Every year, numerous children die of non-exertional heatstroke after being left in motor vehicles in the United States. Per data obtained from the national nonprofit KidsAndCars.org, the average number of pediatric vehicular heatstroke deaths is 39 per year since 1990. In 2018, this number peaked at 54 pediatric deaths. Prior studies show that the interior temperature of a closed vehicle rises quickly within minutes of closing the doors and windows. This rapid change occurs even on days with cooler ambient temperatures (20s °C/70s °F): the interior temperature of a car may still reach 117F within an hour.
Children, particularly infants and toddlers, are at increased risk for heat illness due to several physiologic and developmental factors:
- Unable to escape hot environments or to self-hydrate
- Lack mature thermoregulatory systems
o Have lower rate of sweat production than adults
- Have higher basal metabolic rates than adults
- Have higher body surface area:mass ratio --> absorb heat faster in hot environments
Bottom line: ED providers can be instrumental in giving anticipatory guidance on vehicular heatstroke in children during the warmer seasons:
- Educate caregivers to “Look before you Lock”
- Suggest that the caregiver place a valuable object (phone, employee badge, handbag) in the back seat when traveling with a child
- Remind caregiver of the dangers of intentionally leaving a child in the car for any reason, even during cooler spring/summer days.
NHTSA recommends that car seats be replaced following a moderate or severe crash. Car seats do not automatically need to be replaced following a minor crash.
A minor crash is one in which ALL of the following apply:
-The vehicle was able to be driven away from the crash site.
-The vehicle door nearest the car seat was not damaged.
-None of the passengers in the vehicle sustained any injuries in the crash.
-If the vehicle has air bags, the air bags did not deploy during the crash
-There is no visible damage to the car seat.
NEVER use a car seat that has been involved in a moderate to severe crash. Always follow manufacturer's instructions.
The leading cause of death in the US for those aged 16 to 24 years is motor vehicle collisions (MVCs). Teen drivers are more likely than any other age group to be involved in an MVC that result in injury or fatality. Texting while driving, nighttime driving, inexperienced driving, and driving under the influence of alcohol or drugs may play a role in these collisions.
Can anticipatory guidance related to safe driving be done in the ED? YES!
This study implemented a toolkit that contained a copy of the driving law, a sample parent-teen driving contract and statistics on teen driving injuries. Post toolkit questionnaires showed that both teens and their guardians learned new information.
Bottom line: Engage in anticipatory guidance in the ED with teens and their parents about seatbelt use, the dangers of driving under the influence and local driving laws.
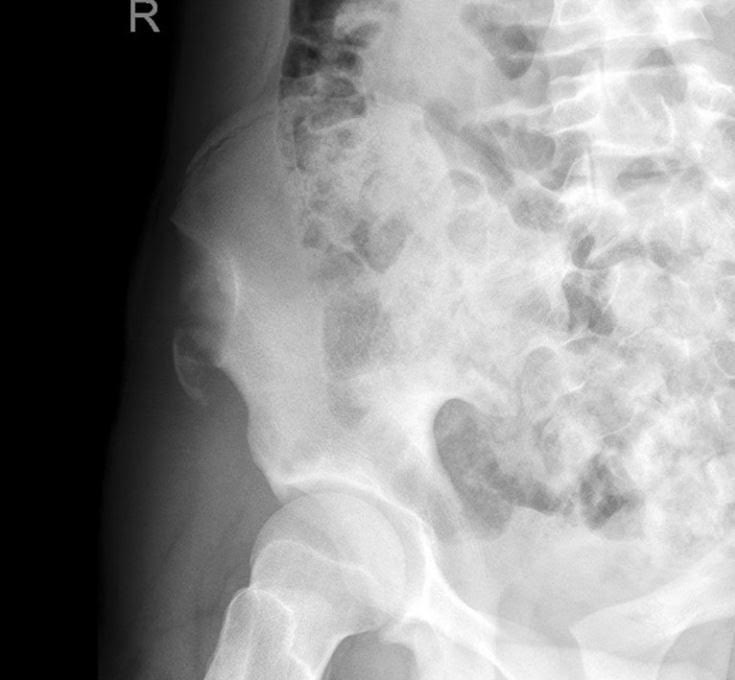
A 15 y.o. female presents to your emergency department with sudden onset hip pain after winding up to kick a soccer ball during her game today. You see a well-developed female in obvious discomfort, with tenderness to palpation over her lateral hip and pain with passive ROM at the hip. You obtain this x-ray. What is your diagnosis?
Tonsillectomy and adenoidectomy (T&A) is the second most common ambulatory surgery performed in the US. Children younger than 3 years, children with craniofacial disorders or sleep apnea are typically admitted overnight as studies have shown an increase rate of airway or respiratory complications in this population.
The most common late complications include bleeding and dehydration. Other complications include nausea, respiratory issues and pain.
Post-operatively, the overall 30-day emergency department return rate is up to 13.3%. Children ages 2 and younger were more likely to present to the ED. There is significantly higher risk of dehydration for children under 4 years. Children over the age of 6 had significantly higher bleeding risk and need for reoperation for hemorrhage control.
Urinary retention in pediatrics is defined as the inability to void for more than 12 hours in the presence of a palpable bladder or a urine volume greater than expected for age.
Maximum urine volume calculation for age: (age in years + 2) x 30ml.
Causes of urinary retention include mechanical obstruction, infection, fecal impaction, neurological disorders, gynecological disorders and behavioral problems.
The distribution is bimodal occurring between 3 and 5 years and 10 to 13 years.
Antibiotic stewardship has led various organizations such as the AAP, AAFP, and IDSA to introduce two different approaches to the treatment of acute otitis media (AOM):
Immediate treatment with antibiotics should always include the following patients:
The observation approach can be considered in the following very slect patient group:
Often the issue with pediatric AOM isn't necessarily the overprescribing of antibiotics, but the inaccurate/inappropriate over diagnosis of acute otitis media. An erythematous tympanic membrane does not equal AOM. Crying and fever can result in a red TM. Fluid seen behind the TM, is often just serous otitis media, which isn't AOM.
When antibiotics are warranted, first-line treatment is with high dose amoxicillin, 90 mg/kg per day divided into two doses; unless the child has received beta-lactam antibiotics in the previous 90 days and/or also has puruent conjunctivitis mandating amoxicillin-clavulanate instead. In the later case, prescribing the Augment ES, 600 mg/5mL formlation with a lower clavulanic concentration lessening GI upset and diarrhea is prefered.
Streptococcal pharyngitis is common in the pediatric population however in children younger than 3 years, group A streptococcus (GAS) is a rare cause of sore throat and sequela including acute rheumatic fever are very rare. Inappropriate testing leads to increased healthcare and unnecessary exposure to antibiotics.
The national guidelines published by the Infectious Diseases Society of America do NOT recommend GAS testing in children less than the age of 3 years unless the patient meets clinical criteria and has a home contact with documented GAS.
Bottom line: Balance fluid resuscitation with LR was not associated with improved outcomes compared to NS and pediatric sepsis. Selective LR use necessitates a prospective trial to definitively determine comparative effects among crystalloids.
- Tibial tubercle avulsion fractures are rare and pediatrics, accounting for less than 3% of all epiphyseal injuries in children ages 11-17 years.
- The typical mechanism is a sudden forceful quadriceps contraction. Patients present with sudden pain after sprinting or jumping with pain, bruising, deformity or swelling over the tibial tubercle and with a decrease ability to extend the leg.
- 10 to 20% of cases result in anterior compartment syndrome related to the rupture of the anterior tibial recurrent artery.
- Although directly measured intra-compartmental pressures can facilitate the diagnosis of compartment syndrome, interpretation of these values can be challenging with healthy children having higher average lower leg compartment pressures than adults. Treatment of subsequent compartment syndrome is often based on a high index of suspicion.
Question: In febrile children younger than 2 years, what combination of clinical and laboratory variables best predicts the probability of a urinary tract infection?
Given that urinary tract infections (UTI) are the most common source of serious or invasive bacterial infections in young febrile infants, early identification and treatment has the potential to reduce poor outcomes. Wouldn't it be great if there was an easy way to identify patients at highest risk?
Researchers from the Children’s Hospital of Pittsburgh formulated a calculator (UTICalc) that first estimates the probability of urinary tract infection (UTI) based on clinical variables and then updates that probability based on laboratory results.
Bottom line:
The UTICalc calculator can be used to guide to tailor testing and treatment in children with suspected urinary tract infection with the hope of improving outcomes for children with UTI by reducing the number of treatment delays.
Go ahead and give it a click!! https://uticalc.pitt.edu/
There is no standardized national reporting of dog bites in the US. Based on the reported figures, it is estimated that 2% of Americans are bitten annually, and children are affected disproportionately. With kids, it's usually the family dog, and occurs at home.
To avoid infection, usually from Pasturella species, many of us were taught never to primarily repair dog bites by suturing, and to always prescribe prophylactic antibiotic coverage with amoxicillin-clavulanate. However, the literature recommends otherwise in certain cases.
Bite wounds to the face and hands should have special considerations. In general, face wounds heal with lower rates of infection, but provide the greatest concern for cosmetic appearance. Hand wounds have notoriously higher rates of infection.
The latest recommendations for dog bites are as follows:
1. All dog bites should be copiously irrigated under high pressure.
2. Dog bites to the face should be primarily repaired when <8 hours old, as infection rates are not significantly different and cosmesis is greatly improved.
3. Injuries to the hands should be left open, unless function is in jeopardy or there are neurovascular concerns.
4. Prophylactic antibiotics do not always have to be prescribed, especially in low risk patients. Examples of high risk patients include, but are not limited to: primarily repaired bites, injuries in the hand, >8 hours old, deep or macerated or multiple bites, and the immunocompromised.
Gunshot injuries are a leading cause of morbidity and mortality in the pediatric population. The Pediatric Trauma Society supports the use of tourniquets in severe extremity trauma. The Combat Application Tourniquet (CAT) that is commonly used in adults has not been prospectively tested in children. This study used 60 children ages 6 through 16 years and applied a CAT to the upper arm and thigh while monitoring the peripheral pulse pressure by Doppler. The CAT was successful in occluding arterial blood flow in all of the upper extremities and in 93% of the lower extremities.
Bottom line: The combat application tourniquet can stop arterial bleeding in the school aged child.
-Benzodiazepines alone are effective in terminating status epilepticus in 40 to 60% of pediatric patients
-The guidelines for second line agents are based on observational studies and expert opinion
-Adverse effects of phenytoin include hepatotoxicity, pancytopenia, Stevens-Johnson syndrome, extravasation injuries, hypotension and arrhythmias
- Levetiracetam has a reduced risk of serious adverse events, greater compatibility with IV fluids and can be given in 5 minutes versus 20 minutes for phenytoin.
Bottom line: In a recent randomized control trial they found that levetiracetam was not superior to phenytoin as a second line agent for management of convulsive status epilepticus in children. There was no difference between efficacy or safety outcomes between the two groups.