https://the.emergencyphysio.com/wp-content/uploads/knee-lip-lateral.png
What do you see?
There is no clear fracture line
Much like ice floats on water, fat also floats on water/blood because it is less dense.
An intra-articular fracture may allow for blood and fat to exit the bone marrow and settle in the joint space.
This is called a lipohemarthrosis.
Best seen with a cross-table horizontal lateral view x-ray.
Go back to the image and examine the supra patellar pouch.
Most commonly seen in the knee in presence of a tibial plateau fracture.
Seen in approximately 1/3rd of tibial plateau fractures
If you see this without a clear fracture, consider CT of knee which can help detect the hidden fracture.
Remember the DDx of knee hemarthrosis with negative plain films:
Meniscal tear, ligament tear (usually ACL), patellar dislocation and osteochondral fracture.
Except for meniscal tearing (>6h) these other pathologies cause rapid onset swelling (<2h).
Haglund’s deformity
Calcaneal bony growth at the Achilles insertion
Also known as a “pump bump”
Risks: Tight & rigid shoes. Shoes with a hard heel counter. High arches. Tight Achilles tendon. Repetitive heel stress (jumping). Genetically prone bone structures.
Most common in woman between the ages of 15 and 35. Wearing heels. Runners.
Hx: Heel pain and tenderness with a noticeable bump at back of heel. Worse with walking and with certain footwear.
PE: Swelling and redness around bony prominence.
Pain and tenderness in the posterior heel, especially when pressure is applied.
Imaging: Excessive traction and abnormal biomechanics lead to insertional calcifications and bone spurs.
Over time, an exostosis may develop at posterior superior calcaneus as shown in the attached film.

Tx: Physical therapy and orthotics that alter heel height in shoe.
Surgery for chronic cases.
NSAIDs are first line analgesic medications for many pain related ED presentations
All NSAIDs are not created equal in their side effect profile
Ibuprofen and ketorolac are both commonly used NSAIDs in the ED
A 2010 review looked at relative risk estimates of individual NSAIDs and associated upper GI bleeding/perforation.
Definitions: Most of included studies included patients with NSAID use within prior week and daignosed upper GI bleed admitted to the hospital.
Daily use predicted increased risk.
In comparison between these two common medications Ibuprofen and Ketorolac: RR as follows
Ibuprofen (2.69 [95% CI 2.17-3.33]) vs ketorolac (14.54 [95% CI 5.87-36.04])
Ketorolac has approximately double the half life of ibuprofen
Other commonly used ED medications were also included:
RRs:
Naproxen 5.63 (95% CI 3.83-8.28)
Indomethacin 5.40 (95% CI 4.16-7.00)
Meloxicam 4.15 (95% CI 2.59-6.64)
Diclofenac 3.98 (95% CI 3.36-4.72)
Conclusion: The risk of upper GI bleeding varies between individual NSAIDs at the doses commonly used in the general population. When possible, consider the relative risk of a particular NSAID when making a selection.
Distal Radius Fractures
One of the most common fracture locations seen in EM (1/6th of all fractures)
Surgical rates are approximately 15-20%
Bimodal injury distribution:
Younger patients (10-14yo)
Usually involved in sport and usually high energy mechanism
Sport associated injury: Artificial turf increase risk by 5x.
Increased risk with skiing and rugby
Increased risk with novice and intermediate snowboarders who don’t wear protective equipment.
Older patients (>50yo)
Associated with osteoporotic bone from low energy fall
Risk factors among older patients: Hx of recurrent falls, prior fragility fracture, decreased bone density, corticosteroid use, and also dementia when patient reaches age 75.
Encourage your older patients who sustain this injury to discuss bone density testing with their PCP. Patients at higher risk of hip fractures (which carries high morbidity and mortality)
Check and document median nerve function in all patients esp. in high energy injuries
Median nerve involved in up to 21-30%.
Check “A-OK sign” against resistance
Iatrogenic median nerve injury can also occur if patient splinted in position of flexion
Metformin, most widely used for type 2 diabetes, has shown promising early results in several different health outcomes.
A recent study, published in JAMA, investigated whether metformin could reduce knee pain in patients with symptomatic knee OA who were overweight or obese.
This was a small double-blind, placebo-controlled clinical trial involving 107 participants.
Background: There is some evidence (both preclinical and preliminary human) that metformin can reduce cartilage degradation and increase chondrocyte viability.
Intervention: Participants received metformin 2000 mg/day (n=54), or identical placebo (n=53) for 6 months.
Mean age, 58.8 [SD, 9.5] years. 68% female.
Patients had symptomatic radiologic knee OA and a body mass index > 25.
Adverse effects: Diarrhea (8 [15%] in the metformin group and 4 [8%] in the placebo group) and abdominal discomfort (7 [13%] in the metformin group and 5 [9%] in the placebo group).
Despite this, there were high levels of medication adherence.
The study found significant differences in primary and secondary outcome measures: Knee pain, stiffness and function.
There was some weight loss in both groups (mean change, 4 lbs in the metformin group and 2.6 lbs in the placebo group). Unlikely to explain outcome differences.
Conclusion: In patients with symptomatic knee osteoarthritis who were overweight or obese, metformin, had a moderate and statistically significant reduction in knee pain compared with placebo. Because of the small sample size, confirmation in a larger clinical trial is warranted.
This article reminds us that hip fractures have a one year mortality rate of 12-25% and 50% of hip fracture patients develop complications while in the hospital. “Almost half of individuals hospitalized with hip fractures experience complications, such as delirium, pneumonia, acute kidney injury, urinary tract infection, and deep vein thrombosis”
Because of these complications, multidisciplinary teams should be caring for these patients and great care should be exercised when evaluating these patients.
Non benzodiazepine muscle relaxants
Muscle relaxants were the most commonly (32%) prescribed medication upon discharge from the ED for lower back pain.
Muscle relaxants, such as cyclobenzaprine, provide short term pain-relief for patients with acute low back pain compared to placebo.
There is little difference in efficacy among the various muscle relaxants.
Evidence for muscle relaxants for back pain is weak compared to NSAIDs, so limit use to patients who have contraindications to NSAIDS.
There is no strong evidence that combination therapy with NSAIDs is more effective than NSAIDs alone.
If using during the day, consider using a lower dose (cyclobenzaprine 5mg) and a higher dose at night (10mg).
If treating with NSAIDs, consider using only at night to promote sleep.
Also, limit use to those patients who can tolerate the side effect profile of muscle relaxants, which include anticholinergic effects, dizziness, and sedation.
Risks of these agents increase with age, so should be used with caution in older adults.
Often given to this population due to fears of NSAID side effects.
Lidocaine transdermal patches
Frequently used for lower back pain.
A single 5% patch contains 700mg of lidocaine.
There is low systemic absorption.
Data supporting efficacy for lower back pain are limited.
Best benefit in other neuropathic conditions such as post herpetic neuralgia.
Topical capsicum
Underused, safe, non-sedating.
Potential treatment option for acute and subacute back pain (<3 months duration).
Can be OTC or via prescription.
Available in cream, lotion and patches.
Best used 3-4 times per day for maximal effectiveness.
Grade A recommendation from North American Spine Society.
A previous pearl discussed Spondylolysis. Once clinical concern is sufficient, the question of appropriate imaging arises.
Traditionally, the addition of oblique radiographs was recommended because they showed the pathognomonic “Scotty dog” sign. Recent studies have shown there is no significant increase in diagnosing spondylolysis with the addition of these oblique views. These additional views carry added cost and radiation exposure (approximately double).
AP and lateral radiographs offer similar diagnostic sensitivity to the old four view series.
If plain films are negative and symptoms persist despite 2-3 weeks of rest from offending activities, advanced imaging can be pursued on an outpatient basis. This is also strongly considered if the patient wishes to return to sport.
Despite being primarily osseous pathology, studies have shown that MRI can have similar diagnostic sensitivity to CT particularly in cases of acute injury. MRI may also show signs of stress reaction before complete fracture occurs.
Communicate with radiology and MRI technicians that you are looking for spondylolysis as this may affect the MRI sequences.
If a positive finding occurs on plain film, ordering CT imaging for the entire lumbar spine should be deferred due to added radiation concerns especially in cases where MRI would be available.
If MRI is not practical, consider limiting CT to one level above and one level below the region of concern. This would decrease the radiation exposure by approximately 50%
If advanced imaging is not practical or available and patient has a positive plain film, consider recommending repeat imaging in 4-6 weeks as an outpatient with rest from all offending activities.
https://buckup-cuh-production.s3.amazonaws.com/images/Capture_IIWc51k.width-840.png
“Hey Doc, do I knee surgery?”
