Vision loss whether acute or chronic is a common presenting complaint to the ED. This will be the first in a series of pearls on the subject. This pearl will address the nomenclature used by ophthalmology based on the length of vision loss.
• Transient visual obscuration - Episodes lasting seconds. Usually associated with papilledema and increased intracranial pressure.
• Amaurosis fugax - Brief, fleeting attack of monocular partial or total blindness that lasts seconds to minutes
• Transient monocular visual loss or transient monocular blindness - A more persistent vision loss that lasts minutes or longer
• Transient bilateral visual loss - Episodes affecting one or both eyes or both cerebral hemispheres and causing visual loss
• Ocular infarction - Persistent ischemic damage to the eye, resulting in permanent vision loss
MEWDS (Multiple Evanescent White Dot Syndrome)
Scaphoid Fractures in Children:
Because of the high (30%) fracture rate seen on followup films it is recommended that all children be placed into a thumb spica splint until followed up.
Slipped Capital Femoral Epiphysis (SCFE)
SCFE can present as hip, thigh or knee pain in the young adolescent. Risk factors include hypogonadism, hypothyroidism, hypopituiratism, and obesity. One way to make the diagnosis is to obtain a AP view of the pelvis and draw a line(Klein's line) along the superior border of the neck of the femur. This line should intersect the femoral epiphysis. If it does not the diagnosis of SCFE can be made.
However, this is only about 40% sensitivity. Green et al recently published a study that demonstrated that if you measure the distance from Klein's line and the lateral edge of the femoral epiphysis on both sides, and the difference between the two is more than 2mm you can make the diagnosis of SCFE more accurately and sooner.

FIGURE 1. Measurement methods on an anterior-posterior radiograph of a right slipped capital femoral epiphysis. White lines indicate Klein’s line for each hip. A and B, indicate maximum epiphyseal width lateral to Klein’s line. As A is 2mm narrower than B, the right (A) hip qualifies as a slip using our modification but not Klein’s original definition.
Wound Irrigation
A recent article by Thomas et al showed that any concentration of betadiene and hydrogen peroxide used to irrigate a wound was more toxic to fibroblasts (required for wound healing) then it was to bacteria. Low concentrations of chlorhexidine remained bactericidial while having minimal affects on fibroblasts.
WIth the addition of this study the routine practice of soaking a wound in betadiene or hydrogen peroxide should be abandoned. Good irrigation with normal saline or even tap water is all that is really needed to decontaminiate a wound. If a bactericidal agent is needed then low concentrations of chlorhexidine should be used.
Snuff Box Tenderness:
It has become the standard of care that individuals with snuff box tenderness, or pain with axial loading of the thumb, be placed in a thumb spica splint for 1-2 weeks until follow up x-rays can be done. This is done to rule out an occult scaphoid fracture. However, this practice can be hugely inconvenient to the patient and result in some atrophy of their forearm.
An alternative approach is to obtain a CT scan through the wrist to look specifically at the scaphoid bone. If the CT scan is negative you can send them home with some pain control, RICE (Rest, Ice, Compression, Elevation) treatment and let them use thier thumb. No splint is needed. If it is positive then you can splint them and have them follow up with orthopedics or hand surgery.
Reimburshment Pearls:
Often charts are down coded as it is not clear from the documentation that your medical decision making was complex.
For instance, if your final diagnosis is GERD, and you do not document that you were also concerned about angina or a pneumothorax your level 5 chart could be coded as a level 3, since the final diganosis does not seem that complex. In order to prevent this document:
I realize that when you are busy this might be the last thing on your mind, but the difference between a level III chart and a level V chart is about $100, and the only additional work is the 3 minutes it would take to document what you did for the patient.
More to come...
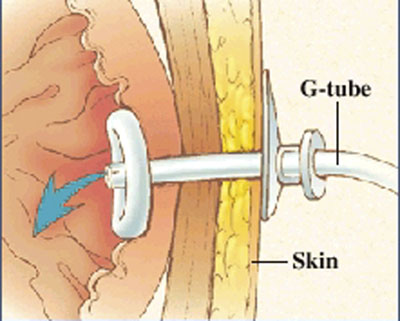
I am sure everybody has received a patient from a nursing home that had a malfunctioning PEG tube. Now if they would only crush the tablets before putting them down the tube, or better yet use liquid medications our life would be easier.
But what do you do if it is Friday and the GI lab is not open to Monday. The answer is that you can remove the PEG and replace it with another PEG tube or even a foley catheter will do for the weekend. The original PEG tube has a semi-rigid plastic ring (as shown in photo) and does not have a balloon that can be default. You can pull these out by placing counter traction on the abdominal wall and pulling with steady firm pressure. This may take a little more force than you are initially comfortable with.
Please see the attached photo of a PEG tube, and remember the other option is to admit these patients for IV fluids until the GI lab opens.
AC Joint Dislocations
The acromioclavicular (AC) Joint is commonly injured when a person falls onto their shoulder.
The AC Joint consists of three ligaments:
Injuries to this joint are classified as Type I – Type VI and involve sprain or tears of the AC or CC ligaments
Medical Treatment of Hyperparathyroidism
Hyperparathyroidism results in elevated PTH and typically results in elevated calcium levels (hypercalcemia).
Though most cases are asymptomatic, symptomatic patients can present with:
Treatment options to be discussed next week....Stay tuned.
Rhogam Dosing:
Though most textbooks recommend Micro-Rhogram (50mcg) for woman that have miscarried and are less than 12 weeks gestation, you might find it a real challenge to get that dose from your pharmacy or blood bank.
The cost difference between microRhogram and Rhogam is minimal so most hospitals have decided to only stock full dose (300 mcg) Rhogam. The full dose can be given to woman in their 1st trimester without any deleterious effects.
Just remember if you are giving it as a result of a delivery you should order a Kleihauer-Betke test to determine if additional doses of Rhogam are needed.
Apathetic Hypothyroidism AKA Hypothyroidism in the Elderly
Remember that elderly do not present with classic signs and symptoms of hypothyroidism, but rather it is more common for them to have atypical presentations.
Things that make the diagnosis more difficult in the elderly are:
Consider the diagnosis in elderly patients with:
Cushing Syndrome
The most common cause of Cushing syndrome is the use of exogenous glucocorticoids, and it is rarer to have a problem with the hypothalamic-pituitary-adrenal axis.
These patients can present with:
For the emergency department we need to be worried about those on chronic steroids that can not increase their native steroid production in a time of stress which will lead them to adrenal crisis.
Pearls for those with Cushing Syndrome:
Monteggia's Fracture
Postpartum Headaches:
NG Tubes and Foleys:
Dovetailing off Dr. Hayes Lidocaine pearl on Thursday I thought we could provide an additional pearl on how to decrease pain with the insertion of Foleys and NG tubes.
Most providers use regular surgilube and coat the tip of the NG tube and foley with it prior to inserting it. Unfortunately this tends to only lubricate the first several centimeters of the passage you are trying to transverse, making the rest of the way a little uncomfortable.
Using a Uroget of viscious lidocaine allows you to actually inject the lubricant into the nares or urethral meatus. This will provide better lubrication of the entire passage and also provide some anesthesia.
Even if you do not want to use lidocaine most foley kits come with a syringe full of surgilube that can be injected into the urethral meatus helping to lubricate the passage.
Blast Injuries:
In honor of the 4th of July holiday, here is a quick pearl about blast injuries.
Metacarpal Fractures and Growth Plates:
The growth plates on metacarpals are on the distal end of the bone, except for the 1st metacarpal which is on the proximal end near the carpal bones.
Don't mistake this for a fracture line, however, make sure you get comparison views if they are tender over the area, as this can help you diagnosis a Salter Harris Type 1 fracture.
High Pressure Injection Injuries: