Carpal Tunnel Syndrome (CTS):
All to often we see children that are sent to the ED for "Pink Eye" as the school nurse will not allow them back into class unless they are treated with antibiotics. A recent study out of New York identified 4 factors that are associated with low risk (<8% chance) of bacterial (culture postive) conjunctivitis. They are:
An editorial in journal watch comments that if this study can be replicated in other geographic areas we could change the practice of prescribing antibiotics that are not necessary.
Prosthetic hip dislocations are a common occurance in the Emergency Department. After you have gotten the hip back in place there are several ways to prevent the hip from coming out again. An abductor pillow will work but it confines the patient to bed. A better option to prevent further hip dislocations until the patient can get an appropriate brace made or reparative surgery is to place the patient in a straight leg knee immoblizer. It is nearly impossible to dislocate your hip if your knee is fully extended.
So after reduction of their simple hip dislocation (i.e: no fractures) place the patient in a straight leg knee immobolizer and they can followup with their orthopedist as an outpatient.
Review of the Appearance of Ossification Centers in Children's Elbows
Determing if a child's elbow has a fracture or if you are looking at an ossification center is easier if you remember the mnemonic CRITOE. This is the order that the ossification centers appear:
Critical Care billing is time dependent and includes all time spent caring for and coordinating (i.e.: reviewing records, talking to consultants or family) the care of the patient except for the time spent doing separately billable procedures (i.e. central line, CPR, etc). The following procedures taken from the ACEP website are included in the Critical Care code so the time spent doing these procedures should BE included in your total Critical Care time .
They are :
ACADEMIC MEDICINE CAVEAT: For the reporting of time-based services, such as critical care or moderate sedation, the teaching physician must be directly present during the entire reported time period.
Knee Dislocation:
Pelligrini-Stieda Lesion:
A Pelligrini-Stieda lesion is shown in the radiograph below. This lesion was originally described in 1905, and is associated with a tear of the Medial Collateral Ligament. Heterotrophic calcification forms causing chronic pain, which typically needs to be surgically excised.
So for the students out there, it is possible to diagnosis an MCL tear on plain radiographs. Just not very often.

The Segond Fracture:
An benign appearing avulsion fracture of the lateral tibeal plateau that is marker for more significant injuries such as:
If this avulsion fracture is seen consider immobilzing the patients knee until they can follow up with Orthopedics and/or get an MRI to determine if additional injuries are present.

A recent study by Smith et al showed that the general abdomen/pelvic CT scan in trauma patients obtained with 5mm slices is a better screening test for spine fractures than plain films. They also showed that when compared to dedicated reconstructed thoracolumbar CT scan (2mm slices focused on the spine) it did not miss any clinically significant fractures.
The statistic for plain radiographs and the nonreconstructive CT scan are shown below.
| | Plain Radiographs | Nonreconstructive CT Scan | ||
| | Lumbar | Thoracic | Lumbar | Thoracic |
| Sensitivity % [95% CI] | 47 [33 to 62] | 13 [3 to 32] | 94 [83 to 99] | 73 [50 to 89] |
| Specificity % [95% CI] | 91 [78 to 97] | 71 [54 to 85] | 95 [85 to 99] | 94 [79 to 99] |
| Positive Predictive Value % [95% CI] | 85 [66 to 96] | 15 [2 to 45] | 95 [86 to 99] | 89 [67 to 99] |
| Negative Predictive Value % [95% CI] | 61 [48 to 72] | 56 [41 to 71] | 93 [82 to 99] | 83 [66 to 93] |
The take home point is that dedicated Spine CT scans are probably not needed unless they are going to be used to guide surgical or non-surgical management, and plain films should probably be abandoned in patients that are undergoing CT scans of the chest/abdomen/pelvis.
Impingement Syndrome and the Diagnostic Accuracy of 5 Common Tests
It is also reported that subacromial impingement syndrome (SAIS) is the more frequent cause of shoulder pain.
The authors of this study attempted to determine the diagnostic accuracy of the following 5 tests for SAIS:
The study demonstrated that any 3 positive tests out of the 5 has a sensitivity of 0.75 (0.54-0.96) , specificity of 0.74 (0.61-0.88), positive likelihood ratio of 2.93 (1.60-5.36) and negative likelihood ratio of 0.34 (0.14-0.80). See the table below for the individual test characteristics. No single test was deemed accurate enough to make the diagnosis by itself.
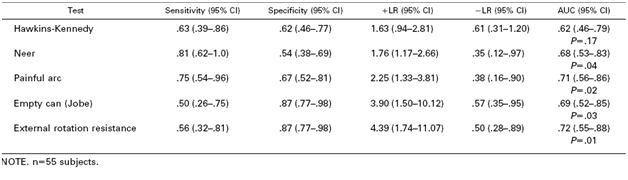
So in the end you should be familiar with most of these tests in order to use a combination of them to make the diagnosis of impingement syndrome. Future pearls will review how to perform these tests.
Scaphoid Fractures:
For suspected scaphoid fractures with negative radiographs it is common practice to put a person in a short arm thumb spica splint until followup up radiographs can be obtained in 10-14 days.
However, there is evidence that a short arm thumb spica splint is not enough for people that have a true scaphoid fracture. Gellman et al demonstrated that long arm thumb-spica cast immobilization for six weeks followed by short arm thumb-spica cast immobilization decreased time to union by 25% when compared to short arm thumb-spica casting alone.
The theory is that the short arm splint still allows for forearm rotation that can cause shearing motion of the volar radiocarpal ligaments. A long arm splint prevents this shearing action. The disadvantage of a long arm splint though is potential elbow joint stiffness and muscle atrophy that can occur during the prolonged period of immobilization.
So for your next patient with a scaphoid fracture seen on radiographs place them in a long arm thumb spica splint.
Temporal Arteritis (TA) is commonly associated with the sudden onset of a unilateral headache centered around the temporal region. The most devastating consequence of TA is blindness though this is only reported in up to 50% of cases though can be bilateral in up to 33% of patients.
According to the American College of Rheumatology criteria for classification of temporal arteritis this diagnosis can be made in the ED without a biopsy. You just need at least 3 of the following 5 items to be present (sensitivity 93.5%, specificity 91.2%) to make the diagnosis :
Uveitis and Iritis Treatment:
Iritis is a common diagnosis in the ED, but did you know it was actually a subset of Uveitis.
Uveitis is an inflammation of one or all parts of the uveal tract which consists of the iris, the ciliary body, and the choroid.
The subsets of uveitis are:
Treatment of iritis and uveitis next week.
Acute paronychia
Pityriasis Rosea
Nikolsky's sign is positive when slight rubbing of the skin results in exfoliation of the skin's outermost layer. The more technical term is acantholysis which is the loss of the normal adhesion of the epithelial skin cells which allows for this sloughing.
Seen in:
Often helpful to differentiate pemphigus vulgaris from bullous pemphigoid. The sign is usually absent in bullous pemphigoid. Just be careful with how much testing you are doing as this can be very painful to the patient.
Hypothermia Pearls:
Finally, remember to monitor the patient closely when you first start rewarming as this can induce cardiac arrest. This is thought to occur as colder peripherial blood returns to the central circulation as peripherial veins and arteries dilated from the warm fluid.
Patella fractures are typically due to direct trauma as in a fall or direct blow to the knee.
Fractures may be missed on the AP view or misdiagnosed as a bipartate fracture. To avoid these pitfalls look closely at the lateral view and consider getting a sunrise view of the knee (better visualizes the patella). Finally, unilateral bipartate patella are very rare so consider an x-ray of the contralateral knee if you are considering this as your diagnosis.
Surgery should be considered for:
Some of the causes of acute vision loss are: