The cross-reactivity between cephalosporins and penicillins is significantly lower than the 10% figure many of us learned. In fact, the beta-lactam ring is rarely involved. So, when the warning pops up next time you order ceftriaxone in a penicillin-allergic patient, what should you do?
In a patient with a documented penicillin allergy, here is a simple chart to help determine when a cephalosporin is ok to use:
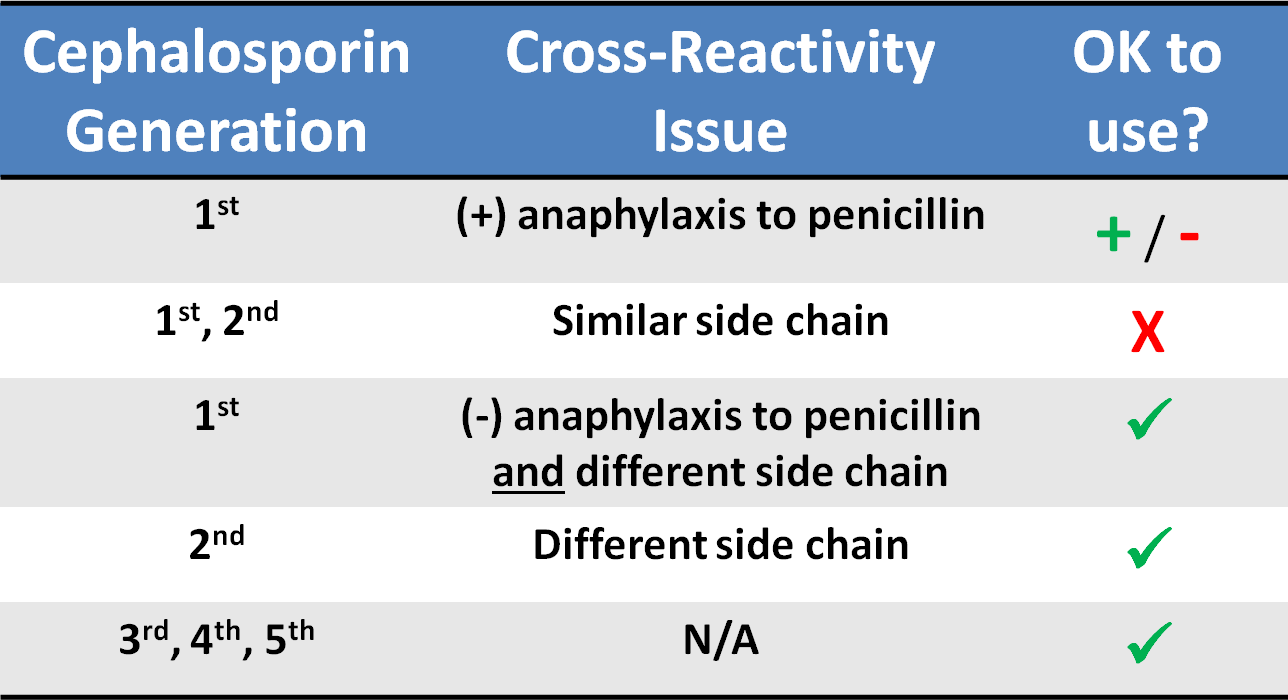
Common penicillins and cephalosporins with similar side chains include ampicillin/amoxicillin and cephalexin, cefaclor, cephadroxil, and cefprozil.
Beta-lactam antimicrobials (penicillins, cephalosporins, and carbapenems) are frequently used for empiric and targeted therapy in critically ill patients. They display time-dependent killing, meaning the time the antibiotic concentration is above the minimin inhibitory concentration (MIC) is associated with improved efficacy.
Two new pharmacodynamic/pharmacokinetic studies suggest that current beta-lactam antimicrobial dosing regimens may be inadequate.
Antimicrobial dosing in critically ill patients is complex. Current dosing of beta-lactams may be inadequate and needs to be studied further with relation to clinical outcomes.
In May 2014, the U.S. Public Health Service released the first comprehensive clinical practice guidelines for PrEP.
Pre-Exposure Prophylaxis (PrEP) has been shown to decrease the risk of HIV infection in people who are at high risk by up to 92%, if taken consistently.
How this applies to the ED patient:
For more information, the CDC has a comprehensive website dedicated to PrEP.
Despite the lack of strong evidence to support the recommendation, the severity of the 2009 influenza pandemic prompted the World Health Organization (WHO) to advise that higher doses of oseltamivir (150 mg twice daily) and longer treatment regimens (> 5 days) should be considered when treating severe or progressive illness.
So, does the data support higher dosing in critically ill influenza patients?
A new systematic review concluded that "the small body of literature available in humans does not support routine use of high-dose oseltamivir in critically ill patients."
Clindamycin used to be a first-line agent for many SSTIs, particularly where MRSA was suspected. With growing resistance to staph species, the 2014 IDSA Guidelines recommend clindamycin as an option only in the following situations:
* Clindamycin may be used if clindamycin resistance is <10-15% at the institution.
In a prospective cohort of 598 ED patients, 5 risk factors were independently associated with uncomplicated cellulitis patients who fail initial antibiotic therapy as outpatients and require a change of antibiotics or admission to hospital:
Patients presenting with uncomplicated cellulitis and any of these risk factors may need to be considered for observation +/- IV antibiotics.
Four small case series (one prospective, 3 retrospective) have concluded that dexmedetomidine (Precedex) may be a useful adjunct therapy to benzodiazepines for ethanol withdrawal in the ED or ICU. They are summarized on the Academic Life in EM blog.
A new randomized, double-blind trial evaluated 24 ICU patients with severe ethanol withdrawal.
Group 1: Lorazepam + placebo
Group 2: Lorazepam + dexmedetomidine (doses of 0.4 mcg/kg/hr and 1.2 mcg/kg/hr).
Acetaminophen spent much of 2013 being chased by paparazzi and sharing magazine covers with Miley Cyrus. What a fall from stardom after becoming known as the pain reliever “hospitals use most,” and the one, “recommended by pediatricians.” Slogans we know well based on $100 million/year spent on advertising.
Approximately 150 patients a year die from unintentional acetaminophen poisoning averaged over the past 10 years. From 2001 to 2010, annual acetaminophen-related deaths amounted to about twice the number attributed to all other over-the-counter pain relievers combined,
The FDA sets the maximum recommended daily dose of acetaminophen at 4 grams, or eight extra strength acetaminophen tablets.
Ingestion of 150 mg/kg or approximately 10g for a 70 mg individual reaches the toxic threshold for a single ingestion. The toxic threshold decreases in cases of chronic ingestion.
Patients who “unintentionally” overdose have been found to take just over 8g per day (almost double the recommended maximum). This is unlikely due to taking one extra 325mg tablet once or twice.
Before we all go on a mad NSAID prescribing binge, let's all be aware of the dangers, educate our patients and allow Acetaminophen to walk the red carpet again.
A new study of almost 2 million prescriptions in VA patients compared the risk of cardiovascular death or dysrhythmia in patients receiving azithromcyin, levofloxacin, and amoxicillin.
What they found
Compared with amoxicillin, azithromycin was associated with a significant increase in mortality (HR = 1.48; 95% CI, 1.05-2.09) and dysrhythmia risk (HR = 1.77; 95% CI, 1.20-2.62) on days 1 to 5, but not 6 to 10.
Levofloxacin was associated with an increased risk throughout the 10-day period. Days 1-5 mortality (HR = 2.49, 95% CI, 1.7-3.64) and serious cardiac dysrhythmia (HR = 2.43, 95% CI, 1.56-3.79). Days 6-10 mortality (HR = 1.95, 95% CI, 1.32-2.88) and dysrhythmia (HR = 1.75; 95% CI, 1.09-2.82).
Important limitations
This study did not have a comparator group of patients getting no antibiotics. Previous data suggest patients on any antibiotic (eg, penicillin) have a higher risk of death or dysrhythmia.
The supplemental index shows that patients receiving azithromycin and levofloxacin had more serious infections (eg, PNA, COPD, etc.) which may have put them at higher risk for worse outcome irrespective of antibiotic choice.
What it means
It seems azithromycin and levofloxacin may contribute to a small increase in cardiovascular mortality and dysrhythmia during their use. A previous study found this is more likely in those with existing cardiovascular disease.
Aseptic meningitis is meningitis with negative bacterial cultures. Overall, viral infections are the most common etiology, however medications can also cause this illness.
Well known causes of aseptic meningitis include: antimicrobials (particularly sulfamethoxazole/trimethoprim), NSAIDS, antivirals (valacyclovir), and antiepileptics.
Recently an abstract was published that suggests that patients on levetiracetam have a higher risk of developing aseptic meningitis than those on topiramate and gabapentin. Lamotrigine has also been implicated, but appears to have a lower risk than levetiracetam, topiramate and gabapentin.
Background
The ACLS recommendation for epinephrine dosing in most cardiac arrest cases is 1 mg every 3-5 minutes. This dosing interval is largely based on expert opinion.
Primary Outcome
A new study reviewed 21,000 in-hospital cardiac arrest (IHCA) cases from the Get With the Guidelines-Resuscitation registry. The authors sought to examine the association between epinephrine dosing period and survival to hospital discharge in adults with an IHCA.
Methods
This pattern was consistent for both shockable and non-shockable cardiac arrest rhythms.
Tranexamic Acid (TXA) topically applied was compared to anterior nasal packing in 216 patients with acute anterior epistaxis. Cotton pledgets (15 cm) soaked in injectable TXA (500 mg/5 ml) were inserted into the bleeding nostril and removed after bleeding had arrested. This was compared to standard anterior packing.
RESULTS
| TXA Anterior packing |
| % pts bleeding stopped in 10 min: 71% 31.2% |
| Discharge after 2 hours 95.3% 6.4% |
| Rebleeding in 24 h hours 4.7% 11% |
| Satisfaction scores 8.5 4.4 |
Bottom line: topical tranexamic acid looks promising for control of uncomplicated anterior epistaxis.
In most situations (dependant on state laws and institutional policies), methadone-maintained patients enrolled in a drug abuse program are best managed by continuing methadone at the usual maintenance levels with once-a-day oral administration.
Pearl: In the event the methadone clinic is closed and/or the dose cannot be verified, 30-40 mg (10-20 mg IM) is generally enough to prevent withdrawal in most patients.
This is only a short-term measure and some patients may require additional methadone. Full doses of methadone should be reinstituted as soon as possible.
46 patients treated with high-dose droperidol (10-40 mg) were studied prospectively with continuous holter recording.
What they did
Patients initially received 10 mg droperidol as part of a standardized sedation protocol (for aggression). An additional 10 mg dose was given after 15 min if required and further doses at the clinical toxicologist's discretion.
Continuous 12-lead holter recordings were obtained for 2-24 hours. QTc > 500 msec was defined as abnormal (with heart rate correction - QTcF).
What they found
Only 4 patients had abnormal QT measurements, three given 10 mg and one 20 mg. All 4 had other reasons for QT prolongation. No patient given > 30 mg had a prolonged QT. There were no dysrhythmias.
What it means
There was little evidence supporting droperidol being the cause and QT prolongation was more likely due to pre-existing conditions or other drugs.
Tranexamic acid (TXA) is an antifibrinolytic that prevents clot breakdown by inhibiting plasminogen activation and plasmin activity
The CRASH-2 trial enrolled 20,211 adult trauma patients with significant hemorrhage (SBP <90 or HR 110) or at significant risk of hemorrhage
Patients were randomized to 1 gram TXA over 10 minutes followed by an infusion of 1 gm over 8 hours vs placebo
There was a significant reduction in the relative risk off all cause mortality of 9% (14.5% vs 16%, RR 0.91, CI 0.85-0.97, p = 0.0035)
The patients that benefited most were those most severely injured, and in those treated in less than 3 hours of injury.
JNC8 (the Eigth Joint National Commission) released their recommendations for blood pressure management this week. The full article as published in JAMA can be found at http://jama.jamanetwork.com/article.aspx?articleid=1791497
Highlights from this report are
General Pearl: Remember to be cautious in acutely lowering the blood pressure in asymptomatic patients. Acute lowerings can cause watershed ischemia leading to strokes.
In a potentially ground breaking study of healthcare-associated pneumonia (HCAP) patients, atypical pathogens were identified in 10% of cases!
Application to clinical practice: Add atypical coverage with a macrolide or respiratory fluoroquinolone for HCAP patients who have been in the community for any length of time.
The study also identified HCAP patients who may not require 3 'big gun' broad-spectrum antibiotics. This is a practice changing article for ED providers. For more analysis of the study, please note the bonus reading links below.
Bonus reading:
Dr. Emily Heil (@emilylheil) analyzes the full study in more depth at Academic Life in Emergency Medicine: http://academiclifeinem.com/new-treatment-strategy-not-so-sick-health-care-associated-pneumonia/
Dr. Ryan Radecki (@emlitofnote) critiques the study at Emergency Medicine Literature of Note: http://www.emlitofnote.com/2013/10/down-titrating-antibiotics-for-hcap.html
It has linear, predictable pharmacokinetics, achieves maximal concentration within 1-2 hours, is 50% renally excreted, and has a half life is 9-11 hours.
Edoxaban was evaluated in a recent trial comparing warfarin in patients with atrial fibrillation.
The primary end point or first stroke or systemic pulmonary embolic event occurred in 1.5% with warfarin, compared with 1.18% in the high dose edoxaban (HR 0.79; 97.5% CI 0.63-0.99, P<0.001). In the intention to treat there were trends favoring high dose edoxaban and unfavorable trends with the lower dose.
The principal safety end point of major bleeding occurred in 3.43% with warfarin versus 2.75% with high dose edoxaban (HR 0.86; 95% CI 0.71-0.91, P<0.001).
Bottom line: Both high dose (60 mg) and low dose (30 mg) edoxaban were non-inferior to warfarin with prevention of stroke or systemic emboli, and were associated with significantly lower rates of bleeding and death from cardiovascular causes.
Currently it is approved for use in Japan.
When patients with severe allergies to penicillin (urticarial, bronchospasm, anaphylaxis, angioedema) are excluded, the cross reactivity to cephalosporins is very low (approximately 0.1%)
The reaction is related to structures in the side chain, not the cyclical structure as thought in the past.
There are several cephalosporins with IDENTICAL side chains that should not be given to patients with allergies to specific penicillins, namely: