Heat stroke is hyperthermia (>41.6 Celsius / 106 Fahrenheit) plus neurologic findings (e.g., altered mental status, seizures, coma, etc.); it also causes systemic inflammation response syndrome (i.e., cytokine release), coagulation disorders (e.g., thrombosis in end organs) and tissue abnormalities (e.g., acute kidney injury and rhabdomyolysis)
Two classifications exist:
Treatment includes:
Despite the most aggressive therapy, up to 30% survivors may have permanent neurologic or multi-organ system dysfunction months to years after recovery
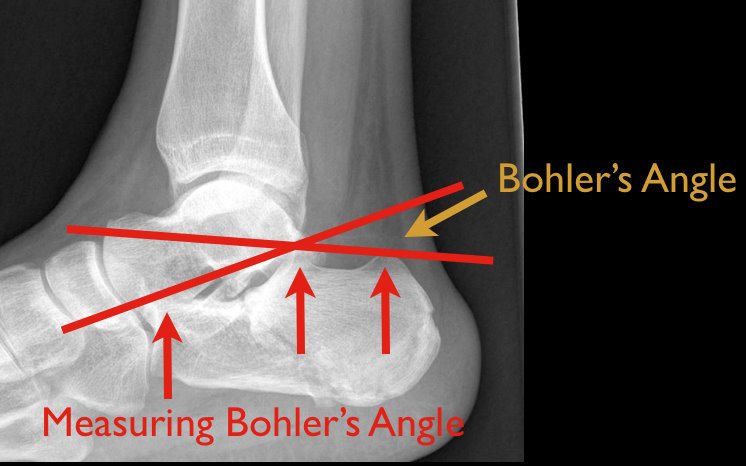
48 year old male following 15 foot fall onto both feet. What is the diagnosis?
…and why is it called the “Lover’s Fracture”?