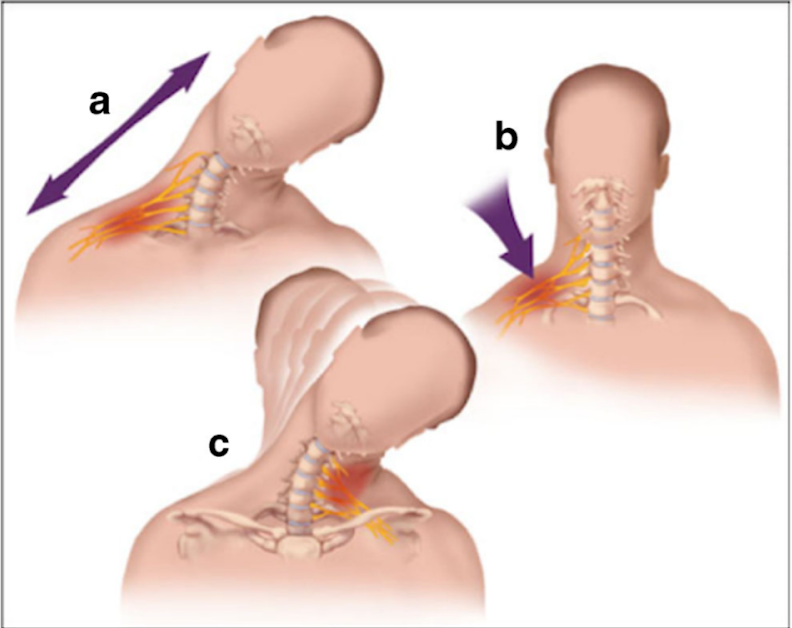
A stinger is a short lived neuropraxia to the upper brachial plexus
Named for the temporary sensation that radiates from the shoulder to the hand
Can occur though 3 common mechanisms
Most commonly from direct traumatic or tractional injury
https://www.physio-network.com/wp-content/uploads/2021/11/unnamed-1.png
Common in American Football
Occurs in almost 50% of players over a 4-year college career
Most commonly to running backs and linebackers in one NFL study
Symptoms: Unilateral burning pain and tingling in the arm with transient weakness
Symptoms NOT confined to a single dermatome.
Usually in C5, C6 innervated muscles (deltoid and biceps).
Symptoms are transient usually resolving in approximately 2 minutes
If asked to examine someone for this at a sporting event
Evaluate patient for:
C spine tenderness
Full cervical range of motion
UNILATERAL weakness in shoulder Abductors and external rotators
UNILATERAL weakness in biceps
UNILATERAL weakness in forearm pronation
UNILATERAL weakness in triceps extension
Consider evaluation for concussion symptoms if appropriate
Majority of patients in college and profession sports return to play in game when exam returns to normal
Ankle sprains are frequently lateral.
They occur less frequently to the medial or “high” ankle.
High ankle sprains without fracture occur in 5-6% of ankle injuries presenting to the ED
Rates of injury are much higher in college and professional hockey and football players
The tibiofibular syndesmosis is primarily injured in high ankle sprains
Mechanism: Typically, external rotation or eversion on a dorsiflexed ankle
Example: When a player’s leg is forcefully rotated while foot is planted
Hx: anterior lateral ankle pain. Frequently significant pain with weight bearing.
PE: local tenderness over the syndesmosis ligaments
Two specialized tests may aid in the diagnosis
https://wikism.org/Squeeze_Test#/media/File:Squeeze_test_example.jpg
2. Dorsiflexion-external rotation test – This test attempts to reproduce the forces commonly involved in the original injury. Positive test is reproduction of pain. Position patient similar to above test. Grasp the upper calf with one hand while the other hand grasps the midfoot and places the foot in dorsiflexion and external rotation.
https://www.dralexjimenez.com/wp-content/uploads/2017/07/external-rotation-test-1.png
Trigger finger/thumb
Occurs from mechanical impingement
-Stenosing tenosynovitis
Much more common in patients with diabetes
Causes clicking, catching, locking and pain
Occurs at the A1 pulley
Flexor tendon “catches” as it attempts to glide through a stenotic flexor tendon sheath
Initially, patient's report painless catching or locking of the affected digit during flexion
During finger flexion and extension, pain is caused by inflamed tendon passing through a relatively constricted tendon sheath
Occurs most often in the ring and middle digits
May improve over the course of the day
Diagnoses with active triggering (with digit flexion and extension) and tenderness to palpation at the first annular pulley (A1) which overlies the first MCP joint
-Ask patient to place hand on table face up and gradually fully flex and extend the fingers
May note a palpable nodule of the flexor tendon
Treatment: Activity modification, NSAIDs and splinting (3-6 weeks)
Corticosteroid injection is very effective
https://www.ahta.com.au/client_images/2553101.png
Olecranon bursitis
Superficial synovial membrane located overlying the proximal ulna/olecranon allows for easy irritation and inflammation
Swelling does not involve the joint
Most common bursitis (approx. 4x more common than prepatellar)
Male>>Female
Prone to trauma, inflammation or infection
-RA, gout, overlying break in skin
Chronic inflammation results from excessive leaning on the elbow such as with certain occupations (plumber, military recruit)
Inflammation may be septic or aseptic
Usual cause is traumatic
Approximately 20% of acute cases may have a septic origin
Classically appears as a “goose egg” area on posterior elbow
Well-demarcated and fluctuant
Small amount of swelling and/or those with minimal symptoms should be left alone and treated with activity modification, NSAIDS, ice. Suggest an elbow pad for protection.
