0.5-4 hr) | Diarrhea | Hypoventilation Apnea | Bradycardia Hypotension Dysrhythmias Shock | Lethargy Weakness Paralysis |
Management: There is no specific antidote or reversal agent. The management of nicotine toxicity focuses on organ-specific dysfunction.
Not to be outdone by the recent FDA approval of Idarucizumab to reverse dabigatran, a new factor Xa reversal agent is under investigation. "Andexanet binds and sequesters factor Xa inhibitors within the vascular space, thereby restoring the activity of endogenous factor Xa and reducing levels of anticoagulant activity, as assessed by measurement of thrombin generation and anti factor Xa activity, the latter of which is a direct measure of the anticoagulant activity."
Design
Two parallel randomized, placebo-controlled trials (ANNEXA-A [apixaban] and ANNEXA-R [rivaroxaban]) were conducted in healthy vounteers to evaluate the ability of andexanet to reverse anticoagulation, as measured by the percent change in anti factor Xa activity after administration.
What they Found
Compared to placebo, andexanet significantly reduced anti-factor Xa activity, increased thrombin generation, and decreased unbound drug concentration in both the apixaban and rivaroxaban groups.
Application to Clinical Practice
Designer drugs are structural or functional analogs of controlled substances produced to mimic pharmacological effects of the original compound while circumventing legal restrictions and detection on drug screens. Considered "legal highs" by the public, these highly potent drugs are produced in clandestine laboratories with no regulations for quality control or clinical testing for phamacological effects and thus present major threat to public health. Examples include synthetic hallucinogens (DOM: STP), opiates ( methylfentanyl:china white), stimulants (methamphetamine:crank, MDMA: ecstasy, cathinones:bath salts) and synthetic cannabinoids (spice).
The synthetic cannabinoids are the newest designer drugs and numerous cases of intoxication are being reported including some fatalties.Cannabinoids fall into 3 classes: endocannabinoids, phytocannabinoids, synthetic. Marijuana, the best known cannabinoid is plant derived and its psychoactive effects are mainly due to delta-9-tetrahydrocannabinol (THC) which binds with the endocannabinoid receptors CB1 and CB2 found throughout the central and peripheral nervous system and peripheral organs. The CB receptors interact with opiate receptors which is likely responsible for the analgesic effect.
Since 1984, the John Huffman research group at Clemenson University synthesized over 450 cannabinoid compounds for biomedical reseach known as "JWH compounds". These compounds hold great promise in the investigation of multiple diseases and development of new novel therapies. Over the last several years, these cannabinoid compounds began cropping up sprayed onto herbs marketed in colorful packets and sold on the internet, convienence stores, and head shops. Although clearly labeled as "not for human consumption" considered on the street as a legal alternative to marijuana.
Key Points:
There have been a variety of case reports that have been describing the effects of lipid emulsion therapy on severe hemodynamic overdoses. As time has gone on, we have realized that this therapy is not for all severe overdoses. The type of medication and its pharmacokinetic properties factor into the decision. There is minimal evidence and no ideal randomized control trials that will tell us what the right answer is but take beta-blockers for instance:
Atenolol - in overdose, consider hemodialysis, very effectively removed by HD [1]
Propranolol - very lipophilic and one of the few beta-blockers that can cause widened QRS, seizures as well as the prototypical hypotension and bradycardia.
Because of its lipophilicity, ability to cross the blood brain barrier and ability to cause lethal dysrrthmias, lipid emulsion therapy has been effective in reversing the clinically severe effects of a propranolol overdose. [2]
Toxicity due to body packing and body stuffing can be a significant concern due to unknown quantity and/or substance that was ingested.
A recent prospective observational case series compared the utility of CT abdomen/pelvis with and without PO contrast in identifying the ingested packets.
The gold standard comparison: surgical removal or expulsion of packets.
All patients received CT abd/pelvis with and without PO contrast.
A. Body stuffers (n = 24)
CT w/ PO contrast:
Positive: 7 (sensitivity 29.2%)
Negative: 17
CT w/o PO contrast:
Positive: 9 (sensitivity 36.5%)
Negative: 15
All 24 patients passed ingested packets
B. Body packers (n= 11)
CT w/ PO contrast
CT w/p PO contrast
10 patients expulsed packets; one patient did not have any packets.
Conclusion
Bottom line:
In patients receiving renal replacement therapy as a treatment modality for dabigatran-related bleeding, watch for a rebound concentration increase after hemodialysis is stopped.
More than 50% of patients demonstrate a rebound effect with a median increase in dabigatran concentration of 33%.
It is unclear whether this rebound effect is clinically important, and whether it translates to prolonged clinically relevant bleeding. Extended hemodialysis sessions or consideration of CVVHD should offset this potential problem.
Bonus Pearl:
The North American Congress of Clinical Toxicology starts today and runs through October 12. Look for toxicology pearls and updates on Twitter under the official conference hashtag #NACCT15.
Monosodium glutamate
Metabisulfites (Na sulfite, Na/K bisfulfite, Na/K metabisulfite, etc.)
Tyramine reaction
Niacin
Trichloroethylene
Scrombroids
Hydroxocobalamin
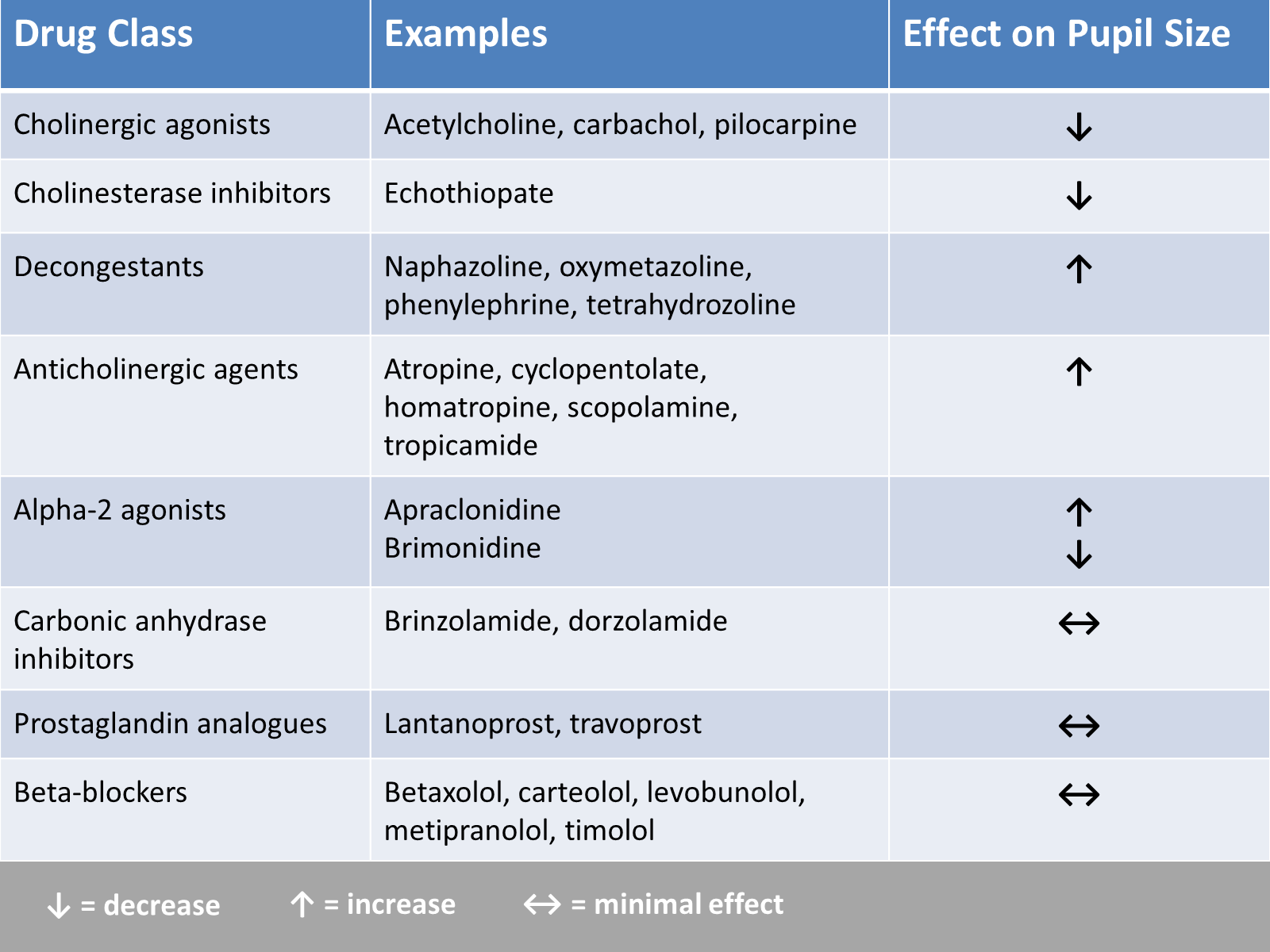
In the evaluation of ED patients, it may be important to understand the effect on pupil size from the ophthalmic medications they use. Here is a summary chart of common eye drops and their effect on pupil size.