Amiodarone is a class III anti-arrhythmic for tachyarrhythmias
Although most patients remain euthyroid on amiodarone, 4-18% develop thyroid disease months to years after exposure.
Amiodarone-induced thyroid disease occurs because amiodarone is structurally similar to triiodothyronine and thyroxine and each 200mg tablet contains 75 mg of iodine.
Two types of amiodarone-induced thyroid disease:
Amiodarone-induced hypothyroidism (AIH)
Amiodarone-induced thyrotoxicosis (AIT)
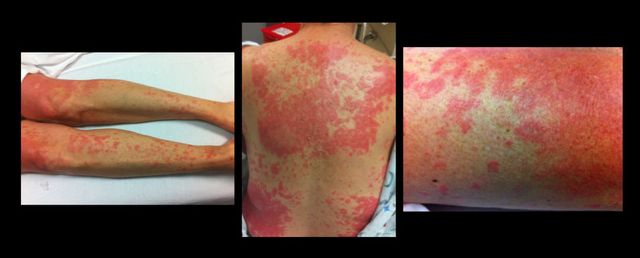
49 y.o. female on Trimethoprim/sulfamethoxazole presents with rash and oral mucus membrane lesions. Diagnosis?
Cancer patients admitted to ICUs with AKI or who develop AKI during their ICU stay have increased risk of morbidity and mortality. AKI in cancer patients is typically multi-factorial:
Causes indirectly related to malignancy
Septic, cardiogenic, or hypovolemic shock (most common)
Nephrotoxins:
Aminoglycosides
Contrast-induced nephropathy
Chemotherapy
Hemolytic-Uremic Syndrome
Causes directly related to malignancy
Tumor-lysis syndrome
Disseminated Intravascular Coagulation
Obstruction of urinary tract by malignancy
Multiple Myeloma of the kidney
Hypercalcemia
Because AKI increases the already elevated morbidity and mortality in these patients, prevention (e.g., using low-osmolar IV contrast, avoiding nephrotoxins), early identification (e.g., strict attention to urine output and renal function), and aggressive treatment (e.g., early initiation of renal replacement therapy) is essential.
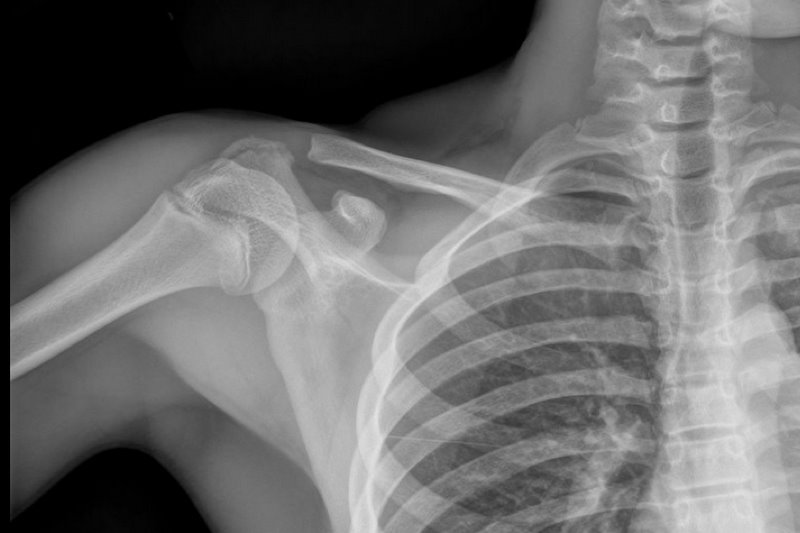
13 y.o. with shoulder trauma (during basketball game). Arm held in adduction and exquisite scapular tenderness. Diagnosis?
Bleeding associated with uremia is a spectrum, from mild cases (e.g., bruising or prolonged bleeding from venipuncture) to life-threatening (e.g., GI or intracranial bleed). The exact pathologic mechanisms are not understood, but are likely multi-factorial (e.g., dysfunctional von Willebrand’s Factor (vWF) and factor VIII, increased NO, etc.)
Besides dialysis, treatments for uremic bleeding include:
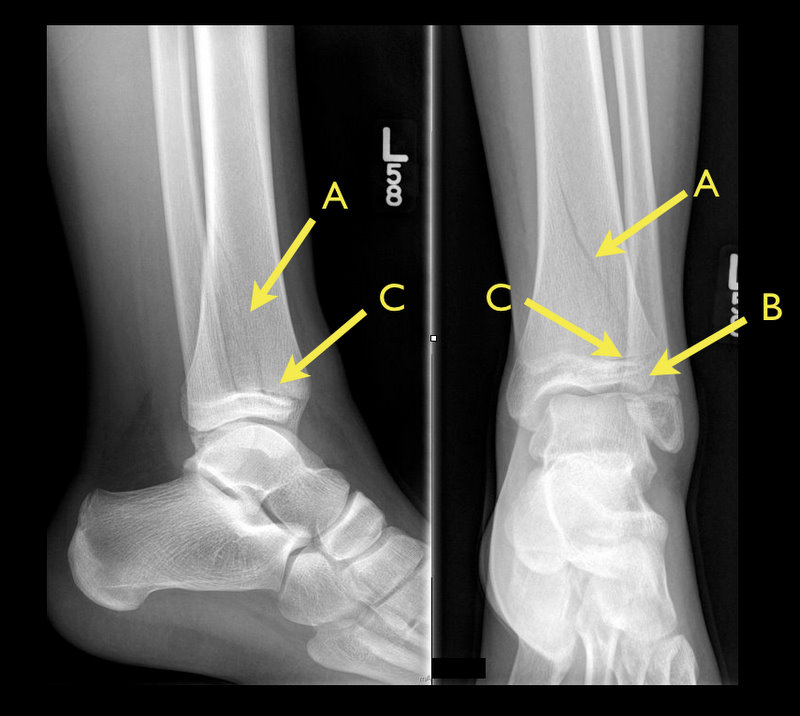
13 y.o. female with ankle pain following fall down escalator. What's the diagnosis? (Hint: Look very closely)

TIP: Suspect when abdominal pain presents 10-14 after chemotherapy (when PMNs are lowest).

