Recently a review paper was published regarding the duration of observation in heroin overdose patients who received naloxone.
It made several conclusions regarding heroin overdose:
It should be pointed out that this is a review paper of limited number of articles with variable quality. Additionally, the clinical history of “heroin use” may be unreliable as fentanyl and novel synthetic opioids are also sold as “heroin.” Providers should exercise appropriate clinical judgement when caring for these patients.
Recently, a retrospective study of unintentional buprenorphine/naloxone exposure among pediatric population was published. All patients were evaluated by toxicologists at the time of initial hospital presentation (or transfer) at the study center.
Bottom line
US, Canadian and European critical care and toxicology societies recently published a consensus recommendation is the management of CCB poisoning.
Bottom line:
1. First line therapy remains unchanged: IV calcium, atropin, high-dose insulin (HIE) therapy, vasopressor support (norepinephrine and/or epinephrine).
2. Refractory to first line therapy: increase HIE, lipid-emulsion, transvenous pacemaker
3. Refractory shock, periarrest or cardiac arrest: Above (#1 & #2) plus ECMO if available.
Fall clean up = Poison Ivy, oak, sumac (Toxicodendron species) which is ubiquitous in North America but it can also be found in British Columbia, Mexico and in parts of Asia. These plants are truly the scourge of outdoor enthusiasts and agricultural workers responsible for up to 40 million cases of miserable often temporarily incapacitating rashes annually.
Fast Facts:
Treatment Tips:
Naloxone has been used to reverse opioid-induced respiratory depression for decades. The “standard” dose of opioid intoxication has been 0.4 mg. However, over the past decade, initial naloxone dose for opioid intoxication has evolved to recommend a lower initial dose (0.04 – 0.05 mg).
A recent article by Connors et al. reviewed 25 medical resources (internet, medical texts and study guides) of different medical specialties (internal medicine, medical toxicology, emergency medicine, pediatrics, anesthesiology, pain medicine and general medicine)
Findings:
Recent editions of emergency medicine text (Rosen’s and Tinitinalli) recommend using 0.04 – 0.05 mg IV in ED patients with history of opioid dependence. Higher doses of naloxone are recommended for non-opioid dependent/apneic patients.
However, history of opioid dependence is difficult to obtain in patients with opioid induced CNS/respiratory depression.
Administering 0.4 mg or higher dose may/can acute agitation or opioid withdrawal symptoms that can utilize more ED resources to calm agitated patient/management of withdrawal. Thus it may be prudent to use low-dose strategy (0.04 mg IV with titration) to minimize the risk of precipitating naloxone-induced opioid withdrawal/agitation.
Bottom line:
In opioid-induced respiratory depression/apneic patients:
To make 0.04 mg naloxone solution:
Antipsychotic as a class has diverse range of toxicity. The atypical (2nd generation) antipsychotics are considered to possess less toxicologic manifestation compared to the typical (1st generation) antipsychotics - lower K channel blockade and minimum Na channel blockade properties. However, select atypical antipsychotics overdose can results in significant morbidity in addition to sedation.
Alpha-1 blockade (hypotension)
Antimuscarinic effect (anticholinergic toxicity)
Delayed rectifier K channel blockade (QT prolongation)
Bottom line: Although lethal overdose from atypical antipsychotics are rare, they can result in significant clinical toxicity when ingested alone or in combintation with other classes of medications.
In pediatric population, small dose or single pill ingestion can potential result in severe or lethal toxicity.
Clinicians should be mindful of potential toxicity following xenobiotic exposure (below) in pediatric population, especially under the age of 5 years old, even if the patient may initially appear asymptomatic.
Suspected ingestion of above medications/xenobiotics may warrent observation up to 24 hours in asymptomatic pediatric population.
Drug-induced hypoglycemia is an often severe and symptomatic. It is a potentially preventable cause of significant morbidity. In one large study, it accounted for 23% for hospital admissions due to adverse drug events and 4.4% of overall admissions. The majority of hypoglycemic events occur with insulin and sulfonylureas. However, multiple drugs can affect glucose homeostasis and have been cited to cause hypoglycemia in therapeutic dose alone or in combination with other medications or illness. Factors that predispose to low blood sugar include reduced food intake, age, hepatic and renal disease, and severe infection. Beware of the possibility of inducing hypoglycemia in patients taking the following:
Agents with lesser quality evidence as predisposing medications or illnesses were present:
Drugs induced hypoglycemia should always be considered in the differential diagnosis of every patient presenting with low blood glucose. Octreotide antagonizes pancreatic insulin secretion and should be considered for first-line therapy in the treatment of sulfonylurea-induced hypoglycemia particularly when glucose levels cannot be maintained by dextrose infusions. Octreotide is administered 50 mcg subcutaneously (1-10 mcg in children) every 12 hours.
Recently, there have been several news reports regarding the emergence of synthetic opioids in the U.S. and Canada. There are multiple synthetic opioids that have been identified as potential agents of abuse including W-18, U-47700, fentanyl derivatives, AH-7921 and MT-45. These compounds share a similar story with synthetic cannabinoid where they were synthesized for research purpose or by pharmaceutical companies but were not marketed. They are often sold as “research chemicals” over the internet.
In July 2016, three case reports have been published regarding several cases of U-47700 intoxication in San Diego, CA and Dallas, TX.
It is unknown if currently available heroin is cut with above mentioned synthetic opioids. Like other opioid receptor agonists, administration of naloxone will likely reverse the opioid toxidrome. But clinical experience in reversing synthetic opioids intoxication with naloxone is limited.
Bottom line:
Irrespective of whether an ED patient is exposed to synthetic opioids or "traditional" opioids of abuse (prescription opioid pain medication or heroin), the management of opioid intoxication management remains unchanged for respiratory depression.
Laundry detergent pods were introduced in 2012 to make washing clothes more "convenient." Since then, pediatric exposures to laundry detergent pods have increased as the use of these detergent pods have become more common in homes. Like other household chemical exposure, small, colorful candy like appearances of laundry detergent pods can attract the attention of < 3 years old children resulting in unintentional exposure due to curiosity or taste.
Most frequent clinical effects (2013 - 2014 national poison center data) from exposure to detergents in general (laundry detergent pods and nonpods & dishwasher detergent):
Laundry detergent pod vs. nonpods:
Laundry detergent pods (only) also resulted in following:
Cases of caustic exposure-like injuries have also been reported (corneal abrasion and esophageal injury)
Bottom line:
Pediatric laundry detergent (nonpods) exposures usually have self-limited symptoms. However, laundry detergent pod exposure can cause more serious clinical effects that may require hospitalization.
Loperamide is a peripheral mu-opioid receptor agonist that is found in over the counter anti-diarrheal medication. Following the trend of opioid abuse epidemic, loperamide has been promoted on online drug-use forum as a treatment for opioid withdrawal and as a possible alternative to methadone. At the same time, recreational use of loperamide has been increasing as an opioid alternative. Unlike therapeutic use of loparamide (2 – 4 mg), loraparmide abusers take supratherapeutic doses (e.g. 50 – 100 mg) to penetrate the CNS to produce opioid effects.
In published case reports, loperamide caused cardiac Na channel blockade (similar to TCA and bupropion) and K channel blockade, resulting in EKG changes including QRS interval > 100 msec with terminal R wave in aVR and QTc prolongation, respectively. Loperamide associated death has also been reported (autopsy finding), although the exact cause of death was not determined.
It is unclear if administration of NaHCO3 can reverse the cardiac Na channel blockade as in TCA and bupropion as the clinical experiences have been limited.
Bottom line:
Ketamine is gaining traction as a prehospital option for managing severe agitation or excited delirium syndrome. Previous reports have mostly been case series, but a new prospective study adds some important information that may help delineate ketamine's role in this setting. [1] The study and an accompanying commentary are both open access. [2]
What They Did
Open-label before-and-after prospective comparison of haloperidol (10 mg IM) versus ketamine (5 mg/kg IM) for the treatment of acute undifferentiated agitation.
What They Found
Appliation to Clinical Practice
Bupropion (Wellbutrin, Zyban) is one of the most frequently prescribed antidepressants and smoking cessation agents. A lesser incidence of undesirable side effects such as weight gain and sexual dysfunction when compared to other antidepressants lends to its popularity. Bupropion's mechanism of action is only partially understood but it is known to be a norepinephine dopamine reuptake inhibitor and anticholinergic receptor blocker at certain nicotinic receptors. Bupropion has a monocyclic structure similar to amphetamines. Seizures are a major concern in overdose. When first released, Bupropion was initially withdrawn from the market due to its narrow therapeutic window with seizures occurring at doses as low as 450 mg.
Patients with chronic digoxin toxicity generally have multiple co-morbidities such as renal failure, dehydration, and cardiac failure. Sick patients with chronically high digoxin levels may have more than just digoxin toxicity as the cause of illness.
A New Study
Prospective observational study with the primary objective to investigate changes in free digoxin concentrations and clinical effects on heart rate and potassium concentrations in chronic digoxin poisoning when digoxin immune Fab are given.
What They Found
One to two vials of digoxin immune Fab initially bound all free digoxin confirming Fab efficacy. However, this was associated with only a moderate improvement in HR (49 to 57 bpm) and potassium (5.3 to 5.0 mmol/L).
Application to Clinical Practice
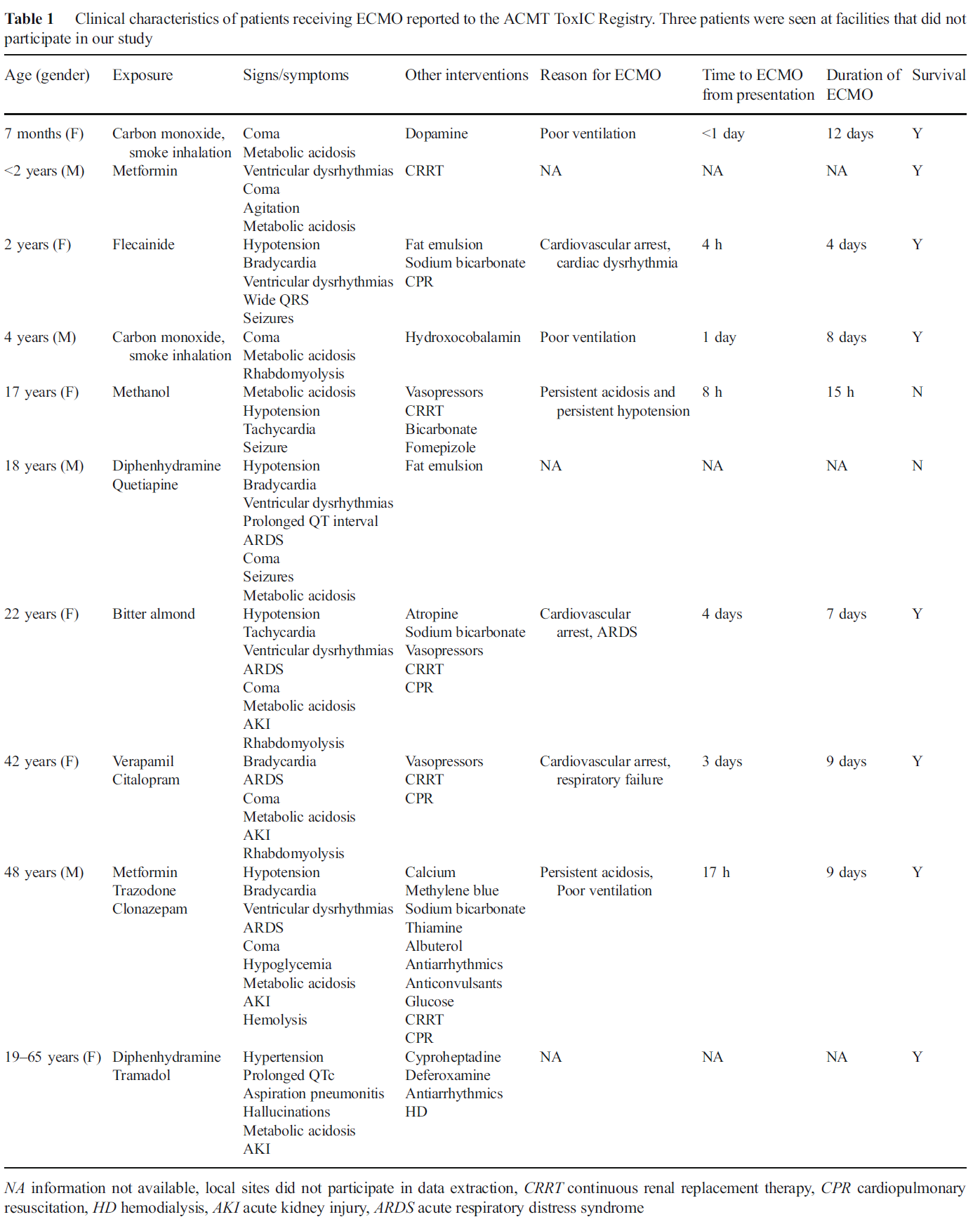
The American College of Medical Toxicology's ToxIC Registry is a self-reporting database completed by medical toxicologists across 69 insitutions in the US.
Application to Clinical Practice
In settings where ECMO is available, it may be a potential treatment option in severely poisoned patients. From the limited data, ECMO was generally administered prior to cardiovascular failure and might be of benefit particularly during the time the drug is being metabolized.
Table from the Case Series
[CORRECTION]: Versed dose is 2-2.5 mg total not mg/kg
Patients with severe agitation present a unique challenge to the emergency department. Acute delirium is often due to psychostimulants such as cocaine, amphetamines, PCP, or synthetic cannabinoids, alcohol, or psychiatric illness. These patients require urgent evaluation necesssitating the use of physical and chemical restraints, not only for their own safety but also the hospital staff's. Fingerstick glucose, pulse oximetry, and vital signs must be expeditiously obtained. Severely agitated combative patients who are physically restrained are at high risk for morbidity from asphyxiation, hypermetabolic consequences (acidosis, hyperthermia, rhabdomyolysis), and death can occur.
Ketamine is phencyclidine derivative that causes dissociative state between the cortical and limbic systems which prevents the higher centers from preceiving visual, auditory, or painful stimuli. Ketamine has a wide safety profile and has been used worldwide for many years with few complications. It possesses ideal characteristics for rapid sedation of agitated patients:
Experience with Ketamine in patients with excited delirium has shown good initial control of agitation however, patients often require additional medications for deeper or longer duration of sedation. Benzodiazepines are recommmended as second line agents particularly intravenous or intramuscular Midazolam 2-2.5 mg /kg.
Acute cocaine toxicity can manifest with several cardiovascular issues such as tachycardia, dysrhythmia, hypertension, and coronary vasospasm. A new systematic review collated all of the available evidence for potential treatment options. Here is what the review found (there is also an 'other agents' section for medications with less published reports):
Benzodiazepines and other GABA-active agents: Benzodiazepines may not always effectively mitigate tachycardia, hypertension, and vasospasm from cocaine toxicity.
Calcium channel blockers: Calcium channel blockers may decrease hypertension and coronary vasospasm, but not necessarily tachycardia.
Nitric oxide-mediated vasodilators: Nitroglycerin may lead to severe hypotension and reflex tachycardia.
Alpha-adrenoceptor blocking drugs: Alpha-1 blockers may improve hypertension and vasospasm, but not tachycardia, although evidence is limited.
Alpha-2-adrenoceptor agonists: There were two high-quality studies and one case report detailing the successful use of dexmedetomidine.
Beta-blockers and alpha/beta-blockers: No adverse events were reported for use of combined alpha/beta-blockers such as labetalol and carvedilol, which were effective in attenuating both hypertension and tachycardia.
Antipsychotics: Antipsychotics may improve agitation and psychosis, but with inconsistent reduction in tachycardia and hypertension and risk of extrapyramidal adverse effects.
Sodium bicarbonate: Twelve case reports documented treatment of dysrhythmia with IV sodium bicarbonate, with seven reporting successful termination.
The authors note that "publication bias is a concern, and it is possible that successful treatment and/or adverse events have not been reported in some of the publications, and in general."
Pure opioid agonists such as Morphine, Hydromorphone, and Fentanyl stimulate opioid receptors and are the most potent analgesics. Fentanyl and fentanyl analogues are up to 100 times more powerful than morphine and 30-50 times more powerful than heroin.
W-18 is a highly potent opioid agonist with a distinctive chemical structure which is not closely related to older established families of opioid drugs. While Fentanyl is approximately 100 times more powerful than Morphine, W-18 is about 100 times more powerful than Fentanyl.
Colchicine is an alkaloid compound found in Colchicum autumnale that is often mistaken by foragers as wild garlic (Allium ursinum). Unintentional ingestion wild garlic or therapeutic misadventures among elderly population with history of gout often result in unintentional toxicity.
It is a potent inhibitor of microtubule formation and function involved in cell division and intracellular transport mechanism. Thus toxicity is related to diffuse cellular dysfunction of all major organs and results in significant morbidity and mortality.
Colchicine toxicity occurs in three phases:
| Phase | Time | Signs and symptoms | Therapy |
| I | 0 – 24 hr | · Nausea, vomiting, diarrhea · Salt and water depletion · Leukocytosis | · Antiemetic · GI decontamination · IV fluids · Observation for leukopenia |
| II | 1 – 7 days | · Sudden cardiac death (24 – 48 hr) · Pancytopenia · Acute kidney injury · Sepsis · Acute respiratory distress syndrome · Electrolyte imbalance · Rhabdomyolysis | · Resuscitation · G-CSF · Hemodialysis · Antibiotics · Mechanical ventilation · Electrolyte repletion |
| III | >7 days | · Alopecia (2-3 weeks later) · Myopathy, neuropathy, myoneuropathy. |
|
Management
In September 2013, an international group representing major societies in toxicology and nutrition support began collaborating on a comprehensive review of lipid use in poisoning. Six total papers will be published, with the most recent two made available online this week. Here are the available (and forthcoming) papers:
Gosselin S, et al. Methodology for AACT evidence-based recommendations on the use of intravenous lipid emulsion therapy in poisoning. Clin Toxicol 2015;53(6):557-64. [PMID 26059735]
Grunbaum AM, et al. Review of the effect of intravenous lipid emulsion on laboratory analyses. Clin Toxicol 2016:54(2):92-102. [PMID 26623668]
Levine M, et al. Systematic review of the effect of intravenous lipid emulsion therapy for non-local anesthetics toxicity. Clin Toxicol. 2016;54(3):194-221. [PMID 26852931]
Hoegberg LC, et al. Systematic review of the effect of intravenous lipid emulsion therapy for local anesthetic toxicity. Clin Toxicol. 2016;54(3):167-93. [PMID 26853119]
Hayes BD, et al. Systematic Review of Clinical Adverse Events Reported After Acute Intravenous Lipid Emulsion Administration. Clin Toxicol. 2016 Apr 1. [Epub ahead of print] [PMID 27035513]
The final paper, which is in process, is the consensus recommendations from the workgroup based on the 4 systematic reviews.