Systemic racism and institutional bias affect all aspects of medicine. This position paper from 2022 highlights some of the disparities present within the EM Clinical Ultrasound community. The authors identified several areas of concern regarding the make up of the leadership of the CU community, and importantly suggest several ways to create a more equitable specialty.
Have you tried using Large Language Model (LLM) driven searches in clinical practice, for example, OpenEvidence, ChatGPT, or Claude?
A recent paper, far from medicine, argues that LLM searching has changed the way we think about search and what we expect from search.
We have moved from searching for sources to searching for the information contained within sources. With this, our expectations have changed – we expect search to provide answers, not documents.
With this shift, the foundations of trust have shifted. Rather than finding a document that provides the answer, and which is supported by the integrity of the authors and publishers – and which the reader can evaluate – LLMs provide an answer, often with little evidentiary base to support that answer.
Some LLMs do a better job of referencing sources in support of their answers than others. This argument suggests how important such transparency can be.
Find the full conversation here, https://publicera.kb.se/ir/article/view/52258, in Sundin O, Theorising notions of searching, (re)sources and evaluation in the light of generative AI, Information Research 2025, vol 30.
As emergency clinicians, we frequently encounter patients from diverse cultural and religious backgrounds, including a growing Muslim population. This guide outlines key pharmacological considerations when caring for Muslim patients, focusing on the presence of alcohol and porcine-derived gelatin in commonly prescribed medications, two ingredients that may conflict with Islamic beliefs. Drawing from real cases and institutional data at Jefferson Health, the authors highlight how such conflicts can lead to medication refusal, delays in care, and decreased adherence.
The article presents a practical and EM-friendly framework for identifying potentially problematic ingredients using tools like the FDA’s National Drug Code (NDC) and the DailyMed database. It also offers substitution strategies and highlights that alternatives often exist, such as switching from suspensions to tablets or selecting alcohol-free formulations. Importantly, the authors explore the Islamic principles of necessity (darura) and transformation (istihalah), which allow for flexibility in life-saving situations. By integrating cultural awareness into our prescribing habits and leveraging simple EHR strategies, such as tagging “pork” as an allergy to trigger alerts, we can provide more inclusive, respectful, and effective care in the ED without adding significant burden to clinical workflows.
Shout out to UMEM alum Diane Kuhn, MD, PhD as the first author of this recent publication…
She and her colleagues examined the factors that contribute to ED patient experience scores, uncovering several which are not considered in the current CMS evaluative framework. See the editor's (our very own Stephen Schenkel, MD, MPP) capsule summary below:
What is already known on this topic? Medicare plans nationally standardized Emergency Department (ED) Patient Experience scores (ED
CAHPS) to allow comparison across sites.
What question this study addressed. Are there clinical and operational ED characteristics for which ED patient experience scores ought to be adjusted?
What this study adds to our knowledge. Based on 58,622 ED visits from one system, patients arriving in pain were less satisfied and those receiving radiologic studies had a positive experience.
How this is relevant to clinical practice. Influences on patient satisfaction are multifactorial and many are outside the control of the ED. Comparing EDs based on patient experience is complex and prone to misinterpretation.
As the authors point out, If patients placed in a hallway bed have a more negative experience simply due to the location in the department, or patients arriving in pain have a more negative experience regardless of ED care, then some EDs will face more challenges than others in achieving optimal patient experiences.
The current CMS evaluative framework may inherently disadvantage certain EDs, including those with limited physical space relative to their patient volumes, such as safety-net hospitals, or those that care for a high proportion of patients experiencing chronic pain. Is this fair? Does it reflect what CMS is trying to evaluate? Are there alternatives?
Kudos to Dr. Kuhn on her insightful publication and Dr. Schenkel for his expert editing!
Malpractice Insurance comes in two varieties: Occurrence and Claims-made.
Occurrence covers lawsuits for which the event occurs while the insurance is active.
Claims-made only covers lawsuits for which the insurance is active both during the event and when the lawsuit is announced. It’s less expensive because the coverage period is both shorter and more definitive.
This is an important distinction when an event and a lawsuit may be separated by years, as happens with medical malpractice.
Occurrence is the “good” kind.
Claims-made requires a tail to cover any claims brought after the insured period ends.
Read how this can go awry in Emergency Medicine at Leon Adelman’s April post here, https://substack.com/home/post/p-161044772.
Despite ongoing attacks against the principles of DEI, most medical organizations know and have acknowledged the necessary role of creating a more diverse, equitable and inclusive environment. Doing so requires both a bottom up and a top down approach, with engaged leadership supporting active efforts to increase diversity
This author, published just this month in Annals, details a unique and exciting way to engage resident leadership in the DEI efforts of an emergency department, with the creation of a Chief Resident for DEI role. They detail the creation of the role, and describe some of the roles and responsibilities and thoughfully discuss some of the limitations. It's an exciting and thought provoking read.
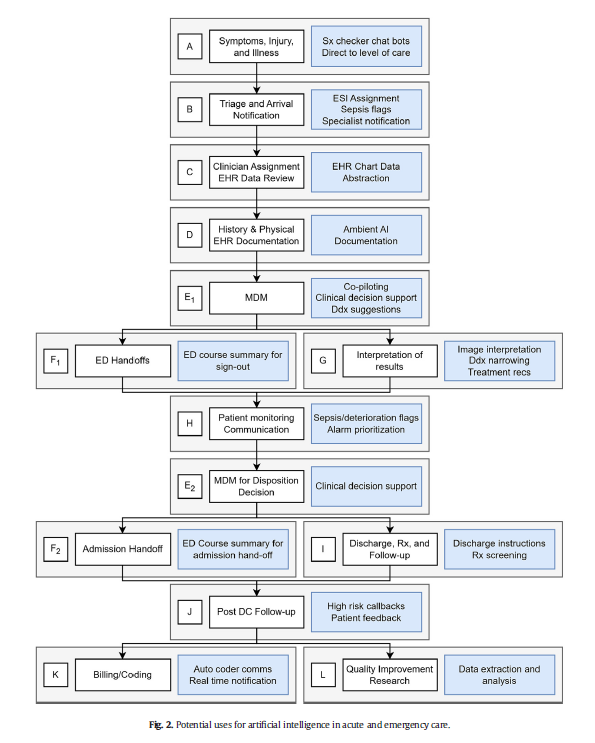
AI is probably already being used in your ED, like it or not…
This article is an excellent review of the ways that AI can be used in emergency medicine. (See blue boxes in the figure below for a visual representation of opportunities for AI to augment emergency care from start to finish.) The authors note that there will always be a role for human physicians in EDs; AI can serve as an adjunct rather than a replacement for physician care. Physicians should strive to be informed leaders in AI development to ensure it is performed in a cautious, thoughtful, patient-centered manner.
We talk a lot about the efforts within our profession at increasing diversity, inclusion and equity, but this study grants a unique perspective on that by surveying our patients on their experience of DEI in the ED.
The authors surveyed about 1700 patients, with 800 responding, at a large ED in Detroit. The population was majority black, and had a wide degree of variability in socioeconomic status.
Overall the patients felt that the staff had no biased or prejudiced interactions with people of different races. However, they felt that people from lower socioeconomic levels, transgender patients, and those that had mental health issues were treated unfairly. They also noted (about17% of respondents) harassment of ED staff by another patient.
You may have seen the headline.
93 million CT examinations conducted on 62 million US patients in 2023 projected to lead to 103000 new cancer diagnoses accounting for 5% of new cancers.
The details of the modeling can be found here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2832778.
What does this have to do with administration?
The solutions rely on administrative involvement:
There’s an editorial here, https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2832782 and a commentary with interviews that put the findings nicely in context here https://arstechnica.com/health/2025/04/ct-scans-could-cause-5-of-cancers-study-finds-experts-note-uncertainty/ (including pointing out that lifetime risk of cancer in the US is 40% and the increase from CT scanning on the order of 0.1% / scan).
This study was the first look at the author's experiences with racial disparities in head and neck trauma in children. It looked at community EDs, and found that white children were more likely to be diagnosed with concussion compared to black children. White children were more likely to be seen as a result of sports or motor vehicle accidents, while black children were more likely to be seen as a result of an assault.
This study revealed the need for further research into the cause of the disparities in care that they identified.
A recent cohort study performed by the NCAA and US Department of Defense looked at NCAA athletes and military cadets who had suffered a concussion.
The study included 1661 NCAA athletes and military cadets, mean age was about 18 years, and 45% were women.
In these groupings, 813 people took over-the-counter pain relievers after their concussion and 848 people did not take any pain relievers.
Analgesics used included medications such as acetaminophen or NSAIDs such as ibuprofen.
Acetaminophen (n = 600), NSAIDs (n = 75), and those taking both (n = 78).
1) 50% recovery
Better teamwork creates better outcomes in emergency medicine. This study investigated how communication practices between physicians and nurses in the ED influence team dynamics and the sense of belonging to the healthcare team.
Methods: 38 emergency physicians and emergency nurses from EDs within a single metropolitan area participated in focus groups.
Positive Influences on Team Belonging:
Negative Influences on Team Belonging:
The findings emphasize the importance of fostering positive communication practices to enhance team dynamics, cohesiveness, and overall well-being within ED healthcare teams.
Ramadan is the holy month in the Islam faith, where observers will fast from sunrise to sunset. This includes food, water, some medications, smoking and sex. This can obviously have some impact on patients' health, especially when presenting to the ED. Here are some considerations to keep in mind:
As with everything, maintaining cultural awareness and compassion will help to
Nurse Practitioners and Physician Assistants practice alongside Physicians in Emergency Departments. In 2021, an estimated 17,679 NPs and PAs worked in EDs.
How long do NPs and PAs continue in Emergency Medicine practice?
An analysis of Medicare data reports that over the eight years of the study, the annual attrition rate averaged 13.8%, or almost 1 in 7 leaving Emergency Medicine practice every year. At the time of attrition, the median age for women was 40.2 years (IQR 33.8 to 49.9) and for men was 45.9 (IQR 37.8 to 56.3).
For additional breakdown and discussion of these numbers, see Gettel CJ, Chosh R, Rothenberg, et al. Workforce Attrition Among Emergency Medicine Non-Physician Practitioners. Ann Emerg Med, in press, https://www.annemergmed.com/article/S0196-0644(24)01294-0/fulltext.
On March 18, 2022, Congress passed the Dr. Lorna Breen Health Care Provider Protection Act, named after an emergency medicine physician who died by suicide during the pandemic. This landmark legislation allocated $103 million across 45 organizations to introduce evidence-based measures to mitigate and prevent burnout.
As a result, the Impact Wellbeing Guide was developed, outlining the six key evidence-based action steps for organization leaders to address health care workers’ professional well-being listed below:
The Guide is designed to help hospital leaders and executives accelerate or supplement professional wellbeing work in their hospitals at the operational level.
A PDF of the full guide is available from the CDC: https://www.cdc.gov/niosh/docs/2024-109/
Clinical practice in the world of the Electronic Medical Record has made many a clinician question the value of electronic reminders.
Banners warn of sepsis, the need for repeat evaluation, vital signs outside expected limits, wait times, and risks for readmission.
Can they instead help ED flow?
Sayan Dutta and colleagues suggest that they can. When clinicians chose to receive notice of a lab or imaging result, push notification reduced time between final result and ED disposition by 18 minutes (95% CI: 15-21 minutes).
The likely key here? Clinicians actively chose when and about what to be notified.
See: Result Push Notifications Improve Time to Emergency Department Disposition: A Pragmatic Observational Study, Annals of Emergency Medicine, 85(1), 53-62. https://www.annemergmed.com/article/S0196-0644(24)00404-9/abstract.
From all of us at UMEM, Happy Thanksgiving!!
We are incredibly Thankful for each of you and all that you do to care for patients and their families.
We are Thankful for those legends who have blazed the path in EM like Greg Henry who the EM community lost yesterday. Our thoughts are with his family. Thank you Dr. Henry for inspiring so many of us. Our pearls today are two of his famous quotes:
“Medicine is show business for ugly people.”
“You don’t go to Disney and see Mickey taking a smoke break. You have to be on when you are on shift”
Gooble, gooble,… gulp, some food for thought on the eve of Thanksgiving.
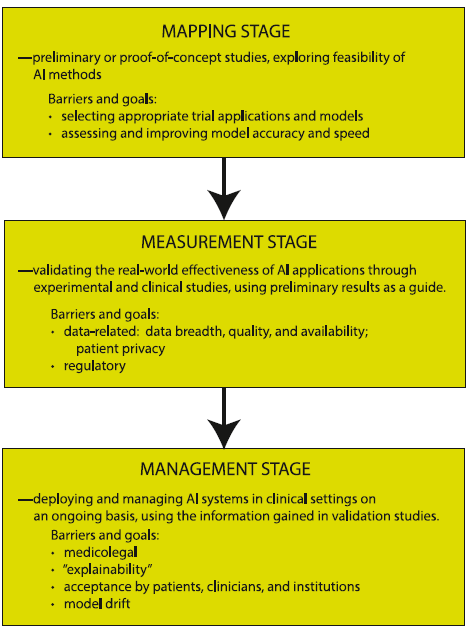
The development of artificial intelligence (AI) in emergency medicine is well under way. The schematic below and accompanying reference presents the anticipated stages in the process of AI development, including important features, considerations, and challenges as we move towards increased integration of AI in our practice of EM.
Does physician altruism influence quality metrics? This study suggests yes.
45 physicians were defined as “altruistic” based on their willingness to share a $250 cash prize with a stranger in an on-line version of the dictator game, something you might have played in an economics class.
Of 250 physicians drawn from primary care and cardiology, 45 met the definition of altruistic and 205 did not.
Overall, patients of altruistic physicians:
The authors suggest that this difference may be on account of altruistic physicians being more willing to consider the appropriateness of tests or treatment or “devote more time and energy to their patients.”
They also note that while most physicians were categorized as not altruistic, at 18% this group of physicians exceeds the 5% of the general US population that would meet this definition.
Perhaps there is something quantitatively demonstrable to being a “good” doctor.
See https://jamanetwork.com/journals/jama-health-forum/fullarticle/2824419