Although oral metronidazole is indicated for mild to moderate Clostridium difficile associated diarrhea, oral vancomycin should be considered first-line therapy in critically-ill patients with moderate to severe disease. Vancomycin dosing should begin at 125mg PO q6 and increased to 250mg q6 if poor enteral absorption exists. Consider adding metronidazole IV if either reduced enteral absorption or severe disease exists.
Recently, fidaxomicin has been shown to be non-inferior to oral vancomycin in the treatment of mild to moderate C. difficile. While promising, the study population was not critically-ill and extrapolation should be avoided.
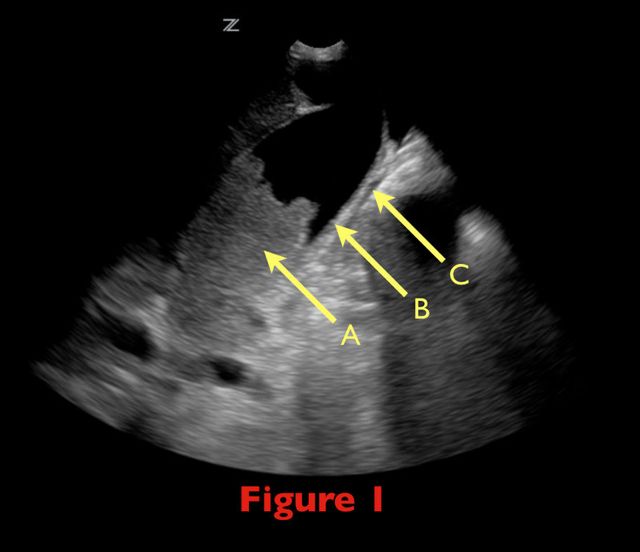
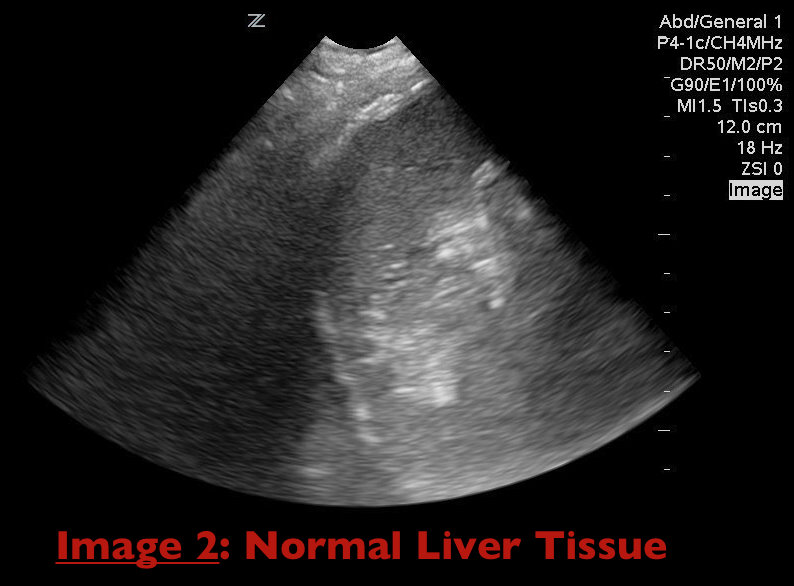
70 yo female from nursing home with fever. RUQ ultrasound is shown below. Diagnosis?

A mortality benefit from combination antimicrobial therapy has not been clearly demonstrated in sepsis. However, when only the most severely-ill patients (i.e., septic shock) are considered in subgroup analysis, there appears to be a mortality benefit to using two antimicrobials against a suspected organism.
Combination antimicrobial therapy may reduce mortality through three mechanisms.
Always obtain appropriate cultures before initiating therapy. Although identification and susceptibility of the organism may take some time, eventually narrowing antimicrobial therapy to monotherapy in the ICU is still recommended.
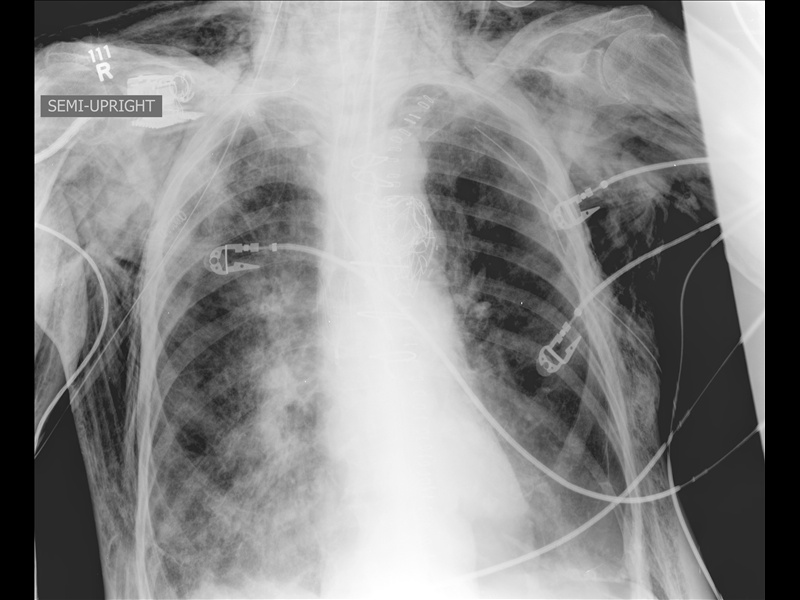
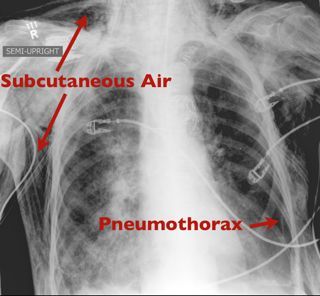
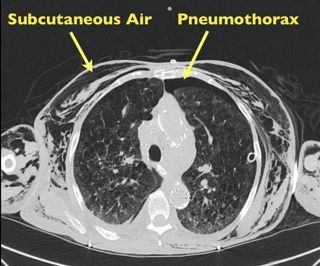
Patient presents with the following X ray after yawning. Diagnosis?

