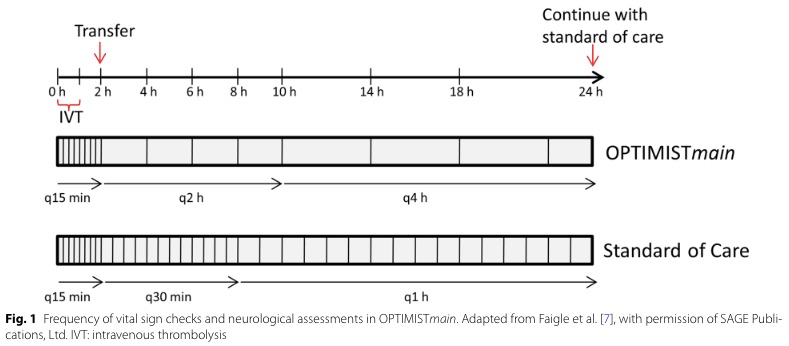
Bottom Line: Patients with NIHSS <10 may be safe for low-intensity post-tPA monitoring if they do not require critical care after an initial period of q15 min standard monitoring for the first 2 hours.
Bottom Line: Patients' language preference does not appear to affect the efficiency of acute ischemic stroke care, especially at experienced high volume stroke centers.
Bottom Line: Migraine is a common and debilitating condition that benefits from early treatment. Consider initiating preventive therapy for patients who experience at least 2 migraine days per month and adverse effects despite treatment.
| Central Nervous System | Peripheral Nervous System | |
| Pattern of Symptoms | • Hemibody involvement • Weakness of UE extensors • Weakness of LE flexors | • Distal involvement in polyneuropathy • Distal and proximal involvement in polyradiculoneuropathy • Proximal involvement in polyradiculopathy • Sensory often precedes motor symptoms • Pure proximal>distal weakness may be due to myopathy or NMJ disorder |
| Sensory Symptoms | • Central poststroke pain (hyperalgesia, allodynia) • Sensory level in spinal cord pathology • Proprioception involved early in dorsal column disorders | • Neuropathic pain (burning, tingling, shock-like) • Ascending sensory loss involving distal BLE>BUE in polyneuropathy • Proprioception involved late in polyneuropathy |
| Reflexes | • Hyperreflexia in affected limb(s) after acute period • Positive Babinski’s sign | • Hyporeflexia in affected limb(s) |
| Tone | • Increased after acute period | • Decreased |
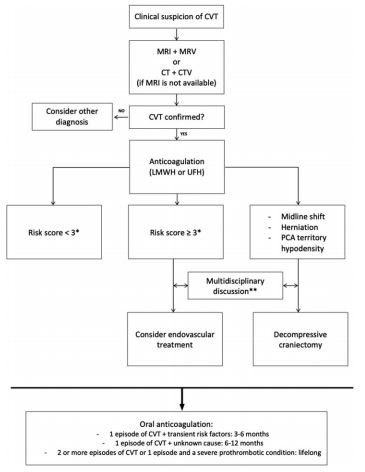
Bottom Line: Severity of CVT presentation depends on the location and clot burden. Anticoagulation is key, though consider endovascular intervention if patient does not improve or deteriorates despite anticoagulation.
Bottom Line: The incidence of CVT is increasing with rate of increase higher in males and older females. Consider CVT beyond traditional risk factors.
Bottom Line: New onset trigeminal neuralgia needs workup for its etiology. Carbamazepine and oxcarbazepine can be effective for symptom management though continuous or long-lasting pain exacerbations are difficult to treat.
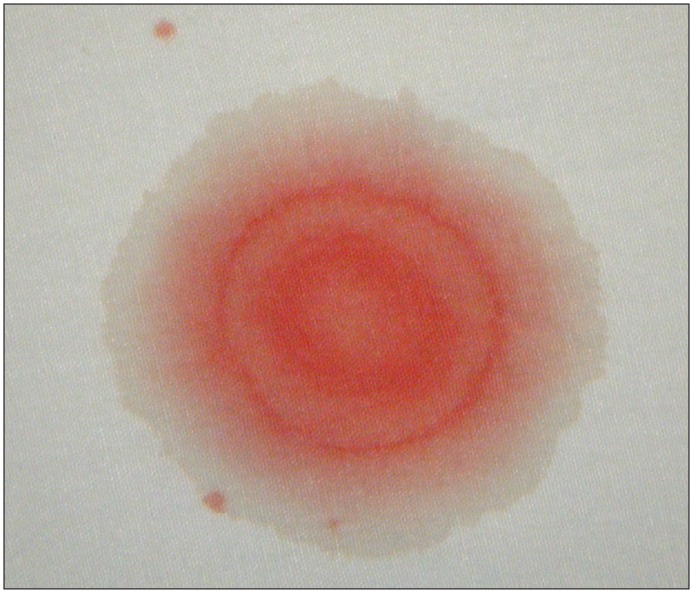
Bottom Line: Beta-2 transferrin is more accurate than the halo sign to identify CSF containing fluid.
Idiopathic intracranial hypertension (IIH) is a vision-threatening illness with significant morbidity and needs to be considered as a possible headache diagnosis in the ED. Most often, this occurs in women of childbearing age with a BMI >30, but atypical varieties exist.
Symptoms: Headache (90%), visual disturbance, pulsatile tinnitus, horizotal diplopia.
Signs: Papilledema, 6th cranial nerve (abducens) palsy.
Evaluation: Neuroimaging including CTV or MRV to identify alternate cause including cerebral venous outflow obstruction, lumbar puncture with opening pressure >30 cmH2O (25-30 cmH2O is gray zone), blood work per clinical presentation, CSF analysis.
Treatment: No clear consensus, but typically acetazolamide. Severe or refractory symptoms may require surgical intervention such as optic nerve sheath fenestration, VP shunt, venous sinus stenting.
Bottom Line: Pregnancy is associated with an increased risk for RCVS, CVT, and Bell’s Palsy. Pregnancy also affects the frequency of migraines due to hormonal fluctuations.
Bottom Line: Discussion of benefit/risk and financial incentive associated with head CT in mild TBI affects patient decision. Interestingly in this population studied, more than half of patients will elect to obtain a head CT even in a low-risk scenario.
Bottom Line: Cervical collars can increased ICP in moderate-severe TBI. In patients with poor cerebral compliance and impaired cerebral autoregulation, even a small increase in ICP can affect cerebral perfusion.
Bottom Line: SARS-CoV has been associated with CNS involvement. Given their similar pathogenesis and finding of hyposmia in COVID-19, SARS-CoV-2 may be associated with risk of CNS involvement.
Bottom Line: Patients on warfarin or a combination of aspirin and clopidogrel have increased risk of significant intracranial injury after blunt head trauma. Aspirin or clopidogrel monotherapy do not appear to be risk factors.
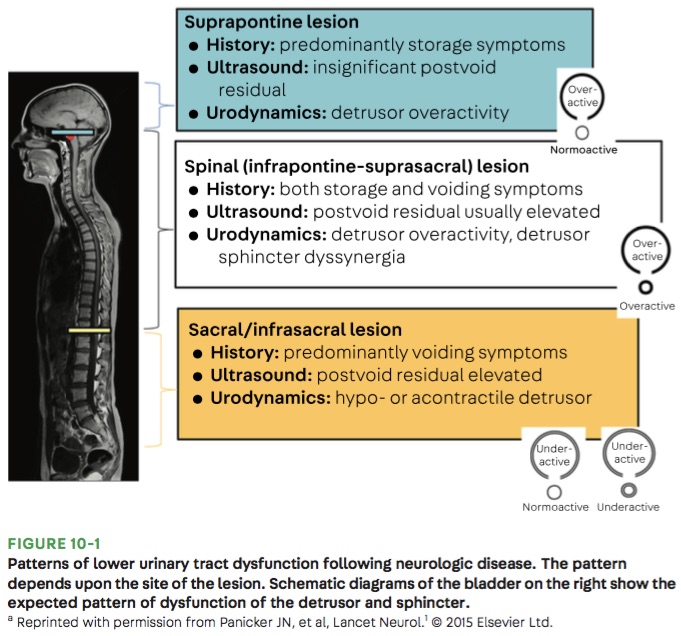
Bottom Line: Urinary retention can be seen with neurological injury involving the lower brainstem, spinal cord, cauda equina, and peripheral nerves.
Bottom Line: Fosphenytoin, valproate, and levetiracetaim have similar efficacy in treatment of benzodiazepine-resistant status epilepticus.
Bottom Line: Consider cryptococcal meningitis even in immunocompetent patients.
Bottom Line: Reduced SBP variability is associated with improved outcomes in ICH.