Up until recently, a tight-fitting mask was one of the only ways to deliver non-invasive positive-pressure ventilation.
High-flow nasal cannulas (HFNC) have been adapted from use in neonates to adults to deliver continuous positive airway pressure (CPAP).
HFNC provides continuous, high-flow (up to 60 liters), and humidified-oxygen via nasal cannula providing positive pressure to the pharynx and hypopharynx. Patients tolerate it well and it is less claustrophobic than tight-fitting masks.
HFNC does not generate the same amount of pressure as CPAP so it may be best utilized as an intermediate step between low-flow oxygen (i.e., traditional nasal cannula) and non-invasive positive pressure ventilation with tight-fitting masks.
Check with your respiratory department if these devices are locally available.
9 year-old boy with sudden onset of unilateral facial swelling. What’s the diagnosis?

Determining the exact etiology of hypotension / shock can sometimes be difficult in the Emergency Department.
The Rapid Ultrasound for Shock / Hypotension (RUSH) exam is a sequential, 5 step-protocol (typically requiring less than 2 minutes) that can be used to determine the cause(s) of hypotension.
The mnemonic for the exam is “HI MAP”, and is easy to remember because a "HI MAP" is our goal with hypotensive patients.
H - Heart (parasternal and four-chamber views)
I - Inferior Vena Cava (for volume responsiveness)
M - Morrison’s pouch (i.e., FAST exam) and views of thorax (looking for free fluid)
A - Aortic Aneurysm (ruptured abdominal aneurysm)
P - Pneumothorax (i.e., Tension PTX)
Refer to the link for a more detailed discussion and podcast from the creators of this exam: emcrit.org/rush-exam
Positive-pressure ventilation (e.g., mechanical ventilation) increases intrathoracic pressure potentially reducing venous return, right-ventricular filling, and cardiac output.
Pericardial tamponade similarly causes hemodynamic compromise through increased pericardial pressure which reduces right-ventricular filling and cardiac output.
When mechanically ventilating a patient with known or suspected pericardial tamponade the mechanisms above may be additive, causing cardiovascular collapse and possibly PEA arrest.
For the patient with known or suspected pericardial tamponade consider draining the pericardial effusion prior to intubation or delaying intubation until absolutely necessary.
If intubation is unavoidable, consider maintaining the intrathoracic pressure as low as possible (by keeping the PEEP and tidal volumes to a minimum) to ensure adequate cardiac filling and cardiac output.
72 year-old man, one-week post right fem-pop bypass presents with painful blue and black toe. Diagnosis?

On October 25, 2011, Eli Lilly announced a voluntary-recall of activated drotrecogin alfa (Xigris) following a recent trial (PROWESS-SHOCK), which demonstrated no survival benefit when using the drug when compared to placebo.
Activated drotrecogin alfa is a recombinant form of human activated protein C previously recommended for adults with severe sepsis and a high-risk of death (APACHE II > 25 or multi-organ failure); it is included in the 2008 International Sepsis Guidelines (Grade 2b recommendation).
The PROWESS-SHOCK trial reported an all-cause mortality rate of 26.4% in the drotrecogin alfa group compared with 24.2% in the placebo group; this difference was not statistically significant.
Interestingly, the study also found that severe bleeding (the drug's main side-effect) was found to be 1.2% in the activated drotrecogin alfa group compared to 1.0% for the placebo group (also non-significant) suggesting it does not increase the risk of bleeding as it had previously been reported.
Hospitals should revise their sepsis guidelines based on this recent news.
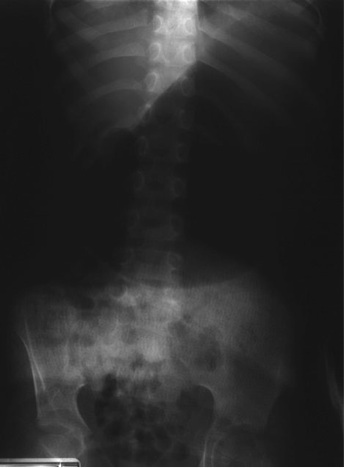
5 year-old male with developmental delay presents with intractable non-bloody and non-bilious vomiting over 10 days; bowel movements are normal. Four weeks ago he was placed in a hip-spica cast following a motor vehicle crash. Abdominal x-ray is below. Diagnosis?
Lisiteria Monocytogenes is typically transmitted from ingestion of contaminated food such as unpasteurized milk or cheese, raw foods, and recently cantaloupes; transmission from veterinary exposure, infected soil and water have also been reported.
Listeria has a predilection for the central nervous system (CNS) causing several infections including meningioencephalitits, brain or spinal abscess, cerebritis (infection of brain parenchyma), and rhomboencephalitis (encephalitis of the brainstem).
Risk factors include immunosuppression, advanced age, newborns, and pregnancy.
There is no clinical way to distinguish CNS infection with Listeria from other pathogens, therefore blood and cerebrospinal fluid (CSF) culture is required.
CSF analysis demonstrates pleocytosis, elevated protein, and low glucose. CSF gram stain has a low sensitivity (~33%), but consider Listeria in the differential if "diptheroid-like" bacteria are reported on gram stain.
Ampicillin is the drug of choice and should be continued for at least three weeks (sometimes longer). Adding gentamycin is sometimes recommended for synergy in severe infection.
Question: 50-year-old diabetic female s/p foot burn several weeks ago, now presenting with pain and discharge from a poorly healing wound. Diagnosis?

· The use of epinephrine in cardiac arrest is currently standard of care.
· Several observational and non-randomized trials have demonstrated the efficacy of epinephrine in cardiac arrest, but there has never been a randomized double-blind placebo-controlled trial in humans.
· A recently published Australian trial randomized cardiac patients (of any type) to receive either 1 mg of epinephrine (n=272) or 0.9% normal saline (n=262); the primary end-point was survival to hospital discharge. Secondary end-points were pre-hospital return of spontaneous circulation (ROSC) and neurological outcomes at hospital discharge.
· Significantly more patients had pre-hospital ROSC in the epinephrine group (regardless of the underlying rhythm), however, there was no statistically significant difference in survival to discharge (the primary outcome) between groups.
· This randomized double-blinded placebo-controlled trial raises many new and interesting questions about epinephrine, but more study is needed before changing current practice.
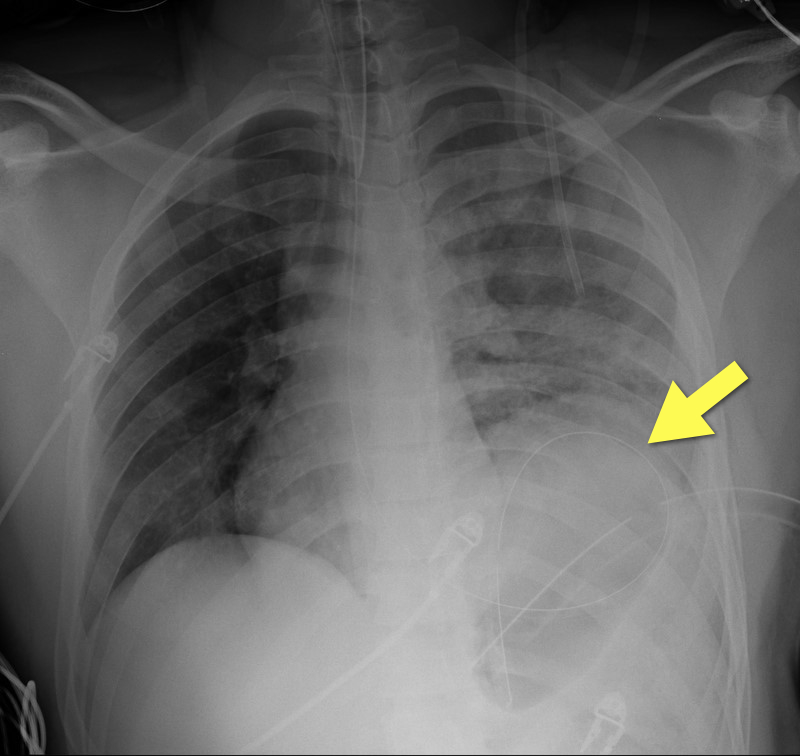
19 year-old male s/p high-speed MVC with hypotension and diminished breath sounds on left. Diagnosis?
Radial and femoral arteries are common sites for arterial-line placement, but are not without complications (e.g., Radial artery: malfunction with positioning and Femoral artery: contamination and infection); an alternative site to consider is the axillary artery.
The axillary artery's superficial location and large size make it a desirable choice for cannulation.
The "anatomical-landmark" and "palpation" methods have been the traditional techniques of axillary arterial cannulation, however these methods may be difficult for to a variety of reasons (e.g., obesity, anasarca, arterial disease, etc.)
Ultrasound allows visualization of the axillary artery and avoids unintended injury to structures in close proximity (e.g., brachial plexus, pleura, axillary vein, etc.); please see figures 1 and 2 in the referenced Sandhu article and http://www.youtube.com/watch?v=Z31YiyV7cNQ.
A recent study (Killu, 2011) found that ultrasound increases success rates when compared to the traditional landmark approach.
Multiple methods of confirming endotracheal tube placement exist, however quantitative waveform capnography is the most reliable method. Unfortunately this may not be immediately available at all medical centers.
Recent studies demonstrate that bedside ultrasound may assist in the detection of proper endotracheal tube placement.
The T.R.U.E. (Tracheal Rapid Ultrasound Exam) was demonstrated to be 99% sensitive, 94% specific, 99% PPV, and 94% NPV during intubation.
The basic exam involves placing a high-frequency linear-array probe on the anterior neck above the sternal notch and identifying the trachea and esophagus during intubation.
The following video is an example of what you DO NOT want to see during an intubation: http://www.youtube.com/watch?v=LvfThxhQ93A
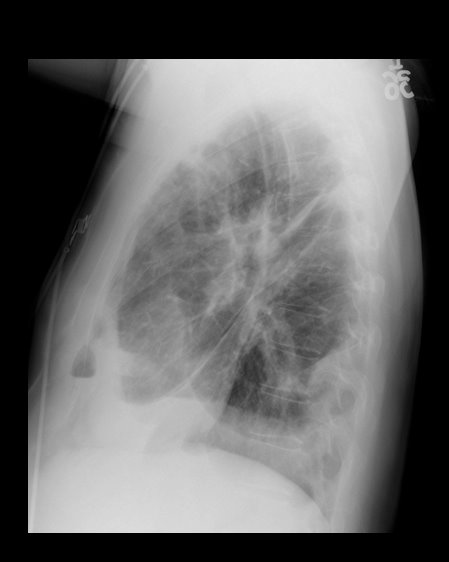
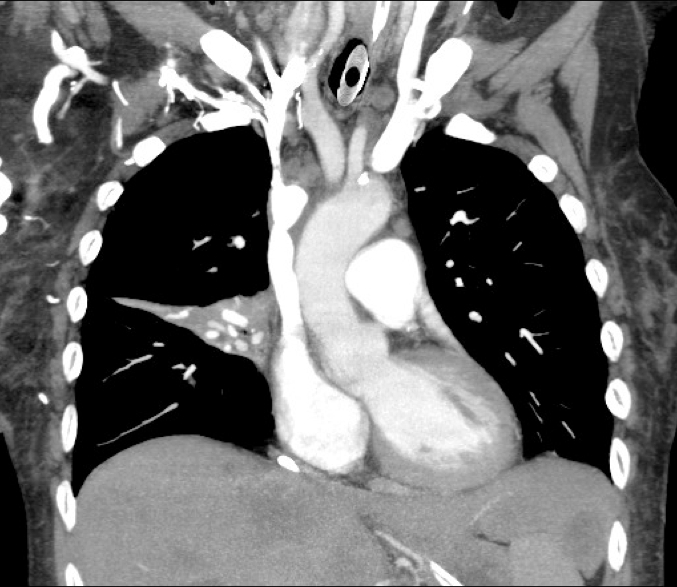
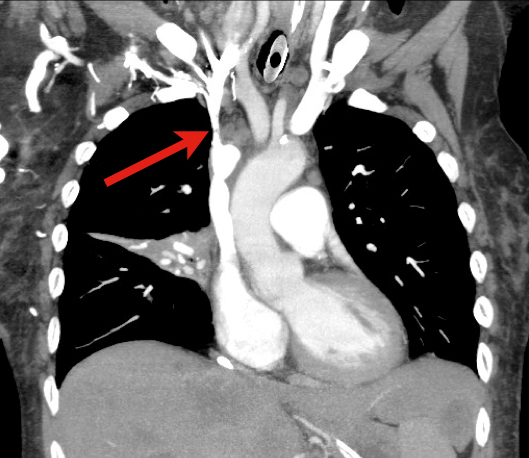
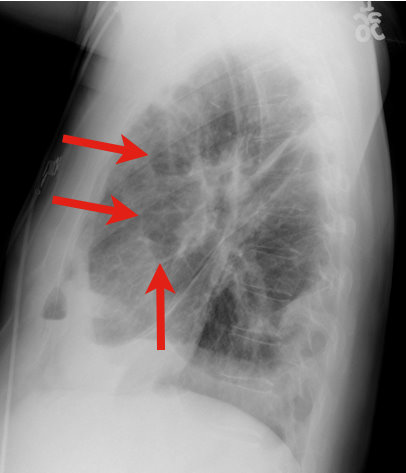
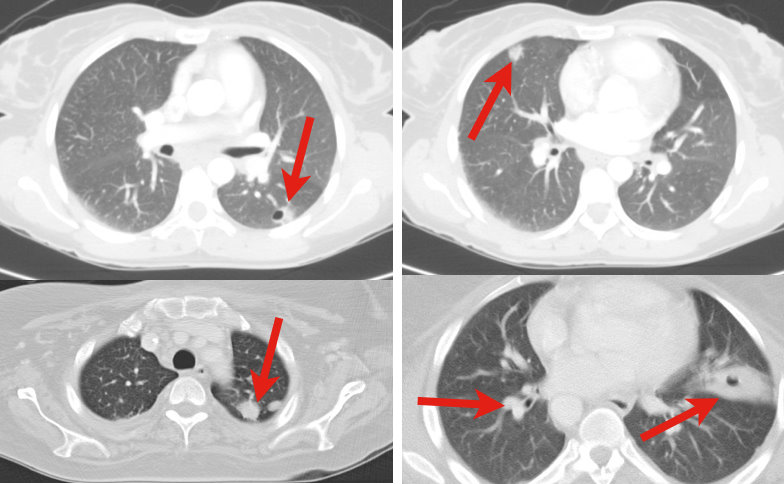
79 y.o. male lung cancer patient with tachypnea, tachycardia, and normal blood pressure. Click here: http://vimeo.com/27973006
Possible diagnosis?
The open cricothyrotomy technique is taught as the trauma airway standard when one “cannot intubate and cannot ventilate” however, it is not without difficulty and limitations. The B.A.C.T. (Bougie-Assisted Cricothyrotomy Technique) may improve the procedure by using a bougie to assist.
Steps for the B.A.C.T. (as described in the paper):
1. Stabilize the larynx with the thumb and middle finger, then identify the cricothyroid membrane.
2. Make a transverse stabbing incision with a scalpel through both skin and cricothyroid membrane.
3. Insert tracheal hook at the inferior margin of the incision and pull up on the trachea.
4. Insert a bougie through the incision with curved tip directed towards the feet
5. Pass 6-0 endotracheal tube or Shiley over bougie into trachea.
Advantages of a bougie:
1. Thin and easy to insert into incision
2. Tactile feedback from tracheal rings confirms proper placement
3. Ensures that stoma will not be lost during procedure
EMRAP.tv has a great video of Dr. Darren Braude demonstrating the procedure;
http://bit.ly/nB3BMG
13 year-old right-hand dominant male following assault with blunt object. Diagnosis?


Pregnancy causes many physiologic changes, which may be challenging during trauma resuscitations. A few pearls on the ABC’s:
Airway
Breathing
Circulation
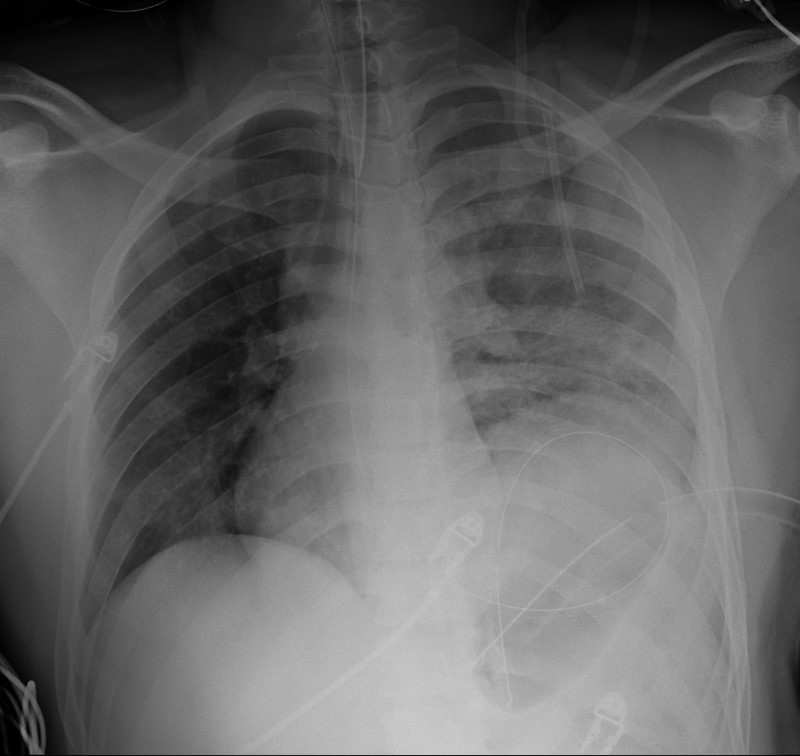
34 y.o. male with history of IVDA (intravenous drug abuse) complains of fever, chills and cough. Diagnosis?