The New England Journal of Medicine and Lancet both published studies evaluating idarucizumab for reversal of dabigatran. It is a monoclonal antibody fragment that binds dabigatran with high affinity. Dr. Ryan Radecki summarizes the two articles on his EM Lit of Note blog.
Here are a few take home points from these early studies:
Recently, there has been a surge in synthetic cannabinoid in the U.S., including the Baltimore area. According to U.S. poison control center data, there has been 229% increase in calls related to SC between January to May of 2015 compared to similar time period in 2014.
The most commonly reported adverse/clinical effects included:
End-organ injuries have been also reported in case reports, including AKI, seizure, MI, and CVA.
Synthetic cannabinoid includes a list of chemical compounds that are structurally different compared to THC – the active compound in marijuana. However, they possess full CB1 (cannabinoid) receptor agonism effect, unlike the THC, which is a partial CB1 receptor agonist.
These chemicals (particularly JWH series) were originally synthesized to study the effect of cannabinoid receptors. Overall, it is difficult to identify the compound and the dose within each packets of SC.
Commonly marketed names include: Spice, K2, K9, herbal highs, Scooby snax, WTF.
Table. Identified synthetic cannabinoids
| Chemical name | Chemical origin |
| JWH-018; JWH-073; JWH-250 | Laboratory of J.W. Huffman |
| CP47,497; CP47,497-C8; CP59,540; cannabicyclohexanol | Pfizer laboratory |
| HU-210 | Hebrew University laboratory |
| Oleamide | Fatty acid |
| UR-144 | CB2 receptor agonist |
| XLR-11, AKB-48, AM-2201, AM-694 |
|
Management: Majority of the patients with acute SC intoxication mostly requires supportive care, including benzodiazepine for acute agitation. However, ED providers should be mindful of potential end-organ injury.
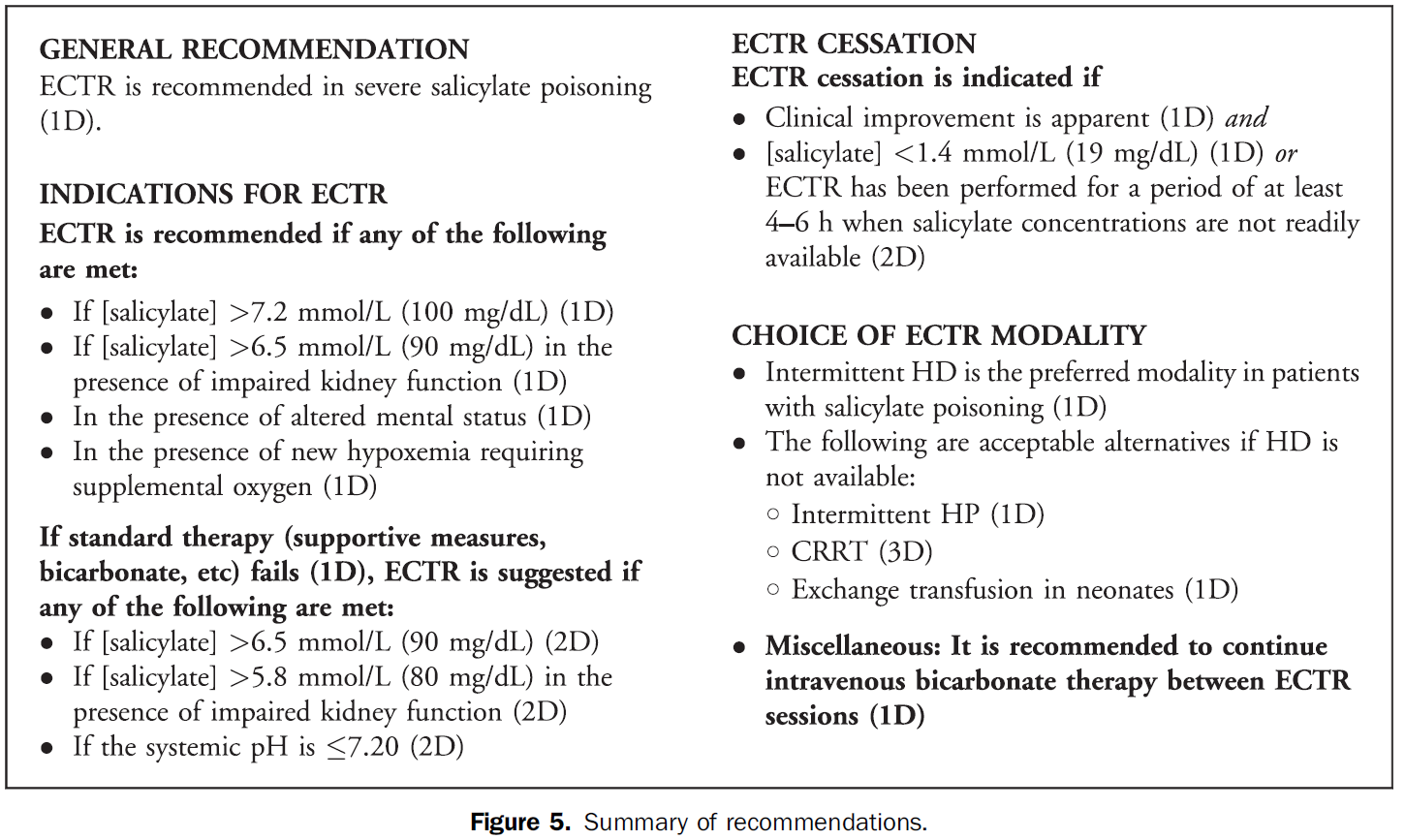
The Extracorporeal Treatments in Poisoning (EXTRIP) Workgroup has published their latest review, this time on extracorporeal treatment for salicylate poisoning. Here are their recommendations on when to dialyze:
Electronic cigarettes are battery-powered devices that deliver nicotine, flavorings, (e.g. fruit, mint, and chocolate), and other chemicals via an inhaled aerosol. E-cigarettes are currently not regulated by the FDA. In many states, there are no restrictions on the sale of e-cigarettes to minors.
