Do you like placing ultrasound-guided IV catheters? Check out this trick for covering the probe during the procedure.
http://ultrarounds.com/Ultrarounds/The_Vascular_Probe_Protector.html
or
https://www.youtube.com/watch?v=ZuOq6Ea_FbA&feature=plcp
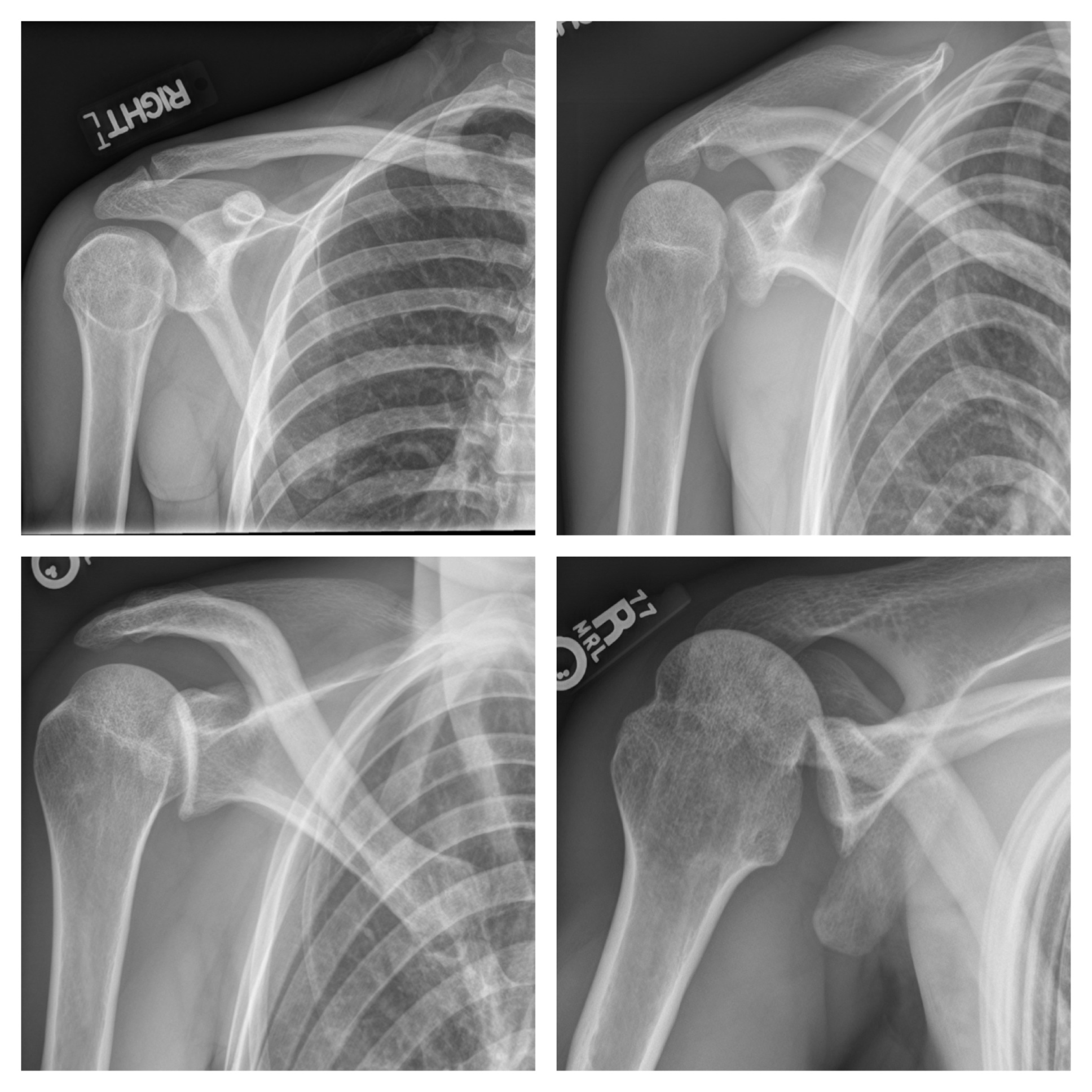
33 year-old male found unconscious by EMS and complains of right shoulder pain upon waking up in the ED. Diagnosis?
Previous pearls have described the increasing evidence against colloid (e.g., hydroxyethyl starch) use during resuscitation. Now it appears that the crystalloid 0.9% normal saline (NS) may be under fire.
The use of large volumes of NS has been associated with hyperchloremic metabolic acidosis and harm in animal studies. The risk of harm in humans, however, has been less clear.
Bellomo et al. conducted a prospective observational study in which patients being resuscitated in the control group received NS at the clinicians' discretion; i.e., chloride-liberal strategy. The use of NS was restricted in the intervention group, where other less chloride containing fluids were used for resuscitation (e.g., Ringer's Lactate); i.e., a chloride-restrictive strategy.
The authors found that when compared to patients in the chloride-liberal group, the chloride-restrictive group had significantly less rise in baseline creatinine, less overall AKI, and a reduced need for renal replacement therapy.
Bottom line: Although this was only an observational study, the liberal use of normal saline during resuscitation may increase the risk of AKI and renal replacement therapy.
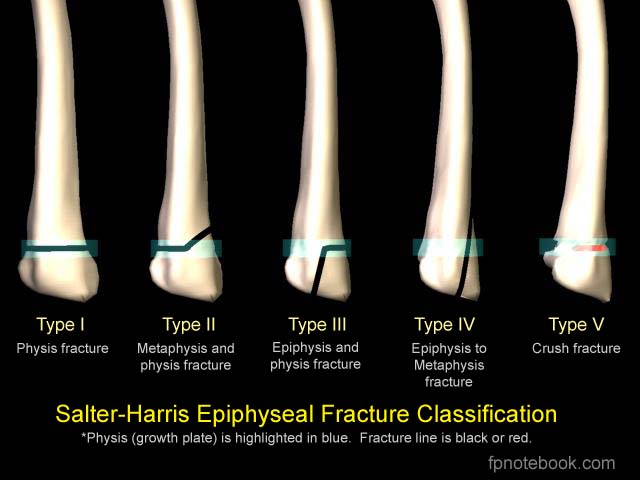
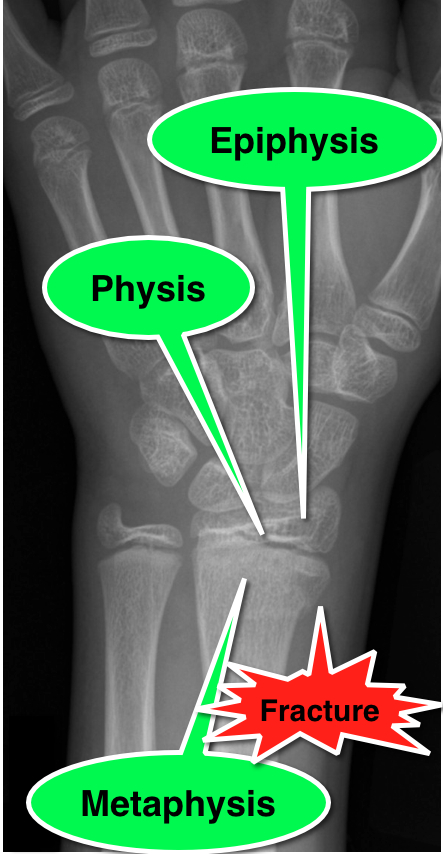
11 year-old male is tackled and falls on his outstretched hand while playing football. X-rays are shown below. What's the diagnosis?

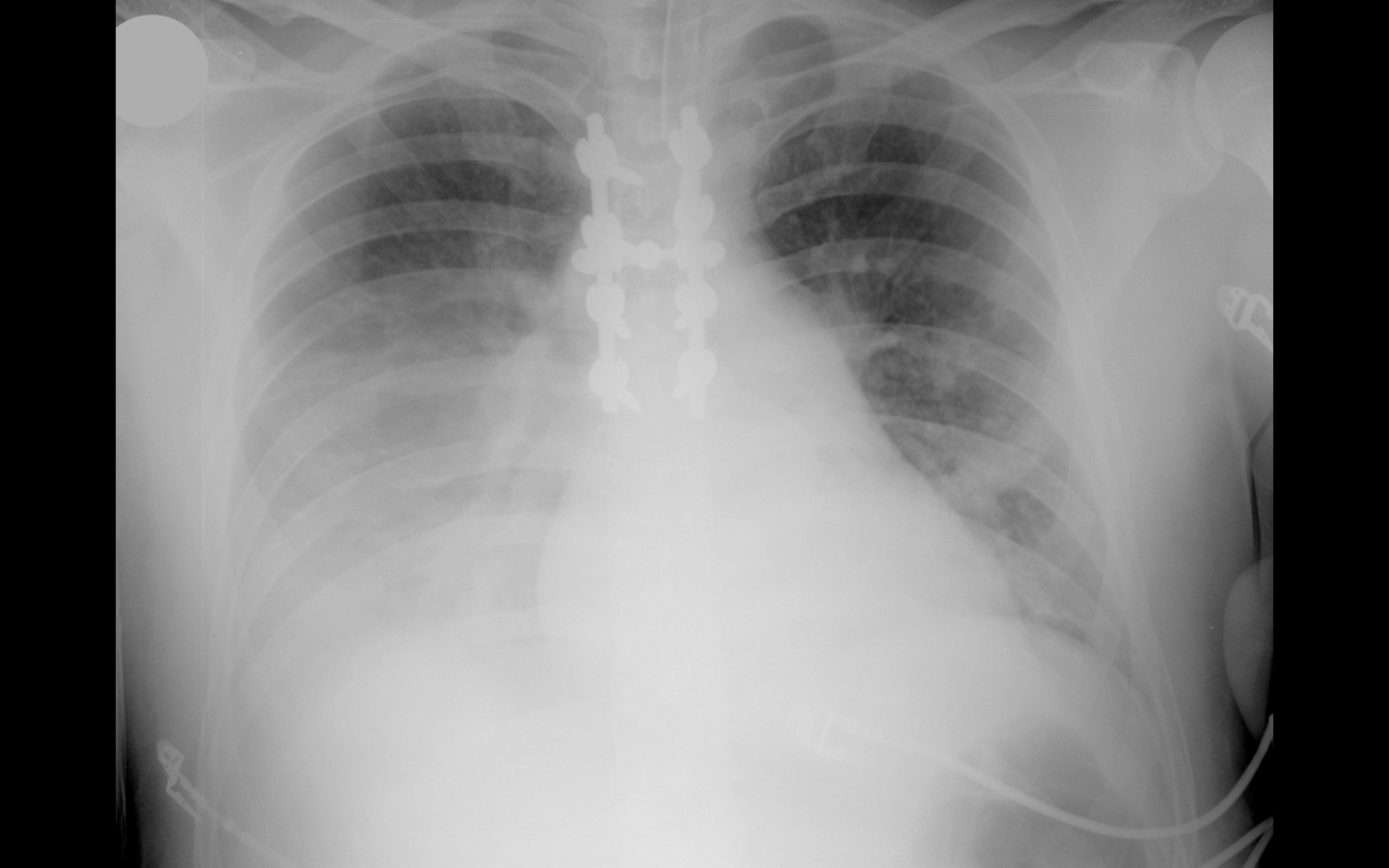
33 year-old male in respiratory distress. What's the diagnosis?
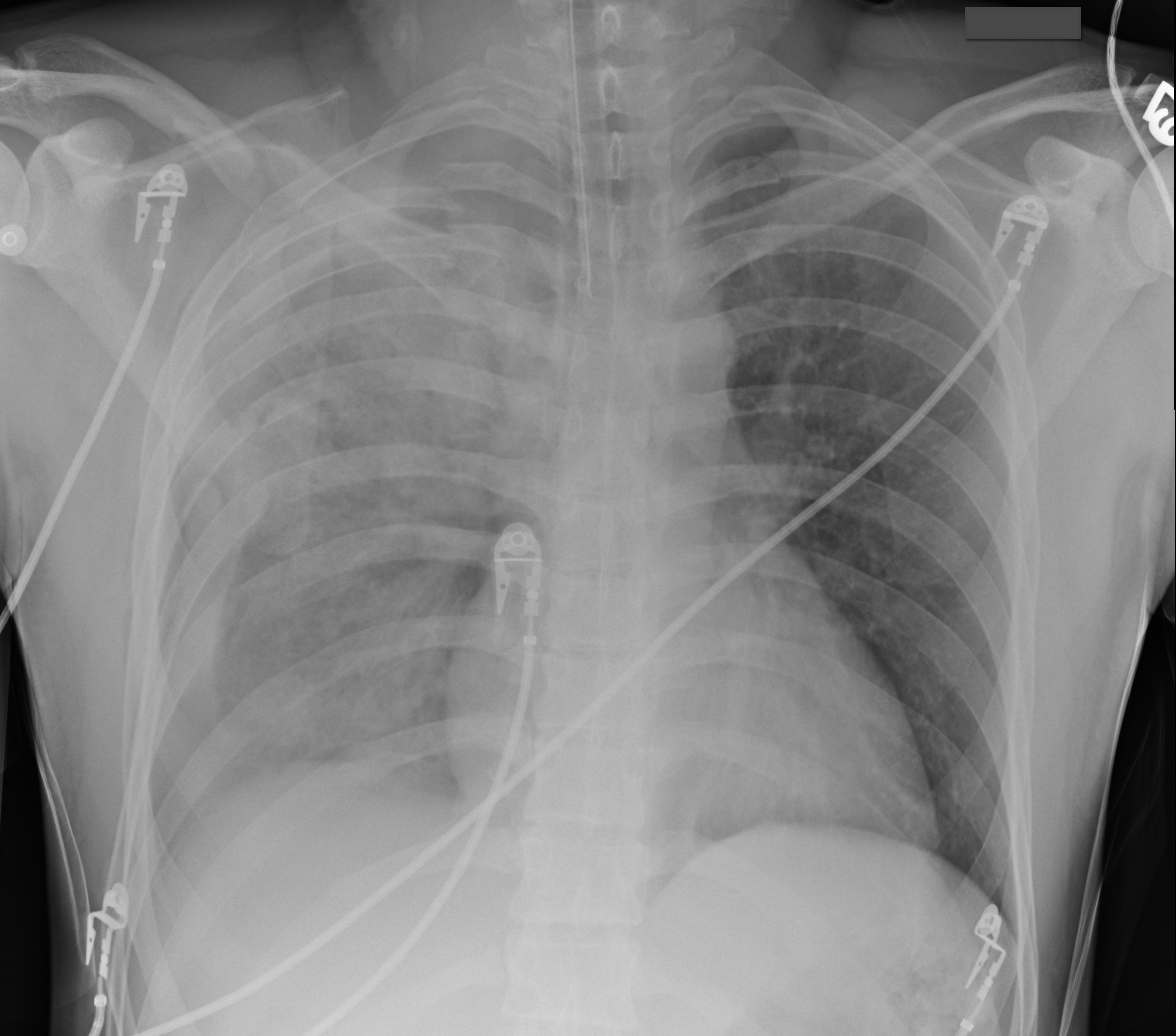
Trauma patient (...yes, that's the only history you're given). Diagnosis?
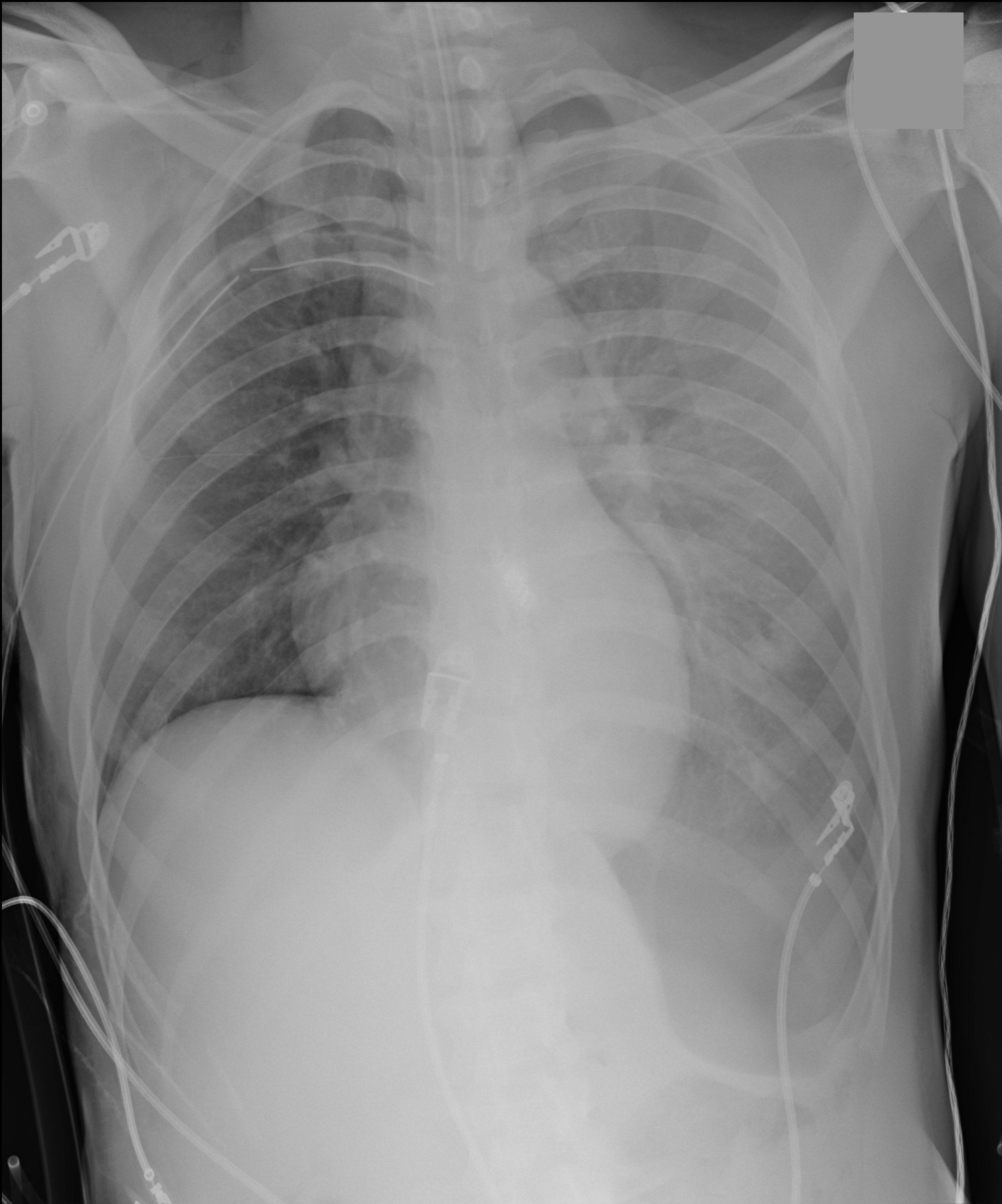
35 year-old male unrestrained driver following motor vehicle crash presents with blunt chest injury. There are multiple injuries on CXR (can you find them all?), but what's up with his right lung?
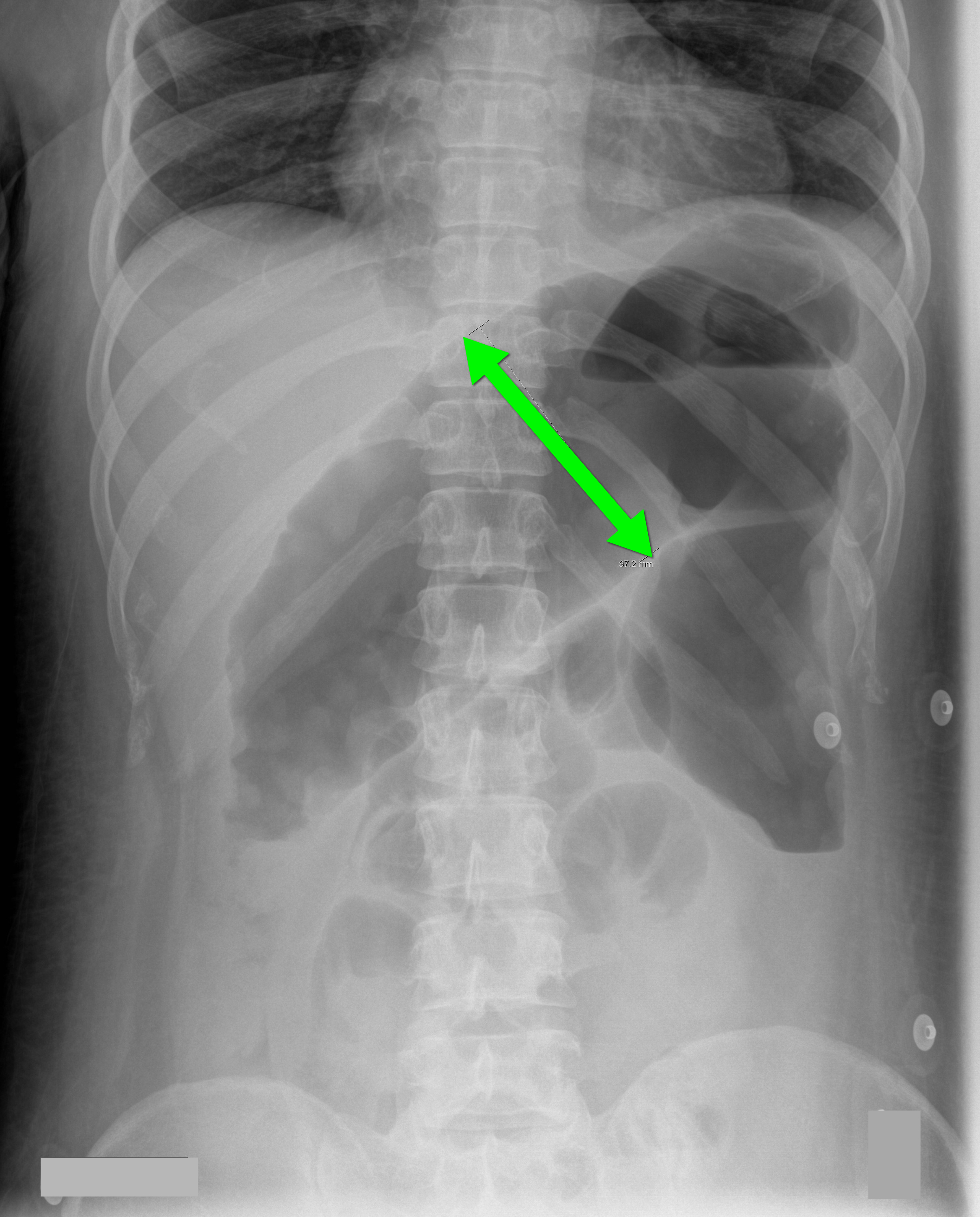
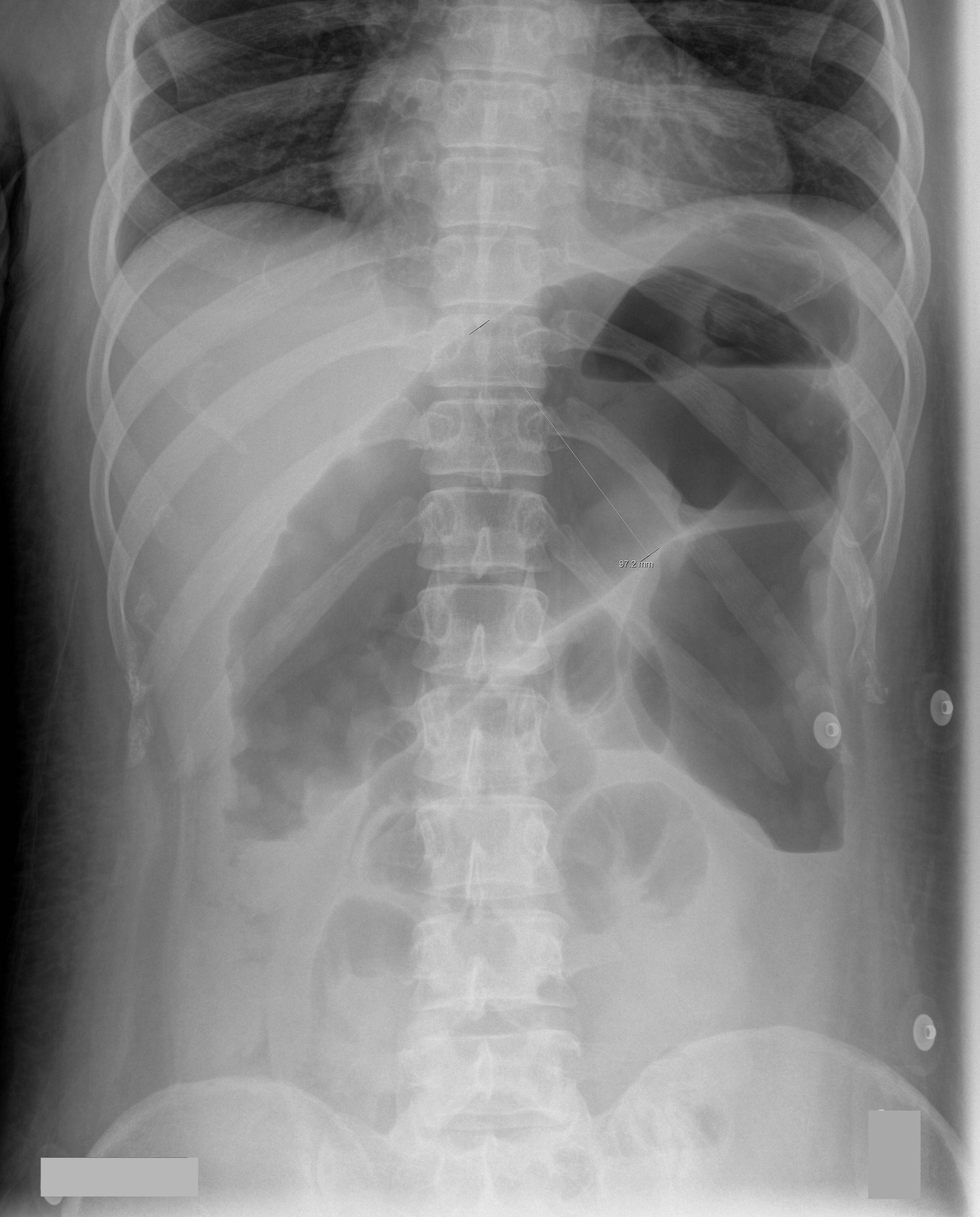
70 year-old male recently treated for community-acquired pneumonia presents with bloody diarrhea, fever, and severe abdominal pain. Abdominal Xray is shown below. Diagnosis?
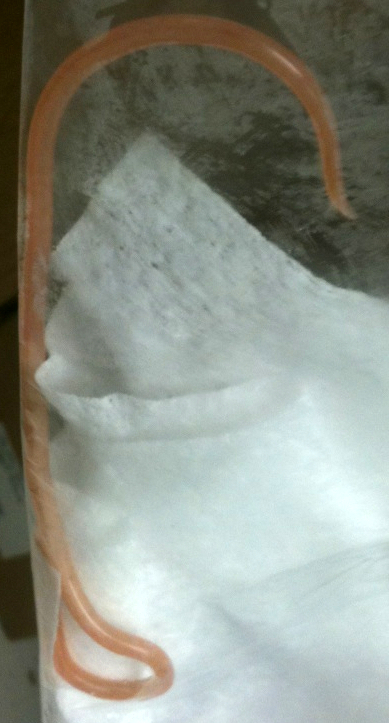
26 year-old male from Indonesia presents with severe abdominal pain and weight loss for the past two months. He also states he found this "worm" in the toilet (see below) after a bowel movement. What is the medical treatment for this condition?
Do you place central-lines?
Do you suture your central-lines into place?
Do you ever get worried that you are going to stick yourself with that needle?
If you answered yes to any of these questions, then maybe this pearl is for you; click here
Intubated patients may occasionally meet certain criteria for extubation while in the Emergency Department. Extubation is not without its risk, however, as up to 30% of patients have respiratory distress secondary to laryngeal and upper airway edema, with some patients requiring re-intubation.
Prior to extubation, Intensivists use a brief “cuff-leak” test (deflation of the endotracheal balloon to assess the presence or absence of an air-leak around the tube) to indirectly screen for the presence of upper airway edema and ultimately the risk of re-intubation. The cuff-leak test is performed by deflating the endotracheal balloon followed by one or more of the following maneuvers:
Ochoa et al. performed a systematic review to determine the accuracy of the “cuff-leak” test to predict upper airway edema prior to extubation. The authors concluded that a positive cuff-leak test (i.e., absence of an air-leak) indicates an elevated risk of upper airway obstruction and re-intubation. A negative cuff-leak test (i.e., presence of an air-leak), however, does not reliably exclude the presence of upper airway edema or the need for subsequent re-intubation.
Bottom line: No test prior to extubation reliably predicts the absence of upper airway edema. Patients extubated in the Emergency Department require close observation with airway equipment located nearby.
Guide-wires can be challenging to dispose of after central-line insertion because they are difficult to keep on the field, hard to place in the sharps box, and can splash nearby observers.
Click here for this little guide-wire disposal trick.
27 year-old woman with AIDS presents complaining of a painful, puritic, and papular rash. What's the diagnosis?

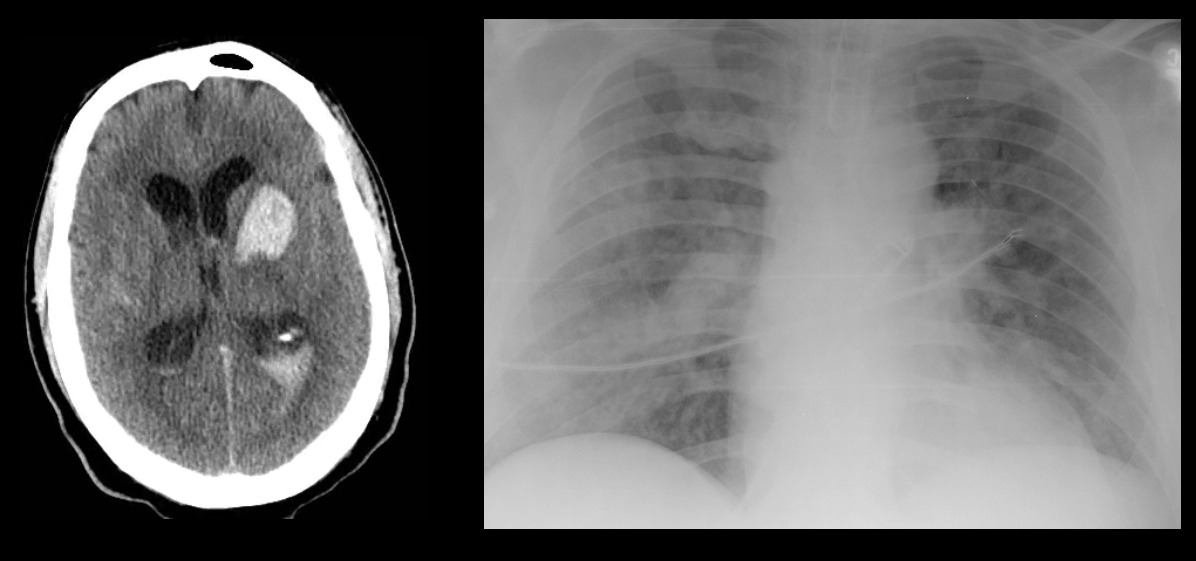
40 year-old male with severe uncontrolled hypertension presents with altered mental status (head CT below). The CXR is from the same patient. What's the connection?
40 year-old male with severe uncontrolled hypertension presents with altered mental status. Head CT is shown here. Name three common anatomic locations generally seen for non-traumatic intracerebral hemorrhage.
32 year-old female presents with 5 days of fever, chills, and flank pain. She is hypotensive on presentation and urinalysis shows pyuria. Click here for the non-contrast CT scan. What's the diagnosis and what type of antibiotics should be started empirically?
A Cochrane review of 37 studies concluded that Succinylcholine (SUC) is superior to Rocuronium (ROC) during rapid sequence intubation.
The authors claim that compared to ROC, SUC has a faster onset of action (45 vs. 60 seconds) and overall a shorter duration of action (10 vs. 60 minutes).
Dr. Reuben Strayer wrote a letter to the journal editors and stated that these findings should be interpreted carefully; he highlighted that most of the studies in the review used doses of ROC less than 0.9 mg/kg (most studies used 0.6mg/kg).
Dr. Strayer asserted that ROC’s onset of action is dose dependent; when using doses of 1.2 mg/kg, ROC’s onset is indistinguishable from that of SUC. He also stated another major benefit of ROC is the lack of adverse effects that SUC possesses (hyperkalemia and malignant hyperthermia).
What are your thoughts on this? Go to http://www.facebook.com/Criticalcarenow and take the poll (there are 5 choices). Results will be posted next week.
56 year-old male presents with chest pain. You perform an ultrasound of the heart and see the clip below. What's the diagnosis? Thanks to Dr. Ken Butler for the case.
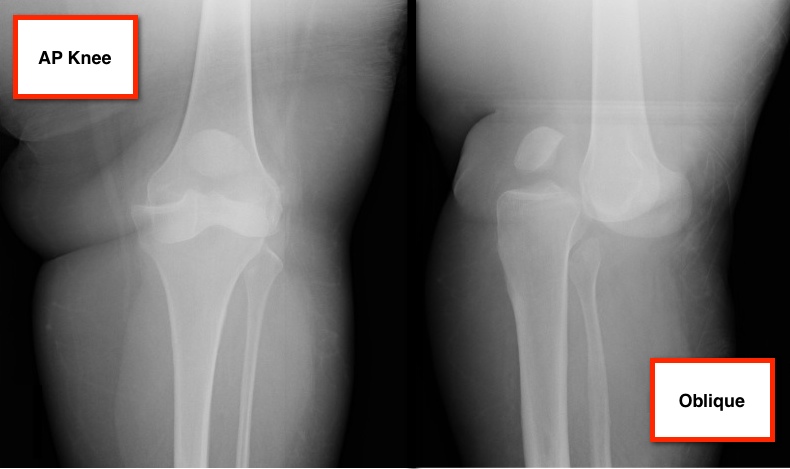
36 year-old female presents with left knee-pain following a motor vehicle crash (XRs are shown). What's the diagnosis AND what is the first test that should be performed to assess for vascular injury?