If this does not resolve symptoms after approximately 4 weeks, consider referral for aspiration and steroid injection
If aspiration is ED performed for evaluation of possible septic bursitis, recommend a compressive elbow sleeve to help prevent reaccumulating
If a recurrent issue for patient and aspirated, consider a posterior elbow splint for approx. 10 days and refer to orthopedics.
Shoulder Abduction Test aka Bakody’s Sign
Used clinically in the evaluation of patients with suspected cervical radiculopathy
Unlike Spurling’s test, where we create discomfort, this test attempts to relieve it.
Specifically, evaluates for nerve root compression at C4-C6/7
To perform:
Arm Abduction can be active or passive
3. Instruct the patient to hold this position for 30 seconds.
4.Observe the patient for any relief of symptoms (A positive test)
Decrease in pain, numbness, weakness or tingling
5. Repeat on the unaffected side for comparison.
Sensitivity: 17–78% Specificity: 75–92%
Note: when asked about what alleviates their pain, patients will frequently describe and demonstrate the maneuver.
Consider adding this simple maneuver in your assessment of patients with suspected symptomatic cervical radiculopathy
A northeast university was recently in the news when several members of the lacrosse team were hospitalized with rhabdomyolysis. 9 of 50 players who participated in the workout required hospitalization. This occurred after a single intense 45-minute workout led by an alum and recent graduate of the Navy Seal training program.
It was surprising to many that young, fit, athletes would be so affected from a single workout.
Nontraumatic exertional rhabdomyolysis occurs following intense physical activity especially in untrained individuals or those unaccustomed to the particular activity (for example a group of runners performing an intense HIIT workout).
Prolonged strenuous activity can result in rhabdomyolysis even in trained individuals in the absence of known risk factors or prior history.
Increased risk when natural cooling mechanisms are affected such as when the individual is taking medications with anticholinergic properties, or the individual is wearing heavy military gear or football equipment.
Increased risk with sickle cell trait.
Increased risk when that activity is performed in environments of severe heat and humidity.
Exercise routines that have a heavy eccentric focus increases risk of rhabdomyolysis.
An Eccentric exercise involves slow lengthening of muscles under load
Examples: the lowering phase of a barbell while performing a bench press or the downward phase of a pull up
Helpful kinetics:
Following the exertional event, the serum CK will rise within 2-12 hours, reaching its maximum in 1-3 days.
CK has a serum half-life of approximately 36 hours.
CK levels decrease at approximately 40% per day.
When it comes to walking, recent research and public health strategies have focused on how much you do that helps. This idea frequently comes up in the form of the 10,000 step goal.
A recent study in the British Journal of Sports Medicine found that walking between 9,000 and 10,000 steps/day could reduce the risk of death by 39% and cardiovascular disease by 21%.
For both outcomes (all-cause mortality and incident CVD), approximately 50% of the benefit was achieved between 4,000-4,500 steps per day.
Study accessed data on greater than 72,000 individuals (avg age 61, 58% female) using accelerometer data over an average of 6.9 years.
Instead of volume, a recent study in the same journal looked at the benefits of walking speed.
The study looked at pooled data from 10 studies involving more than 500,000 people from the U.S., Japan and the U.K.
Walking speed definitions:
Easy or casual walking - less than 2 mph.
Average or normal pace was defined as 2-3mph.
A “fairly brisk” pace was 3-4 mph
A “brisk/striding walking pace” was greater than 4mph
Compared with people who walked at a casual/easy speed, those who walked at a normal/avg speed (2–3 mph) had a 15% lower risk of Type 2 diabetes.
Walking at a fairly brisk pace (3–4 mph) was associated with a 24% lower risk of Type 2 diabetes.
Walking at a brisk or striding pace (over 4 mph) was associated with a 39% reduced risk of Type 2 diabetes.
Globally, 537 million adults have type 2 diabetes, a figure that is expected to reach 783 million by 2045.
Take home: Consider recommending tips on walking pace and distance for our sedentary patient population to optimize health.
The Lever test can be used to examine for a torn ACL
May be helpful when examining larger patients
Place patient supine with both knees extended. Examiner places fist below the proximal third of patient’s calf.
With the other hand, the examiner presses down on the distal third of the patient’s quadriceps.
Positive test: A torn ACL disrupts the lever arm of the lower leg. The heel will not rise.
Negative test: An intact ACL allows the lever arm of the lower leg to lift the heel. The heel will rise.
More study is needed but reported sensitivities are similar to classic tests such as the anterior drawer or Lachman.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}