Vancomycin is often started empirically for gram-positive and MRSA coverage. Although effective and generally well-tolerated, emerging resistance and side-effect profiles limit its use in some patients. Two alternatives are Linezolid and Daptomycin.
Linezolid
Daptomycin
60 y/o male transferred from local rehab facility c/o abdominal pain.

Emergency Medicine physicians are gaining experience with non-invasive ventilation (i.e., Bi-level ventilation and continuous positive-pressure ventilation) in managing respiratory distress and failure. Although NIV is commonly used across a variety of pathologies, the best data exists for use with COPD exacerbation and cardiogenic pulmonary edema (CHF, not an acute MI)
Although other indications for NIV have been studied, the data is less robust (eg., smaller study size, weak control groups, etc.). If there are no contraindications, however, many experts still support a trial of NIV in the following populations:
Failure to clinically improve during a NIV trial should prompt invasive mechanical ventilation.
25 year old male presents after falling from 10 feet and landing on right shoulder. Diagnosis?

Many changes in pulmonary physiology occur during pregnancy. These changes are generally well tolerated but can become problematic when pathologic states arise.
Here are a few examples of the normal changes and potential consequences:
Progesterone increases tidal volume and respiratory rate.
“Normally" a mild respiratory alkalosis pH 7.4-7.47, PaCO2 28-32, and bicarbonate 17-22 (renal compensation).
Low metabolic reserve with systemic illness.
Weight gain, anasarca, and breast size reduces chest wall elasticity.
Potential for restrictive physiology and reduced lung volumes.
Can be challenging to to mechanically ventilate due to decreased compliance and intra-thoracic pressure
Mechanical displacement of abdominal and thoracic contents by growing uterus.
Reduced lung volumes leading to reduced oxygen reserve and decreased apnea time.
Aim higher if placing chest tube (avoid abdominal contents)
Uterine pressure on stomach can increase aspiration risk and pulmonary injury.
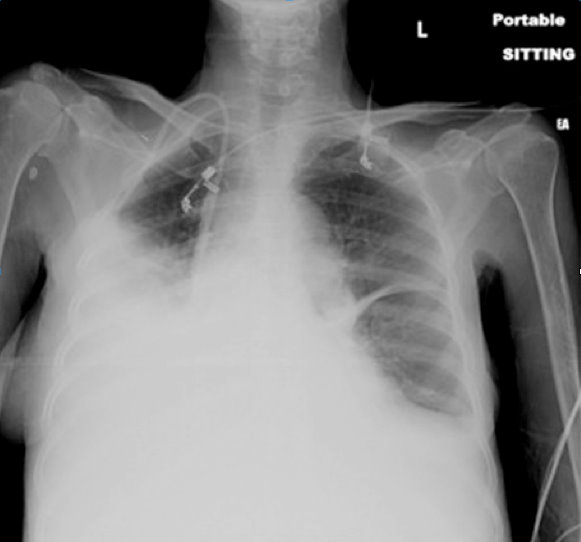
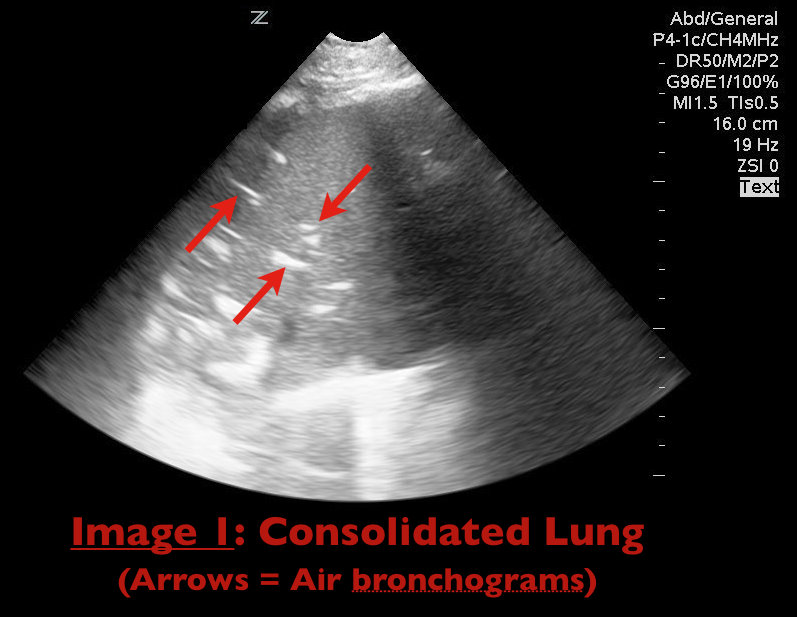
65 yo female with breast cancer presents with dyspnea and CXR shown below. Diagnosis? Can anything help clarify the diagnosis?