Category: Orthopedics
Keywords: Shoulder, biceps, tendon (PubMed Search)
Posted: 11/28/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
A 25 year old athlete presents to the ED with right anterior shoulder pain.
Pain radiates into proximal biceps.
It is worse with heavy lifting and especially “pulling” exercises at the gym.
How do we evaluate for biceps tendonitis?
Pathology is often the long head of the biceps
https://physioworks.com.au/wp-content/uploads/2019/12/biceps-tendonitis.jpg
Start by palpating this area and attempt to reproduce the discomfort
Speed’s test
Yergason’s test
Category: Orthopedics
Keywords: Elbow, dislocation, instability (PubMed Search)
Posted: 10/25/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Ulnar Collateral ligament injuries of the elbow
Overhead throwing athletes are at risk of insufficiency and rupture of the ulnar collateral ligament (UCL) of the elbow
This can lead to valgus instability similar to what can occur in the knee
Overhead throwing places a significant valgus stress on the elbow
Though classically seen in baseball pitchers, may also be seen in javelin throwers and other high velocity throwing sports
In the acute setting may be seen after an elbow dislocation
History includes a “pop” and medial elbow pain following throwing activities
In cases of overuse injury, athletes will report a progressive loss of velocity, accuracy, and/or endurance with throwing.
The ulnar collateral ligament is the primary restraint to valgus stress from 30 to 120 degrees of flexion
One classic test for UCL instability is the milking maneuver
Patient may be sitting or standing
Patient’s forearm is supinated and elbow flexed at 90 degrees
A valgus force is applied by pulling the patient’s thumb while the examiner’s other hand stabilizes the elbow and palpates the medial joint line.
Instability, pain or apprehension at the UCL is considered a positive test
https://www.youtube.com/watch?v=gbn24X_qqn0
Category: Orthopedics
Keywords: Carpal Tunnel Syndrome, neuropathy (PubMed Search)
Posted: 10/10/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Carpal Tunnel Syndrome (CTS)
The hallmark of classic CTS: pain or paresthesia (numbness and tingling) in a distribution that includes the median nerve territory, with involvement of the first three digits and the radial half of the fourth digit.
The symptoms of CTS are typically worse at night and often awaken patients from sleep.
Fixed sensory loss is usually a late finding
Involves the median-innervated fingers BUT spares the thenar eminence.
This pattern occurs because the palmar sensory cutaneous nerve arises proximal to the wrist and passes over, rather than through, the carpal tunnel.
Consider a more proximal lesion in cases involving sensory loss in the thenar eminence
Example: pronator syndrome
Category: Orthopedics
Keywords: Elder abuse, bruising, trauma (PubMed Search)
Posted: 9/26/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Physical injury patterns associated with physical elder abuse
Elder abuse is both common and underrecognized
Between 5 and 10% of US older adults are victims of elder abuse annually
For many older adults, contact with a health care provider may represent their only contact outside the home
Differentiating physical elder abuse from unintentional trauma can be very difficult
A recent study compared these two groups with a case-control design
Study cases: 100 successfully prosecuted physical elder abuse cases from a single urban ED
Physical abuse victims were more likely to have:
Bruising (78% vs. 54%)
Injuries to maxillofacial, dental or neck region (67% vs. 28%)
Particularly the LEFT side
Neck injuries 6x more common is assault
Ear injuries occurred in assault but not in falls
Absence of fracture (8% vs. 22%)
Less likely to have lower extremity injuries (9% vs. 41%)
22% of victims had no visible injuries
Most common mechanism assault with hands or fists and pushing or shoving causing a fall
Take home: Consider elder abuse especially in cases of the above red flags
Rosen T, et al. Identifying Injury Patterns Associated With Physical Elder Abuse: Analysis of Legally Adjudicated Cases. Ann Emerg Med. 2020 Sep;76(3):266-276.
Category: Orthopedics
Keywords: Spine fracture, decision rule (PubMed Search)
Posted: 9/12/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
A recent study looked at thoracic spinal fractures in the era of the trauma panscan
NEXUS Chest CT Study from 2011 to 2014 at 9 Level I trauma centers.
Goal: To describe the identification rate and types of thoracic spine fractures.
Inclusion: age over 14 years, blunt trauma occurring within 6 hours of ED presentation, and chest CT imaging during ED evaluation.
11,477 subjects, 217 (1.9%) had a thoracic spine fracture
The majority of spine fractures in patients who had both chest x-ray and CT were observed on CT only (91%). 50% had more than 1 thoracic spinal level involved (mean 2.1). 22% had associated cervical fractures and 25% had associated lumbar fractures.
64% had vertebral body fractures
45% had posterior column fractures
28% had compression fractures
6% had burst fractures
Many patients (62%) had associated thoracic injuries such as
Rib fractures (45%)
PTX (36%)
Clavicle fracture (18%)
Scapular fracture (17%)
Hemothorax (15%)
100 patients had clinically significant thoracic spine fractures.
Thoracic spine fractures are relatively uncommon in adult patients with blunt trauma.
If thoracic spine fracture is suspected clinically, radiography is not an effective screen and clinician should consider CT. If not suspected, guidelines discourage ordering CT to screen for this injury because of effective screening instruments, the diagnosis of clinically insignificant injuries and radiation exposure.
All clinically significant thoracic spine fractures would have been detected by the NEXUS Chest CT decision instrument.
https://www.mdcalc.com/nexus-chest-ct-decision-instrument-ct-imaging
Bizimungu R, Sergio Alvarez, Baumann BM, et al. Thoracic Spine Fracture in the Panscan Era. Ann Emerg Med. 2020;76(2):143-148.
Category: Orthopedics
Keywords: Elbow, fracture, ultrasound (PubMed Search)
Posted: 8/12/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Diagnostic performance of Ultrasonography for detection of pediatric elbow fracture
Elbow fractures account for approximately 15% of pediatric fractures
Fat pads are traditionally taught as a marker of fracture
In a cadaveric study:
Elbow effusions of 1-3 mL could be identified with ultrasound
Elbow effusions of 5-10 mL could be identified with plain film
Pediatric plain films are sometimes challenging to obtain and interpret compared to adults
-More likely to be uncooperative in obtaining required views
-Non-ossified epiphyses
Ultrasound may be used to detect
-Cortical disruption and irregularity
-Growth plate widening
-Hematoma interposed between fracture fragments
-Elevated posterior fat pad
Absence of elbow fracture was indicated by
-Lack of cortical disruption
-Absence of posterior fat pad sign
Meta-analysis of 10 articles totaling 519 patients using ultrasonography to detect elbow fractures
Sensitivity 96%
Specificity 89%
False negative rate 3.7%
For comparison, plain radiographs
Interpreted by peds EM physicians (87.5% sensitive and 100% specific)
Interpreted by radiology (96% sensitive, 100% specific)
Consider using ultrasound as a noninvasive, radiation-free modality for accurate diagnosis of pediatric elbow fractures.
Lee SH, Yun SJ. Diagnostic Performance of Ultrasonography for Detection of Pediatric Elbow Fracture: A Meta-analysis. Ann Emerg Med. 2019;74(4):493-502.
Category: Orthopedics
Keywords: Peripheral neuropathy, median nerve (PubMed Search)
Posted: 8/8/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Pronator Teres Syndrome
A compressive neuropathy of the median nerve in the region of the elbow
The median nerve passes through the cubital fossa and passes between the superficial and deep heads of the pronator teres muscle.
Rare compared to other compressive neuropathies such as carpal tunnel syndrome.
More common in women and in fifth decade of life
May be seen with weight lifters, arm wrestlers, rowers, tennis, archery, professional cyclists, dentists, fiddlers, pianists, harpists
Also associated with well-developed forearm muscles
History:
Forearm pain – unlike carpal tunnel
Paresthesias in median distribution
No night symptoms – unlike carpal tunnel
Physical exam:
Sensory loss in medial nerve distribution.
Involves the thenar eminence!
Unlike carpal tunnel syndrome which doesn’t involve sensory loss in thenar eminence.
Pain may be made worse with resisted forearm pronation
Compression/Tinel’s sign over pronator mass reproduces symptoms
Treatment:
Splinting which limits pronation and NSAIDs
Steroid injection
Surgical nerve decompression is non operative treatment fails after greater than 6 months (rare)
Category: Orthopedics
Keywords: carpal tunnel syndrome, neuropathy, (PubMed Search)
Posted: 7/11/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Treatment for carpal tunnel syndrome (CTS)
The management of CTS depends of the severity of the disease
If symptoms or on the mild to moderate range, a trial of conservative treatment is encouraged.
Possible therapeutic approaches can include splinting in wrist neutral position. Some even extend to keep the CMP joints extended. Extreme flexion and extension can increase pressure within the carpal tunnel. Usually for nighttime use only. May be used during day based on work and activity demands.
Has been shown to improve electrophysiologic findings after 12 weeks of use in moderate CTS.
Formal hand physical therapy (by an experienced therapist) may also be of some benefit including carpal bone mobilization, ultrasound and nerve glide exercises.
There is small evidence for the benefit of prednisone (20mg/d) as it has been shown to be more effective than placebo with improvements lasting an average of 8 weeks.
There is no benefit to NSAIDs or diuretics.
There is poor evidence for therapeutic ultrasound and acupuncture.
While more invasive than the above modalities, steroid injections may decrease inflammation and pressure in the carpal tunnel. Patients randomized to steroid injection may do better than those randomized to nighttime splinting.
Early referral in those with positive electrodiagnostic findings is encouraged as they do best with earlier surgical release and have better recovery.
If however the patient has severe, progressive or persistent symptoms or there is known evidence of nerve injury on diagnostic testing, referral for surgical decompression is warranted.
Category: Orthopedics
Keywords: Sickle cell trait, exertional death (PubMed Search)
Posted: 6/13/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Sickle cell trait (SCT) is common and often overlooked clinically
-7.3% African Americans
-0.7% Hispanics
-0.3% Caucasians
SCT is a leading cause of exertional death in athletes who play football
The exact mechanism is unknown but likely involves a combination of high intensity exercise, dehydration, heat strain and inadequate opportunity for cardiovascular recovery leading to microvascular erythrocyte sickling.
This leads to hypoxia, cell death, hyperkalemia, and death from arrhythmia.
Presentation often involves rhabdomyolysis and exertional collapse.
In August of 2010 the NCAA enacted legislation requiring documentation of SCT status of all Division 1 athletes (2012 for Division 2 and 2014 for Division 3)
They also mandated education, counseling and issued guidelines for proper conditioning
Sudden death in athletes with SCT was first observed in military recruits in 1970.
Death in African American military recruits was 28 times more likely in those with SCT than in those without.
A 2012 study of football athletes found the risk of exertional death to be 37 times higher in athletes with SCT than in those without.
Despite game/competition situations being more intense, deaths occur almost exclusively during practice and conditioning drills.
Following the 2010 legislation, there has been a 89% decrease in death from SCT in NCAA D1 football.
Workout plans need to account for heat/humidity, the athletes level of conditioning and allow for adequate rest, recovery, hydration. SCT screening is only part of the solution.
Buchanan et al., 2020. Sudden Death Associated With Sickle Cell Trait Before and After Mandatory Screening. Sports Health.
Category: Orthopedics
Keywords: Concussion, musculoskeletal, injury, lower extremity (PubMed Search)
Posted: 5/23/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Post concussion musculoskeletal injuries
Sport related concussion (SRC) impairs numerous functions of the CNS.
Traditional research has focused on risk of repeat concussion following clearance and return to sport
Several studies have shown a consistent elevated risk of lower extremity injuries from 90 days up to one year following SRC.
These include lateral ankle sprains and ACL injuries. Risk ranges, 1.3-3.4x.
This risk may be greater in those with multiple concussions.
This elevated rate has been seen in populations ranging from high school, college to professional athletes and has also been seen in the general population.
Persistent neurological deficits in cognitive and postural control, stability and gait deviations have been postulated as potential mechanisms.
These may be potential modifiable risk factors before return to play/activity. This may be a role best served by sport physical therapists to assist with sport specific rehabilitation post concussion.
Category: Orthopedics
Keywords: mTBI, concussion, MRI (PubMed Search)
Posted: 5/9/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
MRI for Concussion Testing in the ED
The increased sensitivity of MRI may have a role in detecting more subtle intracranial injuries.
135 patients with mild TBI were prospectively evaluated for acute head injury in emergency departments of 3 LEVEL I trauma.
27% of these patients with a normal initial head CT had an abnormal brain MRI including contusions and microhemorrhages. A greater number of these subtle findings was associated with neuropsychological defects on both short-term memory function and with poorer 3 month cognitive outcomes. Inherent difficulties of access, actionable results and reimbursement issues prevent application of MRI for concussion evaluation in the ED.
Note: Mild TBI defined as GCS 13-15 is not the same as sport or activity related concussion which I consider to be GCS 14-15.
Take home: There is currently no role for MRI in the acute evaluation of concussion in the ED.
1) Yuh et al., 2013. Magnetic resonance imaging improves 3-month outcome prediction in mild traumatic brain injury. Ann Neurol.
2) Huang et al., 2015. Susceptibility weighted MRI in mild traumatic brain injury. Neurology.
Category: Orthopedics
Keywords: ibuprofen, analgesia, pain (PubMed Search)
Posted: 4/25/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Comparison of Oral Ibuprofen at Three Single-dose Regimens for Treating Acute Pain in the Emergency Department: A Randomized Controlled Trial
Ibuprofen is one of the most commonly used medications in the ED for the acute treatment of pain. Analgesic ceiling doses are not well supported. Some adverse effects of NSAIDs are dose dependent (GI and cardiovascular).
A recent study looked to compare the analgesic effect of oral ibuprofen at 3 different doses
Population: Adult ED patients (aged 18 and older) with acute pain.
Methods: Randomized double-blind trial.
Goal: To examine the efficacy of ibuprofen at 400, 600 and 800mg.
Only 225 patients enrolled (75 per group). Outcome was difference in pain scores at 60 minutes.
Results: Difference in mean pain scores at 60 minutes between 400 and 600mg (0.14), 400 and 800mg (0.14) and 600 and 800mg (0.00).
Conclusion: Reduction in pain scores was similar between all 3 dosing groups. Consider lower dosing of ibuprofen in ED patients presenting with acute pain.
This analgesic ceiling dose is lower than recommended by the FDA and most EM textbooks.
Consider using the 400mg ibuprofen dose for ED patients with acute pain
Motov et al., 2019. Comparison of Oral Ibuprofen at Three Single-dose Regimens for Treating Acute Pain in the Emergency Department: A Randomized Controlled Trial. Annals of Emergency Medicine. Oct 2019.
Category: Orthopedics
Keywords: Analgesia, muscle injury, pain control (PubMed Search)
Posted: 3/28/2020 by Brian Corwell, MD
(Updated: 4/11/2020)
Click here to contact Brian Corwell, MD
A recent study looked at
Back pain is the most common pain complaint worldwide
-Accounted for about 9% of all ED visits.
Summary: ED use of tramadol for back pain doubled from 2007 to 2016 despite an overall decrease in opioid use (in that period)
Tramadol -- either administered in the ED or prescribed -- was used in 8.4% of back pain visits in 2016, up from 4.1% in 2007 (P=0.001).
In 2007, overall opioid use was 53.5%; in 2016, it was 46.5% (P=0.001). The largest drop was in hydrocodone use.
A recent study in JAMA looked at the risk of death in 90,000 people one year after filling a Rx for tramadol vs. one of several other analgesics such as naproxen, diclofenac or codeine.
All patients were aged 50 years or older and has osteoarthritis.
Initial Rx for tramadol was associated with a higher rate of mortality than with NSAIDs (but not compared to codeine).
Zeng et al., 2019. Association of Tramadol With All-Cause Mortality Among Patients With Osteoarthritis. JAMA 2019 March 12;321(10):969-982.
Mullins et al., 2020. Trends in Evaluation and Management of Back Pain in United States Emergency Departments (2007-2016). AAAPM 2020.
Category: Orthopedics
Keywords: Dislocation, fracture (PubMed Search)
Posted: 3/28/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Studying the demographics of all both sports and recreation related injuries is important for the development of effective preventive strategies.
Methods: National electronic injury surveillance system all injury program from 2005 to 2013 (367,300 sports and recreation related ED visits).
18 common sports and recreational activities in the United States
Results: A fracture occurred in 20.6% and a joint dislocation in 3.6% in ED visits for a sport related visit
Most of the fractures occurred in football (22.5%) and occurred in autumn and summer. Most fractures occurred in arm/hand (finger most common). Most fractures occurred in school or sporting venues.
The OR for fracture was greatest for inline skating (6.03), males (1.21) and those between 10 and 14 years of age and those older than 84 years (4.77).
Dislocations were highest in basketball (25.7%) and occurred in the autumn and on weekends. Most dislocations occurred in school or sporting venues.
The OR for dislocation was greatest in gymnastics (4.08), males (1.50) and those aged 20 to 24 years (9.04)
The most common fracture involved the finger and the most common dislocation involved the shoulder, followed by finger and knee.
The Demographics of Fractures and Dislocations Across the Entire United States due to Common Sports and Recreational Activities. Sports Health. 2020 Mar/Apr;12(2):159-169.
Category: Airway Management
Keywords: Epidural abscess, back pain (PubMed Search)
Posted: 3/14/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Laboratory studies are not often indicated in the early evaluation of low back pain.
Complete blood counts (CBC) have poor sensitivity and specificity for infection. White blood cell (WBC) counts, have poor sensitivity and specificity for infection. They may be elevated and a left shift or bandemia may be present and increase suspicion for infection, but a lack of these does not rule out infection. Elevated WBC counts are only found in two-thirds of patients with SEA.
Both erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are highly sensitive (84-100%) for spinal infections and are observed in >80% with vertebral osteomyelitis and epidural abscesses. However, elevated CRP was found in 87% of patients with an epidural abscess as well as half of patients with spine pain not due to an epidural abscess, so is not highly specific.
CRP levels rise rapidly and decrease rapidly with improvement in disease and may be better used to follow response to treatment. ESR is the most sensitive and specific serum marker of infection. ESR is elevated in 94-100% of patients with an epidural abscess compared to only 33% of those without an epidural abscess. Infection is unlikely in patients with an ESR less than 20 mm/h. Although an elevated ESR (>20 mm/h) is the most specific serum test for infection, it also may indicate occult malignancy (sensitivity, 78%; specificity, 67%).
If infection is suspected, obtain two sets of blood cultures, as a causative pathogen may be identified in ~50% of patients.
Category: Airway Management
Keywords: MRI, back pain (PubMed Search)
Posted: 2/22/2020 by Brian Corwell, MD
Click here to contact Brian Corwell, MD
Cauda Equina Syndrome is a medical emergency that is considered in all patients who present to the ED with lower back pain.
Clinical presentation is variable in nature and may include some combination of lower back pain, bowel or bladder dysfunction, sexual dysfunction, saddle anesthesia with motor/sensory abnormalities.
MRI is the gold standard for diagnosis
Many of us have encountered a scenario where a patient with high clinical suspicion returns with scan negative MRI.
Studies have attempted to characterize this population.
Patients in the scan negative group had an increased prevalence of functional disorders (37% vs. 9%), functional neurologic disorders (12% vs. 0%), and psychiatric comorbidities (53% vs. 20%).
Further study is needed to characterize this association.
Hospitals may consider individualized neurologic and psychiatric referral for certain patients who are scan negative in the future.
Is scan-negative cauda equina syndrome a functional neurological disorder? A pilot study. Gibson et al., Eur J Neurol 2020, Feb 19.
Is scan-negative cauda equina syndrome a functional neurological disorder? A pilot study. Gibson et al., Eur J Neurol 2020, Feb 19.
Category: Orthopedics
Keywords: Back pain (PubMed Search)
Posted: 2/8/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Taking an accurate history to diagnose Cauda Equina Syndrome (CES)
Classic teaching is to inquire specifically about bowel and bladder function, sexual dysfunction, and/or loss of sensation in the groin.
Rather than asking about urinary incontinence, clinicians should ask specifically about difficulty passing urine, new leakage and retention.
Discussing issues related to sexual dysfunction are difficult for both clinicians and patients.
Rather than asking if there are any issues with sexual function, a more direct and informative way would be to ask if the patient has a “change in ability to achieve an erection or ejaculate” or “loss of sensation in genitals during sexual intercourse.”
Saddle anesthesia has the highest predictive value in diagnosing MRI-proven CES. Loss of sensation may be incomplete and patchy. Ask about change in sensation with wiping after a bowel movement.
Greenhalgh S, Truman C, Webster V, Selfe J. Development of a toolkit for early identification of cauda equina syndrome. Prim Health Care Res Dev. 2016;17(6):559-567.
Category: Orthopedics
Keywords: Concussion, (PubMed Search)
Posted: 1/25/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Timeliness of Concussion Referral
Do patients with a self-limited diagnosis of “concussion” require specialty follow up?
If so, is there a benefit to earlier evaluation?
Recently published research from the University of Pittsburgh Sports Medicine Concussion Program suggests so.
Subjects: 162 concussed athletes between the ages of 12 and 22
Findings: Athletes treated in the first week after injury recovered faster than those who did not receive care until 8 to 21 days post injury.
Note: Once in care the length of time spent recovering was the same for both groups. This suggests that the amount of time prior to the initiation of care may explain the longer recovery time of the 2nd group.
Earlier recovery can help minimize effects on mood, quality of life and lost time in school/work.
Take home: Consiuder early follow up referral to a qualified provider for all concussed patients seen in the ED
Kontos et al., 2020. Association of Time Since Injury to the First Clinic Visit With Recovery Following Concussion. Jama Neurology.
Kontos et al., 2020. Association of Time Since Injury to the First Clinic Visit With Recovery Following Concussion. Jama Neurology.
Category: Airway Management
Keywords: back pain, urinary retention, CES (PubMed Search)
Posted: 1/11/2020 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
Known effects and side effects of prescribed medicines may masquerade as cauda equina syndrome (CES) .
Analgesic medicines used by patients with chronic back pain may also cloud the diagnosis of CES.
Cholinergic medications (glaucoma/myasthenia) may lead to voiding issues.
Anticholinergic medications (COPD/urinary incontinence) may lead to urinary retention.
Opioids – Constipation, reduced bladder sensation
Anticonvulsants (Gabapentin/Pregabalin)- Urinary incontinence
Antidepressants (Amitriptyline) – Urinary retention, sexual dysfunction, reduced awareness of need to pass urine
NSAIDs – Urinary retention.
Verhamme KM, et al. Nonsteroidal anti-inflammatory drugs and increased risk of acute urinary retention. Arch Intern Med. 2005:165;1547-1551.
Category: Orthopedics
Keywords: Klein's line, S sign, AVN (PubMed Search)
Posted: 12/14/2019 by Brian Corwell, MD
(Updated: 6/28/2026)
Click here to contact Brian Corwell, MD
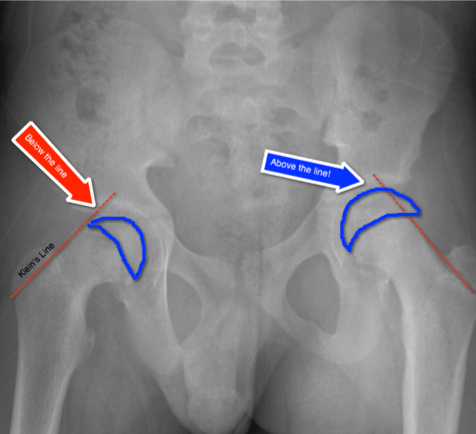
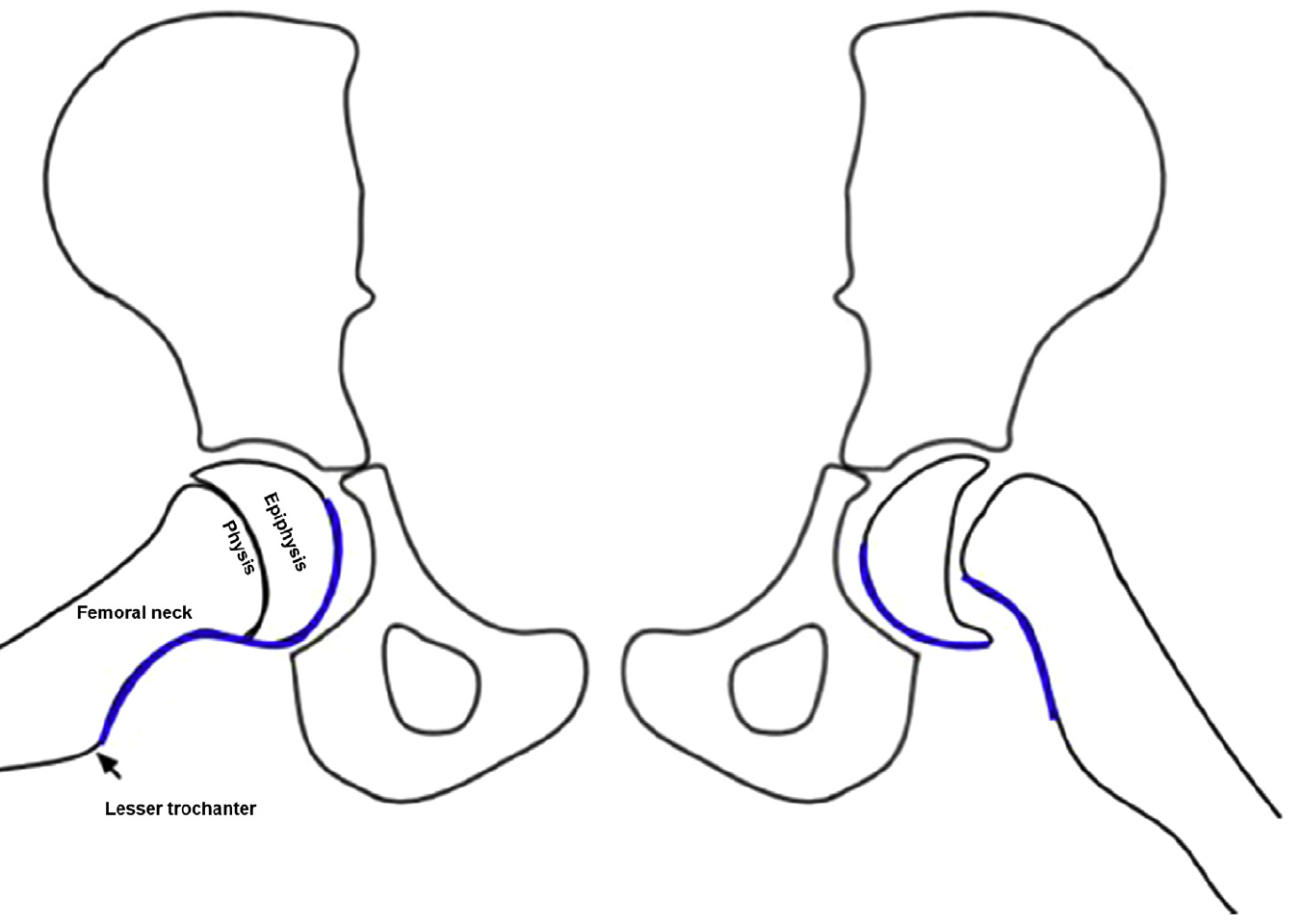
Slipped Capital Femoral Epiphysis (SCFE)
http://www.raymondliumd.com/images/SCFE%20illustrated%20and%20cropped.jpg
Early Diagnosis:
Klein’s Line on AP view
https://pedemmorsels.com/wp-content/uploads/2018/01/Slipped-Capital-Femoral-Epiphysis-3.png
Another virtual line may assist in diagnosis
S-sign
Klein's line and S-sign
Consider adding both of these virtual lines/signs to your review of the pediatric hip plain film
Rebich et al., 2018. The S Sign: A New Radiographic Tool to Aid in the Diagnosis of Slipped Capital Femoral Epiphysis. J Emerg Med.
{kind=link}
{kind=link}
{kind=link}
{kind=link}