24 yo woman presents with syncope, abdominal pain, and normal menses 4 days prior. Urine HCG(+) and quantitative beta-HCG is 1300 with the transvaginal ultrasound seen below. Diagnosis?

(Please note the prior version of this pearl was incorrect with respect to the images referenced. This version is corrected.)
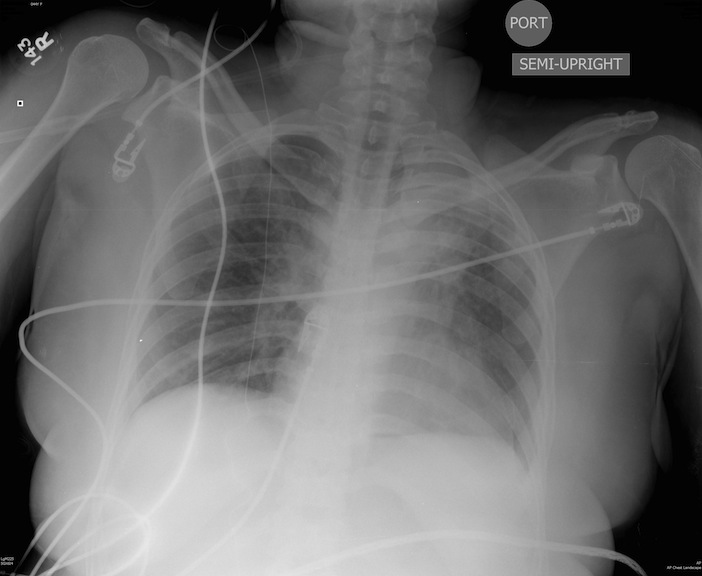
Patient s/p blunt chest trauma. CXR (image 1) vs. lung ultrasound (image 2), do you see any inconsistencies?
The optimal hemoglobin concentration during critical illness is unknown. Although a liberal transfusion strategy (Hb 10-12 g/dL) was once believed to be beneficial for hemodynamics, evidence suggests targeting a conservative strategy (Hb 7-9 g/dL) does not increase mortality, while the unnecessary transfusion of blood products can cause harm (transfusion associated lung injury, infection, etc.) in the non-hemorrhaging patient.
44 y/o female restrained driver s/p motor vehicle crash complaining of chest pain and shortness of breath.
Brain death is the permanent absence of cerebral and brainstem functions (coma, absent pupillary reflexes, no spontaneous respiration, etc.). Legally, brain death is equivalent to cardiopulmonary death.
If brain death is suspected, confirmation is necessary. The apnea test is most commonly used, evaluating for spontaneous breaths when disconnected from the ventilator. If apnea testing is not possible (e.g., ambiguous clinical exam or cardiopulmonary instability) ancillary testing is needed:

Boxer's (or Brawler's) Fracture
Posterior reversible encephalopathy syndrome (PRES) is a syndrome of visual loss, headache, altered mental status, and seizures, typically with severe hypertension. PRES usually occurs with hypertensive encephalopathy or ecclampsia, although cyclosporin and tacrolimus use have been implicated.
PRES is due to a combination of endothelial damage, impaired auto-regulation and increased cerebral perfusion pressure. Classic CT and MRI findings are parietal-occipital, cerebellar, or brainstem cortical and subcortical edema.
Early recognition and symptomatic treatment is key; IV anti-hypertensives (hypertensive encephalopathy), anti-epileptics (seizures), IV magnesium and emergent delivery (ecclampsia), and discontinuing offending medications (cyclosporin and tacrolimus).
With treatment, partial to complete recovery is normal, although residual neurological and visual deficits may persist.
The incidence and prevalence of thrombocytopenia in the ICU is poorly defined however, it has been found to be an independent predictor of death in the critically-ill. Increased mortality does not appear to be related to bleeding complications. On the other hand, survivors of critical illness tend to recover platelet faster as compared to non-survivors.
Thrombocytopenia in the critically-ill is a marker for systemic inflammation/infection although the exact mechanisms are unknown. Common risk factors associated with thrombocytopenia in the ICU population are:
Sepsis
Renal failure
High-illness severity
Organ dysfunction
Bottom line: Thrombocytopenia in the critically-ill is associated with increased mortality.
Linezolid is used for gram-positive infections resistant to conventional therapy (e.g., Vancomycin-resistant enterococcus and Methicillin Resistant Staph Aureus). Linezolid is an oxazolidinone, but more importantly it is a weak monoamine oxidase inhibitor (MAOI) and serotonin syndrome (e.g., altered mental status, neuromuscular abnormalities, autonomic instability) may occur when combined with selective serotonin re-uptake inhibitors (SSRIs) or with recent discontinuation of SSRI.
Be aware that the following drugs can precipitate serotonin syndrome when combined with Linezolid:
Mirtazpine Buproprion Fentanyl
Trazodone Buspirone Bromocryptine
Levodopa Lithium Amphetamines
Cocaine Codeine Reserpine
Ergots MAOI's
Non-Convulsive Status Epilepticus (NCSE) is generally under reported. An ICU study found 10% admissions for altered mental status (AMS) were eventually diagnosed as NCSE.
Pearls:
- Include NCSE in the AMS differential
- NCSE may occur with or without convulsive seizures
- Difficult to distinguish from a post-ictal state (14% of convulsive seizures convert to
NCSE)
- Reported mortality is up to 44%
Consider NCSE when:
- Seizure history / recent seizures
- Post-ictal period >1 hour
- Odd behaviors (e.g., chewing, blinking, personality change) and abnormal eye
movements (86% specific)
- AMS without structural, metabolic or traumatic etiology
- Patient intubated for status epilepticus
If you are unsure but suspicious of NCSE order a STAT EEG. Treat NCSE like a convulsive status.
Ocular sonography is a fast, simple, and non-invasive tool to detect elevated intracranial pressure (ICP) by measuring the optic nerve sheath diameter (ONSD). Several studies have shown a positive correlation between increased ONSD (>5.7mm) and elevated ICP (>20mmHg). Although ultrasound may not replace CT or MRI to diagnose the cause of the increased ICP, its use as a triage tool can expedite these tests.
The technique:
Please see the references below for more information and, as with any new technique please consult local experts prior to making clinical decisions.
Increasing literature demonstrates ICU delirium is bad. Delirium in mechanically ventilated patients is an independent predictor for long-term cognitive defects (e.g., managing money, following detailed instructions, reading maps, and developing dementia). The cited study found 80% of patients with ICU delirium had cognitive dysfunction at three months, and 70% had residual dysfunction at one year (33% had severe dysfunction).
You must be aggressive to prevent delirium:
- Implement daily assessment tools (e.g., CAM-ICU)
- Daily awakening and spontaneous breathing trials
- Early patient mobilization
- Aggressive pharmacological treatment of delirium
- For more information: www.icudelirium.org
Heliox is a mixture of oxygen and helium resulting in a gas less dense than air. In asthma, airway resistance causes turbulent airflow which increases the work of breathing. Heliox reduces airway resistance by increasing laminar airflow.
Benefits:
Better lung mechanics
Improved nebulizer delivery
Few known side-effects/complications
Drawbacks:
Expensive
Contraindicated in hypoxemic patients.
Paucity of large prospective randomized trials.
While you should always involve ID consultants when managing critically-ill HIV/AIDS patients on HAART, consider this; sub-therapeutic levels of anti-retrovirals may promote HIV resistance, potentially invalidating a class of drug for future use. Therefore, it may be advantageous to discontinue the drug(s) during critical-illness to avoid resistance.
Two examples leading to sub-therapeutic HAART levels in critical-illness:
(Sorry for the previously mislabeled pearl...)
Necrotizing soft tissue infections (NSTI) are on the rise and, despite improved surgical and critical care, over the years there has only been a mild reduction in mortality. Survival is associated with early diagnosis and treatment. Unfortunately, NSTI are not always obvious because deeper tissues made be involved first. Despite a validated scoring system and better radiology, our clinical suspicion still rules and relies on a meticulous history and physical exam.
Here are some subtle signs of NSTI:
Pain out of proportion to exam
Edema beyond region of erythema
Skin anesthesia
Skin erythema and/or hyperthermia
Epidemolysis
Skin bronzing
If NSTI is suspected, be vigilant! Start broad-spectrum antibiotics, begin appropriate resuscitation and involve your surgeons early.
Hyponatremia plagues many neurosurgical patients due to the syndrome of inappropriate secretion of ADH (SIADH) or the cerebral salt wasting syndrome (CSW). Both diseases may appear similar (hyponatremia, increased urine osmolarity, increased urine sodium, normal adrenal, renal and thyroid function), but there is one BIG difference. Patients with SIADH are euvolemic or hypervolemic (excess ADH causes fluid retention) whereas patients with CSW are fluid depleted (impaired renal handling of sodium and water). To differentiate, look for signs of hypovolemia: orthostatics, dry mucus membranes, hemoconcentration, pre-renal azotemia, and/or hemodynamics (IVC collapse anyone?).
Bottom line: Distinguish SIADH from CSW because the treatments are exact opposites:
SIADH: Fluid restrict
CSW: Give water and salt (i.e., 0.9% saline)
2. Distinguish artery from vein with compression and/or Doppler.*
3. Sterilely prep the site and ultrasound probe.
4. Cannulate the vein in the transverse or longitudinal plane.
Adrenal insufficiency (AI) can be a life-threating condition and is classified as primary (failure of the adrenal gland) or secondary (failure of hypothalamic- pituitary axis).
Common causes of primary adrenal insufficiency include autoimmune destruction, infectious causes (TB and CMV), or interactions with drugs (e.g., anti-fungals, Etomidate, etc.). Secondary causes are usually due to abrupt withdrawal of steroids after chronic use, although sepsis and diseases of the hypothalamus or pituitary (e.g., CVA) may occur.
Signs and symptoms include fatigue, weakness, skin pigmentation, dizziness, abdominal pain, and orthostatic hypotension; it should be suspected with any of the following: hyponatremia, hyperkalemia, hypoglycemia, hypercalcemia, low free-cortisol level, and hemodynamic instability despite resuscitation.
Treatment:
• Correct underlying the disorder
• Resuscitation and hemodynamic support
• Correct hypoglycemia and electrolyte abnormalities
• Treat with hydrocortisone, cortisone, prednisone, or dexamethasone +/- fludrocortisone (Note: dexamethasone is attractive choice in the ED because it will not interfere with ACTH stimulation test)
