This German retrospective study compared the prehospital use of ultrasound by trained paramedics and compared their findings to in-hospital diagnosis and image results. The authors found:
“Diagnostic accuracy, defined as the concordance between prehospital POCUS-based working diagnoses and final in-hospital diagnoses, was particularly strong for lung ultrasound (pneumothorax, pulmonary edema, pneumonia and pleural effusion; sensitivity 91.7%, specificity 100%) and eFAST (sensitivity 100%, specificity 96.5%), while for the abdominal ultrasound examinations, the specificity was 70% and sensitivity was 71.43%.”
This study sets the stage for future prospective work looking at prehospital US use by paramedics.
This systematic literature review looking at gender differences in trauma care reveals:
A modified 2 round Delphi study was used to create 57 learning objectives in geriatric care for European prehospital providers. Based on in-hospital learning objectives and literature, these experts came up with what appears to be a very reasonable and helpful list of education objectives for pre-hospital providers that could easily apply to emergency medicine learners as a whole. Here is their table:
https://link.springer.com/article/10.1186/s13049-026-01550-3/tables/3
In this retrospective cohort study looking at splenic injury management and outcomes in the UK, patients over age 65 had much higher mortality and were more often managed conservatively (vs splenectomy or embolization) despite having a lower splenic injury grade and lower overall injury severity score compared to those under 65. Many factors are possible here including frailty, reluctance to intervene in older patients, and lower mechanism of injury bias away from evaluation and management.
Looking at trauma patients evaluated at a major trauma center before and after EMS switched from semi-rigid to soft cervical collars for immobilization found no difference in adverse outcomes. Add this to the mounting evidence that our current practice of spinal immobilization may not offer any benefit.
Bradycardia accompanying hypotension can be found in spinal cord injury (loss of autonomic reflex), beta blocker and calcium channel blocker overdose, intrinsic cardiac electrophysiologic derangement, and, often forgotten, intrabdominal hemorrhage. In the appropriate setting (blunt trauma, ruptured ectopic pregnancy), bradycardic hypotensive patients should be considered the same as tachycardic hypotensive patients and get a work up and treatment focused on Hemoperitoneum.
Using a database of 300,000 patients and applying a predictive measure for mortality, these authors found that patients over 66 with a high likelihood of 6 month mortality at the time of presentation were more likely to be admitted to an ICU when they presented to an ED. The authors conclude there is much work to be done regarding discussion of goals of care based on this information.
Looking at a national database, this study concluded the use of low titer O whole blood during trauma resuscitations was increasing at level one centers but not at level 2 and 3 centers. Is this a representation of the national blood supply as whole blood is harder to stock? We need to understand this trend to assure equal and appropriate care to trauma patients across the country.
Another study, this one from New Zealand, showing older trauma patients with similar injury severity score had less trauma team activations and higher mortality.
This case report reminds us that vasculitis is an inflammatory process that attacks blood vessels leading to organ dysfunction. The etiology can be a hypersensitivity reaction (think drugs) or an IgA mediated process secondary to infection (Strep or Mycoplasma). In this case, concomitate use of NSAIDS (very common etiology of hypersensitivity) and Mycoplasma lead to vasculitis. Treatment ranges from supportive care, to steroids to immunosuppressive agents such as azathioprine.
Of 925 ED headache patients in this meta analysis comparing extrapyramidal side effects of bolus vs. continuous infusion of metoclopremide the majority of the reactions occurred in the bolus group.
When compared to saline(!) trauma patients with a high injury severity score who received ketamine via pca for pain control had better quality of life indicators at 1,3, and 6 months post injury.
Bottom Line: arrival temperature had no prognostic value in non-septic older patients. Hypothermia in sepsis, but not fever, predicted mortality.
In a single level 1 trauma center there were 274 patients age over 55 evaluated for falls in a one year retrospective period. Their blood toxicology was reviewed for presence of alcohol, opioids, benzodiazepines and cannabinoids. The authors found:
“detection rates were 21.2% for opioids, 18.6% for ethanol, 13.9% for benzodiazepines, and 9.1% for cannabinoids. Injuries identified included 16.4% spinal fractures, 9.5% extremity fractures, 7.7% hip/thigh/pelvic fractures…In this study, nearly 20% of adults 55+ presenting for fall-related trauma recently used substances that impair psychomotor function.”
An area for injury prevention research and intervention would be to screen patients over age 55 for substance use, consider prescribing patterns in this age group (benzodiazepines) , and discuss with patients fall risk avoidance.
A case report on use of the abdominal aortic and junctional tourniquet in a 27 year old female with hemorrhagic shock secondary to a pelvic fracture after a 10 meter fall demonstrated improved blood pressure and stabilized vasopressor use prior to operative intervention. This device has been used in battlefield situations, however very few reports of civilian use exist. Much more data is needed, however, it is a device to be aware of for future use.
Popliteal artery injuries are very rare (4% of all vascular injuries).
The majority of injuries are secondary to penetrating injury (70+%)
Blunt mechanism of injury has the higher rate of amputation.
Prolonged ischemia time (from injury to repair greater than 6 hours) leads to higher rates of amputation
Hard signs of vascular injury should prompt X-ray imaging of the knee, femur, and lower extremity and transfer to an operating room for repair.
Soft signs ("a history of significant bleeding which has ceased, nonexpanding hematomas, and the presence of an Ankle-Brachial Index of less than 0.9") and shotgun injury should prompt CT angiogram to evaluate arterial injury.
In a metanalysis of studies looking at intercranial hemorrhage in fall patients older than 65 years, the following were unadjusted odds ratio risk factors for finding an ICH in this patient population:
suspected open or depressed skull fracture , signs of basal skull fracture ), reduced baseline Glasgow Coma Scale score , focal neurologic signs , seizure , vomiting , amnesia , loss of consciousness , headache ), external sign of head trauma , male sex , chronic kidney disease , preinjury single antiplatelet , and dual antiplatelet medication .
Preinjury anticoagulant was not a significant risk factor.
When looking at adjusted odds rations only focal neurologic signs , external sign of head trauma , loss of consciousness , and male sex were found to be associated with intercranial hemorrhage.
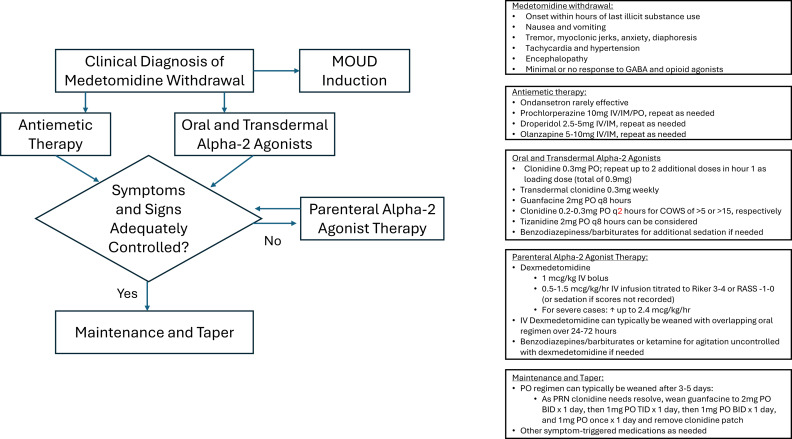
The US drug supply has been found to contain medetomidine as an adulterant to heroine/fentanyl. It is a potent tranquilizer used in animals. It is an alpha 2 blocker (similar pharmacology to clonidine and xylazine). Exposure to this drug can induce withdrawal symptoms to include anxiety, tremor, diaphoresis, nausea, vomiting, agitation, sympathetic hyperactivity, and delirium. Withdrawal can start within 4-6 hours of last use.
Treatment for withdrawal is outlined in this diagram.
An English study describes 30 patients that jumped from a single bridge of 30 meters (98 feet) over the course of 12 years. Twenty six landed in the water. The injury pattern for those landing in water was described as “Hypothermia was the most common presentation (n = 23), followed by pneumothoraces (n = 14), rib fractures (n = 10), thoracic vertebral fractures (n = 9) and lung contusions (n = 8). Lower water temperatures at the time of the incident (p = 0.008) and lower patient body temperatures on arrival to hospital (p = 0.002) were significantly associated with increased 30-day mortality.”
The small group landing on land had more pelvic and extremity fractures than the water group and none had hypothermia.
Remember to start aggressive rewarming in patients who fall into water!
This small study from South Africa shows stab wounds to the chest with a pneumothorax less than 0.5 cm that were managed conservatively had completely resolved on 12 hour repeat chest X-ray. This could facilitate earlier discharge of these patients. It also supports conservative (non-tube placement) approach to asymptomatic small pneumothoraces from stab wounds.
