Pes Anserinus pain syndrome (formerly pes anserine Bursitis)
Occurs at the bursa of the pes anserinus which overlies the attachment of the 1) Sartorius 2) gracilis and 3) semi-tendinosis tendons. Insertions resemble a Goose’s foot.
An inflammatory condition of the medial knee
Location is 2-3 inches below the knee joint on the medial side
1st layer of medial compartment
https://www.dramynrajani.com/wp-content/uploads/2018/05/pes-anserine-bursitis-clinical-test.jpg
Patients complain of knee pain just below medial joint line (esp with stairs)
History may include sudden increase in running distance especially with hills (common)
Associated with obesity, tight hamstring muscles and with knee OA
PE: Tenderness to palpation of the bursa possibly with mild swelling
DDx: MCL tear, medial meniscus injury, medial (knee) compartment arthritis, tibial stress fracture
Treatment: Cessation/modification of offending activities, Icing and ice massage, NSAIDs, hamstring stretching and physical therapy. Failure of the above should prompt referral for bursal steroid injection.
Exericse as preventative medicine!
A recent cohort study of over 2,000 adults (mean age approx. 45) over approximately 11 years of follow-up investigated the association of step count with mortality.
This study found that those participants taking at least 7,000 steps per day compared to those taking fewer steps had a 50%-70% lower risk of mortality. They did not find an association with step intensity.
Another recent study investigated the dose-response association between daily step count and intensity and the incidence of all-cause dementia.
Uk based study of >78,000 adults aged 40 to 79 years with approximately 7 years of follow-up. Data from wrist accelerometer and registry-based dementia diagnoses.
Optimal step dose was 9826 steps. Minimal dose was 3826 steps (value at which the risk reduction was 50% of the observed max).
In this study, steps performed at higher intensity (112 steps/min) resulted in stronger associations.
Conclusions: A great exercise goal for middle aged and older adults is just under 10,000 steps per day to decrease risks of both overall mortality and dementia.
Limited data are available to guide recommendations re screen time after concussion.
A recent ED study looked at screen time effects on concussion recovery.
Population: 125 patients aged 12 to 25 years presenting to the ED <24h after injury. Mean age 17. Approximately 51% male.
Intervention: Patients were placed in a screen time allowed group and a screen time not allowed group for the first 48 hours. Total minutes reported after the study were 630 minutes vs 130 minutes.
Outcome: Time to symptom resolution. Patients took daily symptom scoring tests for 10 days.
Result: Screen time allowed group had a significantly longer time to recovery (8 days) vs screen time not allowed (3.5 days).
Strength: Good attempt at quantifying effects on early screen time exposure on symptom recovery in an ED population.
Weakness: This was a small study. Many patients (>25%) were lost to follow-up and it relies on symptom self-reporting.
The hip joint is a very strong and stable structure requiring great force to produce a dislocation
Most hip dislocations are posterior (80-90%)
Mechanism: MVC generating force onto an adducted flexed hip (most commonly)
Associated injuries occur both locally (acetabular fx) and distant (knee bone and ligamentous)
Significant associated injuries in >70%
The hip joint has a very precarious blood supply.
One of the risk factors for AVN is total dislocation time
<6 hours - 5% incidence
>6 hours – up to 53% incidence
Examine the sciatic nerve carefully with posterior dislocations (10% incidence)
Motor – EHL/ankle dorsiflexion
Sensory – sensation dorsum of foot
There are many reduction maneuvers including the East Baltimore Lift technique
https://www.youtube.com/watch?v=1zvelGbVn04
Demonstrated at 30 seconds in above video
Place patient supine with affected leg flexed to 90 degrees at knee and hip. 2 providers position themselves on opposite sides of the patient and each places their arm under the patient’s calf/popliteal region and their hand on the opposite providers shoulder. A 3rd person is required to stabilize the pelvis. Axial traction is generated by the providers slowly standing up. Gentle internal and external rotation can facilitate successful reduction
The radial nerve is susceptible to compressive neuropathy against the spiral grove of the humerus which can lead to neuropraxia.
When the upper arm is compressed against a chair back or bar edge sometimes from a lost battle with alcohol: Saturday night palsy.
When another individual sleeps on someone’s arm overnight compressing the radial nerve: Honeymoon palsy
From nerve compression from improper technique with crutches: Crutch palsy
If diagnosis not clear from history, DDx includes other entities that can also present with isolated wrist, thumb/finger drop
Horses: Radial verve palsy, CVA, C7 compression
Zebras: Lead toxicity, acute porphyrias (often polyneuropathy but upper extremity before lower and frequently distal extensors
Careful history and exam important in differentiating
In cases of peripheral compression against the spital groove the triceps maintains strength.
The distal extensors lose strength (wrist and fingers)
Including the thumb abduction (abductor pollicis longus is radial-innervated)
AND so will the brachioradialis
The brachioradialis (despite being a forearm flexor) has dual innervation from the radial nerve in 80% of people.
Brachioradialis strength is often preserved in a central lesion.
Best tested with arm supported on a surface in mid pronation/supination (hammer curl position) and have patient flex against resistance and evaluate muscle strength and bulk.
Head Impact Exposure and Concussion Incidence
There has been a major focus on head impact biomechanics as a cause of single-impact concussion in football.
The role of repeated subclinical (without diagnosed concussion) head impact exposure (HIE)
during the preseason and regular season may also be contributory.
There may exist individualized concussion tolerance levels. This threshold may be reduced by the burden of sustained subconcussive impacts
NCAA Division 1 football athletes sustain a median of 426 impacts over the course of a football season
652 impacts/season in high school football
Total head impact exposure during the preseason occurred at 2x the rate of the regular season
This association was investigated over 1120 athlete seasons from 6 NCAA D1 football programs across 5 years
Head Impact Telemetry was used to record head impact exposure
Elevated preseason HIE was strongly associated with preseason and in season concussion incidence
Total season HIE was strongly associated with total season concussion incidence.
Conclusion: There is a prolonged effect of HIE on concussion risk starting with preseason football.
Athletes with higher preseason HIE may have higher risk of concussion for the entire fall season.
In Practice:
In 2016, the Ivy League eliminated full contact practices from the regular season in addition to their existing limits on the amount of full contact in practice during the spring and preseason.
Currently, the NCAA has the following limitations: Teams won’t be allowed to hold full-contact practices on more than two days in a row. Each practice session is limited to only 75 minutes of full contact, in addition to a limit of two preseason scrimmages.
28-year-old male present with dorsal hand pain after “losing his temper”
On exam, you note dorsal swelling, tenderness, and deformity
AP, lateral and oblique views are obtained.
There is no rotational deformity but using the lateral view, you note that there is angulation
Measured as the shaft of the metacarpal as compared to the mid-point of the fracture fragment
Acceptable shaft angulation generally accepted to be less than 40°
Patient has greater that acceptable angulation so you have to perform closed reduction
After appropriate pain control consider the “90-90 method.”
Flex the MCP, DIP, and PIP joints to 90 degrees.
This positioning stretches the MCP collateral ligaments helping to optimize reduction
Next, apply volar pressure over the dorsal aspect of the fracture site while applying pressure axially to the flexed PIP joint.
Best demonstrated below
https://www.youtube.com/watch?v=40irKoUJqsM
4-year-old patient comes to the ED for an unrelated complaint and you notice that his knees appear to be touching while his ankles remain apart.
Genu Varum or “knock knees” may be caused by Infantile Blount’s disease
-A progressive pathologic condition causing genu varum in children between ages 2 to 5
- Centered at the tibia
-Bilateral in up to 80%
-More common in boys
-Leg length discrepancy
- Articular incongruity
Risk factors: Early walkers (<1 year), overweight, large stature, Hispanic and African American
Results in disruption of normal cartilage growth at the MEDIAL aspect of the proximal tibia while LATERAL growth continues normally
May complain of knee soreness or subjective instability
On physical exam
Focal angulation of the proximal tibia
Lateral thrust during stance phase of walking (brief lateral shift of proximal fibula and tibia)
No tenderness or effusion
Imaging: Plain film shows varus deformity of the proximal tibia with medial beaking (beak like appears of bone) and downward slope of the proximal tibia metaphysis (increased metaphyseal-diaphyseal angle)
https://paleyinstitute.org/wp-content/uploads/blounts1.jpg
Treatment depends upon the age of the child and the severity
Successful in up to 80%
Note: In adolescent variant bracing is ineffective and surgery is only treatment
: Genu varum is normal in children <2 years old and becomes neutral at 14 months
DDX: Physiologic varus, Rickets
9-year-old male left hand dominant, presents with left elbow pain.
He is a future “star pitcher,” says his coach dad. “Doc, I bet you didn’t know that although only 10% of people throw with their left hand almost a 1/3rd of MLB pitchers are lefties. He is 3x more likely than a righty to pitch in MLB.” “Maybe I’m asking him to throw too much.”
Hx: Lateral elbow pain and “stiffness” worse with activity that is better with rest
PE: Lateral elbow tenderness (capitellum) with slight (approx. 20 degrees) decreased loss of extension. Minimal swelling noted.
Dx: Panner's disease refers to osteochondrosis of the capitellum (similar to Legg Calve Perthes). Likely due to AVN from repetitive trauma. May also be due to endocrine disturbances.
Affects the dominant elbow of boys between the ages of 5 and 10
Associated with the repetitive trauma of throwing or gymnastics.
Must be differentiated from osteochondrosis dissecans which occurs in the older child >13yo when the ossification of the capitellum is complete
Radiology:
The articular surface of the capitellum may appear irregular or flattened with areas of radiolucency (43%). Loose bodies not seen with Panners, much more likely with OCD lesions.
Treatment: Ice and NSAIDs. Avoid pitching/gymnastics etc. until full radiographic and clinical healing. If significant pain and/or swelling place patient in long arm posterior splint for 7-10 days. Resolution may take several months and up to one year.
A recent study investigated the association between concussion and subsequent mental health conditions in a pediatric population.
Retrospective cohort study. Pediatric patients aged 5 to 18 years who presented to an ED, PCP or mental health practitioner from April 2010, to March 2020, in Ontario, Canada.
Primary outcome: Time to first diagnosis with a mental health condition during follow-up
Secondary outcomes: 1) self-harm 2) psychiatric hospitalization 3) death by suicide.
Mental health conditions: anxiety and neurotic disorders, adjustment reactions, behavioral disorders, mood and eating disorders, schizophrenia, substance use disorder, suicidal ideation, and disorders of psychological development.
Study group, almost 450,000 patients. Age and sex matching between those with concussion and those who experienced an orthopedic injury.
A significant association (P < .001) was found between concussion and mental health conditions
A significant association emerged between concussion and self-harm and psychiatric hospitalization
No association with suicide
Conclusion: Concussion was significantly associated with risk of mental illness, psychiatric hospitalization and self-harm but not death by suicide.
Concussed patients had an almost 40% higher rate of mental health conditions compared to controls (adjusted hazard ratio 1.39)
Take home: Screen patients who return to the ED with post concussive symptoms for mental health symptoms/concerns and provide appropriate awareness for parents
Treatment of Hamstring Strains in Athletes
28 year old athlete presents to the ED and diagnosed with a hamstring strain
Localized swelling, moderate pain and a small limp. Incomplete tearing of the muscle
He is worried that he will miss the remainder of his season and when he returns will reinjure the same hamstring
Consider referral to sports medicine/orthopedics
A recent study looked at use of ultrasound guided hematoma aspiration followed by platelet-rich plasma (PRP) treatment on recovery in acute hamstring injuries
55 male athletes between ages 18 -32 weighing between 170 and 260lbs
27 with treatment protocol plus rehabilitation and 28 treated conservatively (rehabilitation)
All had Grade 2 hamstring injuries diagnosed on MRI
Partial muscle tear (<50% cross sectional area)
Note: Grade 2 hamstring injuries are often associated with INTERmuscle hematoma and subsequent scarring. This can lead to persistent pain/discomfort and reinjury
Average return to play time was 32.4 days in the standard of care group
Average return to play time was 23.5 days in the intervention group (P<0.001)
Recurrence rate of hamstring strain was 28.6% in the standard of care group
Recurrence rater of hamstring strain was <4% in the intervention group (P=0.025)
Athletes with grade 2 hamstring injuries treated with hematoma aspiration and PRP injection into the strain had significantly shorter return-to-play and much lower recurrence rate that athletes treated with rehabilitation alone
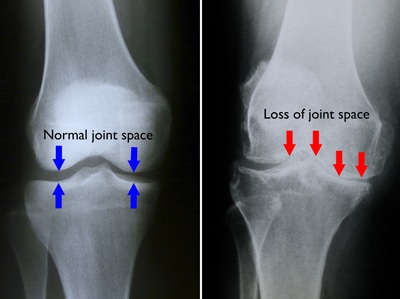
The knee is one of the most commonly affected joints from osteoarthritis (OA).
Patients will complain of knee pain, swelling and stiffness.
This leads to disability as it interferes with walking, using stairs at home and getting in and out of chairs and the bath without assistance.
Increasing incidence due to aging of the general population and rising rates of obesity.
Patients frequently present to the ED for knee pain and imaging is often obtained.
Diagnosis of knee OA can be made with an appropriate history and imaging that shows osteophytes and joint space narrowing.
The best views for knee OA include 1) PA weight-bearing & 2) 45 degree of knee flexion
https://d3i71xaburhd42.cloudfront.net/6f8ce215fb4bcd153a478187c9a6a2ae652a5fc4/250px/1-FigureI-1.png
Note: Weight-bearing radiographs will demonstrate greater joint space narrowing than non-weight-bearing radiographs
Of the 3 compartments of the knee, the medial tibiofemoral compartment is most commonly affected > patellofemoral compartment > lateral tibiofemoral compartment.
Examples of knee OA
https://roberthowells.com.au/wp-content/uploads/2016/04/A00212F02.jpg
https://orthoinfo.aaos.org/link/e7e6933819db4020bc2f3822c45c538f.aspx
23 y/o otherwise healthy Male presents for approx. 3 month history of Right leg mass. It is painful with activity (deep and sharp) but not enlarging. Patient remembers a fall from a bicycle 6 months ago, with negative imaging for fracture.
What is the diagnosis?
https://plinthsandplatforms.files.wordpress.com/2016/06/screen-shot-2016-06-20-at-10-58-18-am.png
https://radsource.us/wp-content/uploads/2019/02/1E.jpg
Quadriceps contusion
Mechanism: Blunt trauma from ball, helmet, stick
Usually to the central region
Damage to highly vascular area of the muscle and to local blood vessels can cause hematoma formation
Typical trauma history and pain worse with muscle activation (knee flexion)
Physical exam: Bruising, tenderness, palpable mass/hematoma
Goals of care: Minimize intramuscular bleeding
Treatment: NSAIDS, crutches, unique type of immobilization
Attempt to increase resting length of the quadriceps muscle to facilitate early healing and return to function
Note: Left untreated, large contusions may result in myositis ossificans
Hamstring Injury
Prevalence varies by sport ranging from 8 to 25 percent with a high recurrence rate frequently during the ensuing sport season, usually in next 2 months but may extend up to one year!
Highest in sports that involve rapid acceleration and deceleration
3 highest risk sports - football and men’s and women’s soccer
Average time lost 17-21 days
Injury much less common in younger athletes
The hamstring is composed of three muscles: the biceps femoris, semitendinosus, and semimembranosus.
Primarily involved in knee flexion and hip extension
Biceps femoris is most commonly injured
https://www.ncbi.nlm.nih.gov/books/NBK539862/figure/article-28873.image.f1
Simple grading system using 3 grades
Grade 1 – mild strain
Grade 2 – Partial tear
Grade 3 – Complete tear
Proximal injuries are more common than distal injuries, occurring at the musculotendinous junction
Avulsion fractures of the ischium occur rarely occur in adults but may occur in skeletally immature athletes
https://radiopaedia.org/cases/ischial-tuberosity-avulsion
When watching a sporting event you will see the athlete grab the buttock or upper thigh. They usually cannot return to play. Most grade 2 or 3 injuries will require crutches. If seeing them the following day significant bruising may be seen.
Numerous modifiable and non-modifiable risk factors have been identified including:
*Weakness of ipsilateral quadriceps or contralateral hamstring, hamstring, hip & quadriceps tightness/poor flexibility, poor warm-up, sudden increased training volume and muscle fatigue.
*Older age (risk increase may begin as early as age 23)
Prior hamstring injury (up to 6x increased risk)
**Premature return to sport increases the risk of reinjury
Differential Diagnosis: Lumbar radiculopathy, sciatic nerve irritation or compression, stress fracture of femur.
Refer to sports medicine/orthopedics for avulsion injuries, complete proximal complete tears and partial or complete distal tears
Caffeine is probably the most wildly used and studied drug/supplement in the world.
It has been shown to enhance exercise capacity and performance.
Mechanism of action is likely multifactorial and involves adenosine receptor antagonism via direct CNS action improving mental alertness, reaction time and reducing the perceived exertion rate (pain).
To no surprise, amateur and elite athletes use caffeine to improve performance.
The well-accepted dosage of caffeine to improve performance is between 3 and 6 mg/kg, approximately 60 min before exercise. This dosage promotes (between 1 and 8%) performance gains in aerobic exercises and exercises with high glycolytic demand from cyclists to tennis players to weightlifters.
Consider the lower end of this range if interested in trying this on your own.
In an evaluation of 20,686 urine samples of elite athletes, almost 75% of the samples contained caffeine in concentrations higher than 0.1 μg/mL
Caffeine also increases maximal oxygen uptake (VO2 max)
23 elite athletes were tested twice with and twice without caffeine.
Randomized, double-blinded, placebo-controlled study.
Caffeine 4.5 mg/kg taken 45 minutes before exercise
Measures: Time to exhaustion and VO2 max.
Caffeine increased time to exhaustion and VO2 max, thereby increasing overall performance.
If you are going to incorporate using caffeine before your next workout, I suggest espresso shots for extra caffeine without the volume of a large cup of coffee. Beware of known side effects such as jitters, anxiousness and difficulties with sleep if taken later in the day. Also consider stomach upset digestive issues, and increased heart rate.
Happy Holidays!!!!
Presentations of Fracture in Nursemaids Elbow
Study group: Visits by children younger than 10 years, with a diagnosis of radial head subluxation at 1 of 45 pediatric EDs from 2010 to 2018.
Retrospective cohort study of 88,466 ED visits for radial head subluxation
Outcome: Missed fracture (return visit for upper extremity fracture within 7 days of the index visit).
Results
Median patient age was 2.1 years,
59% of visits were by female patients,
60% of cases occurred in the left arm.
Radiography was performed at 28.5% of visits (Range 19.8% to 41.7%.)
Extremity fractures were observed in 247 cases, representing 0.3% of the cohort.
The odds of missed fracture were higher in:
Summary:
Only 0.3% of children with a diagnosis of radial head subluxation subsequently received a diagnosis of an upper extremity fracture within 7 days of the index visit.
Missed fractures were commonly about the elbow such as a supracondylar fracture. However, this study also found a significant proportion of missed fractures in other locations (e.g. shoulder, wrist), highlighting the importance of a careful physical examination, and the limitations of localizing pain in younger children.
Recurrence was common, and the risk of recurrence decreased with increasing age at first presentation. Overall, radial head subluxation recurrence was 8.7% after the first visit VERSUS 12%-13% in children younger than 2 years. THese patients are likely to return to the ED with a recurrence within 2 years. These findings should help inform anticipatory guidance to parents regarding the risk of recurrence based on their child’s age.
The classic mechanism for nursemaids elbow is axial traction on a pronated forearm and extended elbow.
The force allows a portion of the annular ligament to slip over the radius.
Consider this diagnosis with other mechanisms of injury especially if the exam is not suggestive of fracture.
Suspect in a patient in minimal distress with arm held semi flexed and pronated.
A recent retrospective study looked at other mechanisms of injury.
69 subjects with a median age of 2.5 years
The most common mechanisms of injury were fall (57%), direct hit to the elbow (16%), and rolling over (7%).
Some studies note the left elbow is more commonly involved but this is likely due to most guardians being right-handed, thereby holding the child’s left hand


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}