Electronic cigarette exposures involving young children are rapidly increasing. Such exposures tend to involve patients aged < 5 years and occur by ingestion of the nicotine-containing liquid. There is a potential for acute nicotine toxicity (nausea, vomiting, pallor, diaphoresis, tachycardia, hypertenstion initially). Respiratory muscle weakness with respiratory arrest is the most likely cause of death.
To date, the overwhelming majority of pediatric ingestions have not resulted in serious medical outcomes. The most commonly reported adverse events were nausea and vomiting.
However, in May of 2014, the first pediatric case of toxicity from ingestion of e-cigarette nicotine liquid was reported. A 10-month old ingested an unknown amount of e-liquid and developed vomiting, tachycardia, grunting respirations, and ataxia. The symptoms resolved by 6 hours after ingestion without specific treatment.
(1) The figure above shows the number of calls to poison centers for cigarette or e-cigarette exposures, by month, in the United States during September 2010 February 2014. E-cigarette exposure calls per month increased from one in September 2010 to 215 in February 2014.
Methemoglobin (MetHb) is produce when Fe+2 in heme is oxidized to Fe+3 under oxidative stress (caused by mediation and chemicals). MetHb does not bind to oxygen and thus decrease RBC’s O2 carrying capacity.
Among medication, overdose of local anesthesia - benzocaine, dapsone, and phenazopyridine are often implicated. (Table 1)
Think about methemoglobinemia in presence of low pulse oximetry (~85%) with lack of response to supplemental oxygen, cyanosis, dyspnea, etc. (see Table 2 – signs and symptoms of MetHb) in patients who are taking or overdosed on medication listed in Table 1.
Diagnosis: CO-oximetry detects toxin-induced hemoglobinopathies, including COHb and MetHb.
Treatment: Methylene blue (1 mg/kg over 5 min) in symptomatic patients or MetHb level > 25%. Resolution of methemoglobinemia should be noted in 30 – 60 min.
G6PD deficiency: Prevalence in the U.S. is 4-7% with highest prevalence in African American population (11%). Methylene blue causes hemolytic anemia in patients with G6PD deficiency within 24 hours of administration. However, G6PD status is often unknown in ED patients. When caring for patients with known G6PD deficiency and methemoglobinemia, providers must carefully consider the risk and benefit of treating MetHb (including severity of poisoning/MetHb) with methylene blue.
Table 1. Causes of MetHb
| Medication
| Chemicals |
| Benzocaine, Lidocaine, Prilocaine | Aniline dye |
| Dapsone | Chlorobenzene |
| Phenazopyridine | Organic nitrites (e.g. isobutyl nitrite) |
| Nitroglycerin | Naphthalene |
| Nitroprusside | Nitrates (well water contamination) |
| Quinones (Primaquine & Chloroquine) | Nitrites (food preservatives) |
| Sulfonamides | Silver nitrate |
| Nitric oxide | Trinitrotoluene |
| Amyl nitrite |
|
Table 2. Signs and symptoms
| MetHb level (%) | Signs and symptoms |
| 1-3% (normal)
| · None |
| 3-15% | · Low pulse oximetry (<90%) · Gray cutaneous coloration |
| 15-20% | · Chocolate brown blood · Cyanosis |
| 20-50% | · Dizziness, syncope · Dyspnea · Weakness · Headache |
| 50-70% | · CNS depression, coma, seizure · Dysrhythmias · Tachypnea · Metabolic acidosis |
| >70% | · Death · Hypoxic injury |
Dabigatran is an orally administered, potent, direct thrombin inhibitor approved for the prevention of stroke and systemic embolism in patients with nonvalvular atrial fibrillation, and for the treatment and secondary prevention of venous thromboembolism.
Several pharmacokinectic studies have suggested that dabigatran possesses a number of ideal properties for expedited removal via extracorporeal methods. Dabigatran has low oral bioavailability (3-7%) and is predominantly cleared (80%) by the kidneys. It is not significantly protein bound, low-to-moderate steady state volume of distribution, and has a low molecular weight. All of these attributes make it a candidate for extracorporeal removal. Low protein binding may suggest redistribution into the plasma post extracorporeal removal.
Dabigatran is a substrate for the multidrug efflux transporter P-glycoprotein. Administration of the drug with potent P-glycoprotein inhibitors (ketoconazole, verapamil, amiodarone, quinidine) may significantly increase risk of toxicity, i.e. bleeding.
Most of the current evidence is based on case reports/case series where HD was the primary mode of removal.
Caution: Redistribution effect in plasma dabigatran concentration was also observed in several cases within 20 min to 12 hours post cessation of renal replacement therapy. Other limitations include:
1) Hemodynamic instability such as hypotension that may make initiation of extracoporeal removal difficult
2) Availability of indicators demonstrating effectiveness of extracorporeal removal
3) Amount of time needed to prepare patient to receive extracorporeal therapy
4) Use of extracorporeal removal as a treatment modality has not been prospectively evaluated
Bottom line: Extracorporeal removal may be an option for patients in the setting of life-threatening bleeding but with consideration of several limitations and should not preclude or delay use of other supplemental hemostatic therapies.
In addition to the down regulation of GABA receptors in chronic ethanol users, there is an upregulation in NMDA receptor subtypes. Although the pathophysiology is much more complex, when ethanol abstinence occurs, there is a shortage of GABA-mediated CNS inhibition and a surplus of glutamate-mediated CNS excitation. If GABA agonists are the mainstay of treatment, why not also target the NMDA receptor? Enter ketamine.
Only one study exists and was published recently.
While the dexmedetomidine studies should not be using reduction in benzodiazepine requirements as an endpoint, it may be acceptable for ketamine since it actually works on the underlying pathophysiology. More studies are needed but it's good to see we’re starting to look at it.
There are some studies that have shown that NSTEMI patients have done worse when administered opioids. Most studies were not well controled and the exact mechanism was not clear. This study adds a biological mechanism to these fidnings.
Hobl et al. showed clopidogre concentrations delayt peak yhours, have overall decrease AUC and actually decrease active metabolites when morphine is administered IV. Morphine may not be the right choice in any ACS that receives clopidogrel.
A new study from South Korea identified 3 potential clinical predictors of developing delirium tremens in patients presenting to the ED with alcohol withdrawal seizures.
If one or more is present, these findings may help assess alcohol withdrawal patients for the risk of developing DTs.
Application to Clinical Practice
Elevation of AST or ALT >1000 after acute ingestion of acetaminophen indicate hepatic toxicity. N-acetylcysteine (NAC) is an effective treatment for acute acetaminophen poisoning. However, in a setting a significant transaminitis, (> 1000s) NAC infusion is continued beyond the routine 21-hour protocol.
Currently, there is no specific guideline or “level” of AST or ALT where discontinuing NAC is deemed safe and appropriate.
A recent retrospective study (n = 37 patients with 343 pairs of AST/ALT) evaluated AST/ALT ratio as a possible indicator for discontinuing NAC infusion after an acute acetaminophen induced hepatic toxicity.
This study found that post peak AST/ALT ratio of < 0.4 had sensitivity of 99% for identifying patients with resolving hepatic injury.
This finding requires validation prior to clinical application but this may be the first step to identifying a safe indicator to help guide clinician when NAC can be discontinued safely.
In the midst of an unprecedented opioid epidemic, there have been considerable efforts to expand access to naloxone (Doyon S, et al. J Med Toxicol 2014;10:431-4). If the situation arises when you need to write a prescription for it, here's how:
Option 1: Naloxone vial and needle traditional IM/SQ using 0.4 mg/mL injection vial and needles (least expensive $40, FDA approved)
Naloxone 0.4 mg/mL single dose vial and 3 cc, 23 g, 1 inch syringes, #2 each
SIG: Inject 1 mL intramuscularly upon signs of opioid overdose. May repeat X 1. Call 911.
Option 2: IMS/Amphastar 2 mg/2 mL prefilled syringe and mucosal atomization device ($95/kit, products FDA approved but intranasal administration is off-label)
Naloxone 2 mg/2 mL prefilled syringe and intranasal atomizer device, #2 each
SIG: Spray one-half of syringe (1 mL) into each nostril upon signs of opioid overdose. May repeat X 1. Call 911.
Option 3: Evzio Autoinjector ($200-700 per Rx though many insurances cover it and the company has vouchers available, FDA approved in 2014, evzio.com/hcp)
Evzio 0.4 mg, #1 two-pack
SIG: Use as directed upon signs of opioid overdose. May repeat X 1. Call 911.
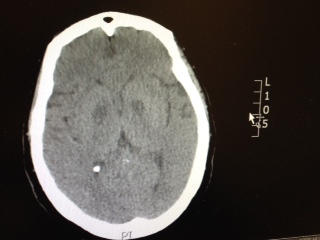
Patient has the following Head CT, what is your differential diagnosis? There are only a few characteristic toxins that can cause this type of finding on CT.
A new review summarized published adverse effects when IV lipid emulsion is used along with venous-arterial extracorporeal membrane oxygenation (VA-ECMO) in patients with cardiotoxic drug poisoning.
Not surprisingly, running fat through the ECMO circuit can cause some issues. Here's what's been published:
It's unclear how these findings should change management if using both treatment modalities, but at the very least, be aware that fat depostion in the VA-ECMO circuits and increased blood clot formation can occur.
| Performance Characteristics of Common Drug Abuse Screening Immunoassays | ||
| Drug/Class | Detection Interval (***) | Comments |
| Amphetamines | 1-2 days (2-4 days) | Decongestants, ephedrine,l-methamphetamine, selegilene & bupropion metabolites may give False (+) results; MDA & MDMA are variably detected |
| Barbiturates | 2-4 days | Phenobarbital may be detected for up to 4 weeks |
| Benzodiazepines | 1-30 days | Benzos vary in reactivityand potency; False (+) results may be seen with oxaprozin |
| Cannabinoids | 1-3 days (>1 month) | Screening assays detect inactive and active cannabinoids; Confirmatory assays detects inactive metabolite THCA (tetrahydrocannabinoic acid) |
| Cocaine | 2 days (1 week) | Screening & confirmatory assays detect inactive metabolite BE (benzoylecgonine); False (+) results are unlikely |
| Opiates | 1-2 days; 2-4 days (<1 week) | Semisynthetic opiates derived from morphine show variable cross-reactivity; Fully synthetic opioids (e.g., fentanyl, meperidine, methadone, propoxyphene, tramadol) have minimal cross reactivity; Quinolone may cross-react |
| Methadone | 1-4 days | Doxylamine may cross-react |
| Phencyclidine | 4-7 days (>1 month) | Dextromethorphan, diphenhydramine, ketamine, & venlafaxine may cross react |
| Propoxyphene | 3-10 days | Duration of positivity depends on cross reactivity of metabolite norpropoxyphene |
(***)Values are after typical use; values in parentheses are after heavy or prolonged use.
Tetrodotoxin is lethal poison that blocks sodium channels. A famous sushi called "Fugu" is cut from a puffer fish that contains this poison. The idea is to get just enough of the toxin to cause peri-oral paresthesia but not too much to get seizures, paralysis and cardiac dysrrhythmias. A recent outbreak in Minneapolis, Minnesota was just reported in the MMWR so it can really happen anywhere, its a great read - dried puffer was bought from a market in NYC.
http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6351a2.htm
2-3 mg of the toxin is lethal to an adult human. No antidote exists though I would try hypertonic sodium bicarbonate for the cardiac dysrrhythmias and appropraite supportive. If the patient survives 24 hrs, the patient will do well without sequelae if appropriately supported.
Hydroxocobalamin is an effective cyanide antidote when administered intravenously. Although intraosseous (IO) access is often used in critically ill patients with difficult or delayed IV access, the efficacy of IO administration has not been investigated until recently.
In a recent randomized animal study, acute cyanide toxicity was induced in two groups of swine where 150 mg/kg Hydroxocobalamin was administered via IV vs. IO. The survival rate, reversal of hypotension, and laboratory results were similar between the IV and IO group.
The finding of this study suggest that IO administration of Hydroxocobalamin is as efficacious as IV administration and its administration in acute cyanide toxicity should not be delayed due to lack of IV access when IO access is available.
Application to Clinical Practice
WBI can facilitate removal of select toxicants from the gastrointestinal tract in some patients, but there is no convincing evidence from clinical studies that it improves the outcome of poisoned patients.
It is believed that administration of beta-blocker administration in patients with cocaine chest pain will produced increased vasoconstriction due to “unopposed alpha effect.”
Several retrospective studies on the use of beta-blocker in patients with cocaine-induced chest pain concluded the use of beta-blocker to be safe.
So is the unopposed alpha effect just a theory?
Lange RA et al. 1990 Ann Internal Med
Design: randomized, double-blind, placebo controlled trial.
30 (38- 68 years old) patients undergoing cardiac catherization for chest pain evaluation were studied.
Cocaine (intranasal administration) resulted in:
Administration of propranolol (intracoronary infusion) resulted in additional:
Complete coronary occlusion observed in 1 patient with ST elevation
Epicardial coronary arterial segment constriction >10% in 5 patients.
Bottom Line: Lange RA et al. 1990 demonstrates that the “unopposed alpha effect” does occur in coronary artery when beta-blocker is administered in a setting of acute cocaine exposure. Overall, the use of beta-blocker in the ED management of cocaine-induce acute chest pain is not a prudent option. It is unknown if the cocaine dose, last use of cocaine (days), or CAD history influence the “safety” of beta-blocker initiation/use during inpatient hospitalization.
Should beta blockers be withheld in cocaine-chest pain patients?
A new study retrospectively compared patients who received beta blockers as an inpatient to those who did not. Even though the beta blocker group had higher risk clinical characteristics, there was no difference in the composite primary end point of myocardial infarction, stroke, ventricular arrhythmia, or all-cause mortality within 24 hours of beta blocker use.
Important Limitations
The potentially dangerous interaction between beta blockers and cocaine is likely a much larger issue in patients with very recent cocaine use in the setting of a catecholamine surge. A retrospective analysis likely doesn't include those patients.
Application to Clinical Practice
While this study doesn't answer the question about beta blocker use in acute cocaine toxicity, it does provide some reassurance about the safety of beta blockers given for cocaine-related chest pain.
Sympathomimetic toxicity is a known toxidrome that is complicated by the development of rhabdomyolysis. There are multiple stimulant agents that induce sympathomimetic toxicity including, synthetic cathinones, cocaine, amphetamines, and methamphetamines.
A recent retrospective, single-center, chart review in the age range of 14-65 years sought to determine the prevalence of rhabdomyolysis in patients with sympathomimetic toxicity and compare rates among patients using specific agents. Rhabdomyolysis and severe rhabdomyolysis were defined as CK>1000 and 10,000 IU/L, respectively.
Rhabdomyolysis occurred in 42% of study subjects (43/102)
Prevalence in 89 subjects due to a single-stimulant exposure:
Rhabdomyolysis
1) Synthetic cathinone (MDPV, alpha-PVP) 63% (12/19)
2) Methamphetamine 40% (22/55)
3) Cocaine 33% (3/9)
4) Other single agents (methylphenidate, pseudoephedrine, phentermine) 0% (0/6)
Severe Rhabdomyolysis
1) Synthetic cathinone 26% (5/19)
2) Methamphetamine 3.6% (2/55)
3) Cocaine 11% (1/9)
4) Other single agents (methylphenidate, pseudoephedrine, phentermine) 0% (0/6)
In this study, patients exposed to synthetic cathinones were more likely to develop rhabdomyolysis and severe rhabdomyolysis compared to the non-cathinone-exposed group.
Bottom Line:
Be aware of this increased risk from synthetic cathinones along with other stimulants. Treat aggressively with IV fluids, rapid correction of hyperthermia, benzodiazepines to control manifestations of sympathomimetic toxicity to reduce muscle activity and metabolic demand.