People who hide illicit drugs can be classified in to three different types.
1. Body stuffers – people who ingest drugs that are poorly wrapped to “eliminate” evidence from police – e.g. street dealers.
2. Body packers – people who ingest large amounts of “well” packed drug packets to transport drugs (usually internationally) – aka “mule.”
3. Body pushers – people hiding drugs in rectum or vagina.
Body stuffers are more frequently encountered in local ED compared to body packers. Stuffers can become symptomatic as the ingested drugs (cocaine, heroin, amphetamines) are often poorly wrapped (e.g. in plastic bag/wrap, cellophane paper, aluminium oil, etc.).
Recent retrospective article looked at the utility of 6-hour observation period in the ED as a management strategy for body stuffers. (n=126)
Characteristics
1. Ingested drugs (self-reported): heroin (48%), cocaine (46%), other drugs [cannabis, MDMA, diazepam, methamphetamine] (16%), unknown (8%)
2. Time of ingestion to ED presentation
Clinical findings
76% of the patients experience clinical signs of toxidrome at time of presentation.
Most common findings:
Patients who ingested heroin were more symptomatic vs. cocaine (87% vs. 70%)
Patients were discharged:
Conclusion
Flumazenil is generally avoided in most adult patients with suspected benzodiazepine overdose due to resedation, seizures/withdrawal, inconsistent reversal of respiratory depression, and the potential for proconvulsant coingestants.
Three relatively recent poison center studies have attempted to demonstrate the safety of flumazenil in this setting. [1-3] In the first study there were 904 adult patients with 13 reported seizures and 1 death. [1] A second study specific to pediatric patients reported 83 patients with no seizures and no deaths. [2] A third study found 80 patients with 1 seizure and 0 deaths. [3]
On the surface, it may appear that flumazenil is safe to give. But, retrospective poison center studies from voluntary reporting cannot be used to prove a drug's safety. The true denominator is unknown. In the pediatric study, we wouldn't expect children to experience withdrawal since they aren't on chronic benzodiazepine therapy. [2] So, it's no surprise there weren't any seizures or deaths.
A recent systematic review and meta-analysis of randomized trials summed it up perfectly: "Flumazenil should not be used routinely, and the harms and benefits should be considered carefully in every patient." [4] Cases in which to consider flumazenil are pediatric patients and reversal of procedural sedation if needed.
Poison ivy, oak, and sumac (Toxicodendron sp) causes a highly puritic, allergic contact dermatitits (ACD) that affects between 10 and 50 million in the US every year. It is a significant occupational hazard as well a scourge for outdoor enthusiasts.
Toxicodendron species contain oleoresins, known as Urushiol compound, secreted by all parts of the plant. Contact with the oil usually occurs by brushing against or direct handling of the plant or contaminated items. This toxin triggers a type IV delayed hypersensitivity reaction in approximately 75% of the population. Within 12-24 hours an erythematous, often linear, vesicular rash develops but new lesions can occur up to 2 weeks later.
There is no ideal treatment for ACD induced by Toxicodendron species. Avoidance and barrier protection are the best strategies. Recommended medications include antihistamines, topical preparations, and systemic steroids. However, steroids require a 2-3 week course to prevent recrudescence of the rash and are not without undesirable side affects.
Zanfel, an OTC granular polyethlene paste, removes urushiol by binding with it to create an aggregate cluster that can be washed away with water. It is highly effective, providing rapid relief even as a sole agent but requires multiple initial applications and is expensive. Mean Green hand scrub has similar ingredients and is claimed to bond urushiol also. Excessive scrathing and abrasive scrubs can cause secondary cellulitis requiring antibiotics.
Oral hypoglycemic agents (e.g. sulfonylureas) can cause symptomatic hypoglycemia. Unlike metformin, sulfonylureas stimulate the release of insulin from beta-cells (in pancreas) in response to serum glucose level.
ED management of hypoglycemia involves:
However, for recurrent hypoglycemia (> 3 episodes of hypoglycemia), think about octreotide, rather than starting a dextrose (D5) infusion.
For example, D5 infusion at 150 mL/hour has only 7.5 gm of dextrose (calculation: D5% = 5gm/100 mL). One gram of dextrose contains about 4 calories (equivalent to one piece of Skittles) So, with a D5 infusion at 150 mL/hour, you are giving your patients 8 pieces of Skittles per hour. A bottle of Snapple lemon ice tea (non-diet) has more calories (150 calories in 16 oz. or 473 mL)!
Octreotide 50 mcg SQ (q6 hour) injection will decrease the insulin release from the beta-cell by blocking the voltage-gated Ca channel on the beta-cell.
All patient who received octreotide in the ED requires admission to the hospital for observation. Patients can be safely discharge from the hospital when finger stick glucose level remains normal for 24 hours after the last dose of octreotide.
Bottom line: In sulfonylrea-induced recurrent hypoglycemia, administer octreotide, rather than continuous infusion of dextrose (D5) solution.
Physostigmine is a cholinergic agent (acetylcholine esterase inhibitor) that can be used to reverse anticholinergic toxicity. Its use has been declining since the publication of several case reports of physostigmine induced cardiac arrest in tricyclic antidepressant (TCA) overdose.
The first case report (and often cited) was by Pental P. et al. (Ann Emerg Med 1980), who presented 2 cases (32 and 25 year old) of asystole after administration of physostigmine (2 mg) in severe TCA overdose. These two cases both had widened QRS interval (120, 240 msec) due to TCA poisoning. Bradycardia preceded the asystole.
The second case report (Shannon M Pediatr Emerg Care 1998) reported a 15 year-old girl with QRS widening (120 msec) received 2 mg of physostigmine and developed severe bradycardia and then asystole.
Another case series (Knudson K et al. BMJ 1984) of 41 patients with overdose of maprotiline showed that physostigmine administration was associated with higher incidence of seizures. No asystole was noted.
Today physostigmine is contraindicated in TCA poisoning. But if we think about it, physostigmine administration probably wasn’t a good idea in the first place. Correcting anticholinergic toxicity of TCA has limited benefit; mortality from TCA overdose is usually associated with cardiac toxicity (Na-channel blockade) and should be treated with NaHCO3 administration
Physostigmine still has a role in treating isolated anticholinergic toxicity (e.g. diphenhydramine, benztropine, dimenhydrinate, scopolamine, jimson weed overdose). Prior to physostigmine administration:
Bottom line: If you suspect isolated anticholinergic toxicity, think about physostigmine. Like any medication, risk and benefit of administration should be considered prior to administration.
The New England Journal of Medicine and Lancet both published studies evaluating idarucizumab for reversal of dabigatran. It is a monoclonal antibody fragment that binds dabigatran with high affinity. Dr. Ryan Radecki summarizes the two articles on his EM Lit of Note blog.
Here are a few take home points from these early studies: