The radial nerve is susceptible to compressive neuropathy against the spiral grove of the humerus which can lead to neuropraxia.
When the upper arm is compressed against a chair back or bar edge sometimes from a lost battle with alcohol: Saturday night palsy.
When another individual sleeps on someone’s arm overnight compressing the radial nerve: Honeymoon palsy
From nerve compression from improper technique with crutches: Crutch palsy
If diagnosis not clear from history, DDx includes other entities that can also present with isolated wrist, thumb/finger drop
Horses: Radial verve palsy, CVA, C7 compression
Zebras: Lead toxicity, acute porphyrias (often polyneuropathy but upper extremity before lower and frequently distal extensors
Careful history and exam important in differentiating
In cases of peripheral compression against the spital groove the triceps maintains strength.
The distal extensors lose strength (wrist and fingers)
Including the thumb abduction (abductor pollicis longus is radial-innervated)
AND so will the brachioradialis
The brachioradialis (despite being a forearm flexor) has dual innervation from the radial nerve in 80% of people.
Brachioradialis strength is often preserved in a central lesion.
Best tested with arm supported on a surface in mid pronation/supination (hammer curl position) and have patient flex against resistance and evaluate muscle strength and bulk.
28-year-old male present with dorsal hand pain after “losing his temper”
On exam, you note dorsal swelling, tenderness, and deformity
AP, lateral and oblique views are obtained.
There is no rotational deformity but using the lateral view, you note that there is angulation
Measured as the shaft of the metacarpal as compared to the mid-point of the fracture fragment
Acceptable shaft angulation generally accepted to be less than 40°
Patient has greater that acceptable angulation so you have to perform closed reduction
After appropriate pain control consider the “90-90 method.”
Flex the MCP, DIP, and PIP joints to 90 degrees.
This positioning stretches the MCP collateral ligaments helping to optimize reduction
Next, apply volar pressure over the dorsal aspect of the fracture site while applying pressure axially to the flexed PIP joint.
Best demonstrated below
https://www.youtube.com/watch?v=40irKoUJqsM
4-year-old patient comes to the ED for an unrelated complaint and you notice that his knees appear to be touching while his ankles remain apart.
Genu Varum or “knock knees” may be caused by Infantile Blount’s disease
-A progressive pathologic condition causing genu varum in children between ages 2 to 5
- Centered at the tibia
-Bilateral in up to 80%
-More common in boys
-Leg length discrepancy
- Articular incongruity
Risk factors: Early walkers (<1 year), overweight, large stature, Hispanic and African American
Results in disruption of normal cartilage growth at the MEDIAL aspect of the proximal tibia while LATERAL growth continues normally
May complain of knee soreness or subjective instability
On physical exam
Focal angulation of the proximal tibia
Lateral thrust during stance phase of walking (brief lateral shift of proximal fibula and tibia)
No tenderness or effusion
Imaging: Plain film shows varus deformity of the proximal tibia with medial beaking (beak like appears of bone) and downward slope of the proximal tibia metaphysis (increased metaphyseal-diaphyseal angle)
https://paleyinstitute.org/wp-content/uploads/blounts1.jpg
Treatment depends upon the age of the child and the severity
Successful in up to 80%
Note: In adolescent variant bracing is ineffective and surgery is only treatment
: Genu varum is normal in children <2 years old and becomes neutral at 14 months
DDX: Physiologic varus, Rickets
9-year-old male left hand dominant, presents with left elbow pain.
He is a future “star pitcher,” says his coach dad. “Doc, I bet you didn’t know that although only 10% of people throw with their left hand almost a 1/3rd of MLB pitchers are lefties. He is 3x more likely than a righty to pitch in MLB.” “Maybe I’m asking him to throw too much.”
Hx: Lateral elbow pain and “stiffness” worse with activity that is better with rest
PE: Lateral elbow tenderness (capitellum) with slight (approx. 20 degrees) decreased loss of extension. Minimal swelling noted.
Dx: Panner's disease refers to osteochondrosis of the capitellum (similar to Legg Calve Perthes). Likely due to AVN from repetitive trauma. May also be due to endocrine disturbances.
Affects the dominant elbow of boys between the ages of 5 and 10
Associated with the repetitive trauma of throwing or gymnastics.
Must be differentiated from osteochondrosis dissecans which occurs in the older child >13yo when the ossification of the capitellum is complete
Radiology:
The articular surface of the capitellum may appear irregular or flattened with areas of radiolucency (43%). Loose bodies not seen with Panners, much more likely with OCD lesions.
Treatment: Ice and NSAIDs. Avoid pitching/gymnastics etc. until full radiographic and clinical healing. If significant pain and/or swelling place patient in long arm posterior splint for 7-10 days. Resolution may take several months and up to one year.
A recent study investigated the association between concussion and subsequent mental health conditions in a pediatric population.
Retrospective cohort study. Pediatric patients aged 5 to 18 years who presented to an ED, PCP or mental health practitioner from April 2010, to March 2020, in Ontario, Canada.
Primary outcome: Time to first diagnosis with a mental health condition during follow-up
Secondary outcomes: 1) self-harm 2) psychiatric hospitalization 3) death by suicide.
Mental health conditions: anxiety and neurotic disorders, adjustment reactions, behavioral disorders, mood and eating disorders, schizophrenia, substance use disorder, suicidal ideation, and disorders of psychological development.
Study group, almost 450,000 patients. Age and sex matching between those with concussion and those who experienced an orthopedic injury.
A significant association (P < .001) was found between concussion and mental health conditions
A significant association emerged between concussion and self-harm and psychiatric hospitalization
No association with suicide
Conclusion: Concussion was significantly associated with risk of mental illness, psychiatric hospitalization and self-harm but not death by suicide.
Concussed patients had an almost 40% higher rate of mental health conditions compared to controls (adjusted hazard ratio 1.39)
Take home: Screen patients who return to the ED with post concussive symptoms for mental health symptoms/concerns and provide appropriate awareness for parents
The knee is one of the most commonly affected joints from osteoarthritis (OA).
Patients will complain of knee pain, swelling and stiffness.
This leads to disability as it interferes with walking, using stairs at home and getting in and out of chairs and the bath without assistance.
Increasing incidence due to aging of the general population and rising rates of obesity.
Patients frequently present to the ED for knee pain and imaging is often obtained.
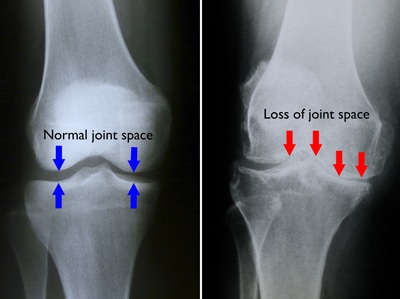
Diagnosis of knee OA can be made with an appropriate history and imaging that shows osteophytes and joint space narrowing.
The best views for knee OA include 1) PA weight-bearing & 2) 45 degree of knee flexion
https://d3i71xaburhd42.cloudfront.net/6f8ce215fb4bcd153a478187c9a6a2ae652a5fc4/250px/1-FigureI-1.png
Note: Weight-bearing radiographs will demonstrate greater joint space narrowing than non-weight-bearing radiographs
Of the 3 compartments of the knee, the medial tibiofemoral compartment is most commonly affected > patellofemoral compartment > lateral tibiofemoral compartment.
Examples of knee OA
https://roberthowells.com.au/wp-content/uploads/2016/04/A00212F02.jpg
https://orthoinfo.aaos.org/link/e7e6933819db4020bc2f3822c45c538f.aspx
Quadriceps contusion
Mechanism: Blunt trauma from ball, helmet, stick
Usually to the central region
Damage to highly vascular area of the muscle and to local blood vessels can cause hematoma formation
Typical trauma history and pain worse with muscle activation (knee flexion)
Physical exam: Bruising, tenderness, palpable mass/hematoma
Goals of care: Minimize intramuscular bleeding
Treatment: NSAIDS, crutches, unique type of immobilization
Attempt to increase resting length of the quadriceps muscle to facilitate early healing and return to function
Note: Left untreated, large contusions may result in myositis ossificans
Hamstring Injury
Prevalence varies by sport ranging from 8 to 25 percent with a high recurrence rate frequently during the ensuing sport season, usually in next 2 months but may extend up to one year!
Highest in sports that involve rapid acceleration and deceleration
3 highest risk sports - football and men’s and women’s soccer
Average time lost 17-21 days
Injury much less common in younger athletes
The hamstring is composed of three muscles: the biceps femoris, semitendinosus, and semimembranosus.
Primarily involved in knee flexion and hip extension
Biceps femoris is most commonly injured
https://www.ncbi.nlm.nih.gov/books/NBK539862/figure/article-28873.image.f1
Simple grading system using 3 grades
Grade 1 – mild strain
Grade 2 – Partial tear
Grade 3 – Complete tear
Proximal injuries are more common than distal injuries, occurring at the musculotendinous junction
Avulsion fractures of the ischium occur rarely occur in adults but may occur in skeletally immature athletes
https://radiopaedia.org/cases/ischial-tuberosity-avulsion
When watching a sporting event you will see the athlete grab the buttock or upper thigh. They usually cannot return to play. Most grade 2 or 3 injuries will require crutches. If seeing them the following day significant bruising may be seen.
Numerous modifiable and non-modifiable risk factors have been identified including:
*Weakness of ipsilateral quadriceps or contralateral hamstring, hamstring, hip & quadriceps tightness/poor flexibility, poor warm-up, sudden increased training volume and muscle fatigue.
*Older age (risk increase may begin as early as age 23)
Prior hamstring injury (up to 6x increased risk)
**Premature return to sport increases the risk of reinjury
Differential Diagnosis: Lumbar radiculopathy, sciatic nerve irritation or compression, stress fracture of femur.
Refer to sports medicine/orthopedics for avulsion injuries, complete proximal complete tears and partial or complete distal tears
Presentations of Fracture in Nursemaids Elbow
Study group: Visits by children younger than 10 years, with a diagnosis of radial head subluxation at 1 of 45 pediatric EDs from 2010 to 2018.
Retrospective cohort study of 88,466 ED visits for radial head subluxation
Outcome: Missed fracture (return visit for upper extremity fracture within 7 days of the index visit).
Results
Median patient age was 2.1 years,
59% of visits were by female patients,
60% of cases occurred in the left arm.
Radiography was performed at 28.5% of visits (Range 19.8% to 41.7%.)
Extremity fractures were observed in 247 cases, representing 0.3% of the cohort.
The odds of missed fracture were higher in:
Summary:
Only 0.3% of children with a diagnosis of radial head subluxation subsequently received a diagnosis of an upper extremity fracture within 7 days of the index visit.
Missed fractures were commonly about the elbow such as a supracondylar fracture. However, this study also found a significant proportion of missed fractures in other locations (e.g. shoulder, wrist), highlighting the importance of a careful physical examination, and the limitations of localizing pain in younger children.
Recurrence was common, and the risk of recurrence decreased with increasing age at first presentation. Overall, radial head subluxation recurrence was 8.7% after the first visit VERSUS 12%-13% in children younger than 2 years. THese patients are likely to return to the ED with a recurrence within 2 years. These findings should help inform anticipatory guidance to parents regarding the risk of recurrence based on their child’s age.
The classic mechanism for nursemaids elbow is axial traction on a pronated forearm and extended elbow.
The force allows a portion of the annular ligament to slip over the radius.
Consider this diagnosis with other mechanisms of injury especially if the exam is not suggestive of fracture.
Suspect in a patient in minimal distress with arm held semi flexed and pronated.
A recent retrospective study looked at other mechanisms of injury.
69 subjects with a median age of 2.5 years
The most common mechanisms of injury were fall (57%), direct hit to the elbow (16%), and rolling over (7%).
Some studies note the left elbow is more commonly involved but this is likely due to most guardians being right-handed, thereby holding the child’s left hand
The total number of concussions tripled among female athletes aged 14 to 18 years during a 20-year period from 2000 to 2019.
Query of National Injury Surveillance System
Female athletes with sports-related concussions or closed head injuries who presented to the ED
In 14- to 18-year-old females the number of concussions increased from 9,000 in 2000 to 32,000 in 2019.
65% of all concussions among female athletes occurred in soccer, basketball, cheerleading, softball, and volleyball.
Association between an increase of 308.7 annual concussions per 10,000 annual female participants.
In a study of more than 80,000 teenage players across US high schools, female athletes are 1.9 times more likely to develop a sports-related concussion than are their male counterparts in comparable sports.
In boys, the most common way of becoming concussed was through direct contact with another player (50%)
In girls, the most common way of becoming concussed was after colliding with another object (ball/goalpost).
This mechanism may partly explain another finding: Boys were also more likely to be removed from play immediately after a suspected head injury than were girls
The Role of Active Rehabilitation in Concussion Management: A Systematic Review and Meta-analysis
Concussions make up 70% to 90% of all traumatic brain injuries
During the recovery process, prolonged rest has been shown to slow recovery and precipitate secondary symptoms of fatigue, reactive depression, anxiety and physical deconditioning.
As a result, a gradual increase in low-level activities has been encouraged after 24-48 h of rest.
23 articles for a total of 2547 concussed individuals, 49% female, both kids and adults. Included both sport related and non-sport related concussion.
None of the studies reported any adverse events in symptomatic participants after subthreshold exacerbation aerobic exercise.
Duration ranged from 15-20 minutes per session or until symptom exacerbation.
Subthreshold activity generally targeted 80% of max heart rate achieved during a graded symptom threshold test.
Every study showed improved concussion symptom scores with a physical activity intervention.
Most common treatment duration was 6 weeks (Range 1-12 wk)
Best outcomes if initiated with 2-3 weeks after injury but intervention beneficial in chronic phases of recovery as well.
The intervention of physical activity decreases post concussion symptom scores and the overall effect across studies was large and positive.
Optimal intensity, duration and time to initiation of exercise intervention needs further investigation.
Exercise effect is likely multifactorial including:
One of the best effects I have seen in treating these patients is that active exercise allows a proactive approach to patient recovery. Patients become less focused on every minor symptom or irregularity.
Exertional Heat Stroke at the Boston Marathon
Study goal: To assess for possible associations between exertional heat stroke (EHS) and sex, age, prior performance and environmental conditions
Data sourced from 2015-2019 Boston Marathon races.
Why Boston: The Boston marathon is one of the only marathons that require qualifying times for entry for a majority of runners which yields a high proportion of faster than average runners. The race is frequently characterized by extreme weather conditions, including warm and humid days.
Results: 136,161 race starters. Incidence of EHS was 3.7 cases per 10,000 starters.
Note: Twin Cities Marathon found 3 cases per 10,000 runners.
Mean age of runners was 43.3. Female 45%, male 55%.
Significant associations between sex and age, sex and start wave and age group and start wave.
Sex not associated with increased EHS incidence.
Age < 30 and assignment to the first 2 waves (faster runners) was significantly associated with increased EHS.
All cases of EHS occurred with average wet bulb globe temperatures (WBGT) were 17° – 20° C.
Linear correlation between EHS and incidence in addition to increases in WBGT from start to peak.
72.5% of cases were race finishers. Non finishers presented after mile 18.
Almost 30% developed post treatment hypothermia.
Almost 2/3rds were discharged directly, the remainder required hospital transport.
Authors estimate needing at least 4 ice water immersion tubs per 10,000 runners with potential of needing 8-10 if race day is humid.
Conclusions: Overall, EHS represented a small percentage of medical encounters but required significant resources.
Younger and faster runners are at high risk of EHS.
Greater increases in heat stress from start to peak worsens risk.
Definitions: WGBT - The Wet Bulb Globe Temperature (WBGT) is a measure of the heat stress in direct sunlight, which takes into account: ambient temperature, relative humidity, wind speed, sun angle and cloud cover (solar radiation). This differs from the heat index, which takes into consideration temperature and humidity and is calculated for shady areas.
Chronic Exertional Compartment Syndrome (CECS)
Similar pathology to acute compartment syndrome except symptoms are related to activity (frequently running) and abate with rest.
95% involve lower extremity
Inappropriately elevated tissue pressure in one or more lower leg compartments associated with exercise
Anterior compartment most frequently involved
As tissue pressure increases, local perfusion is decreased. This leads to symptoms of pain, pressure, cramping and paresthesias.
Also commonly associated with team sports such as soccer, lacrosse and field hockey.
More likely in competitive athletes than recreational.
Patient will be symptom free at time of ED evaluation
Make diagnosis of CECS with history
Diagnosis with compartment pressure measurements done in office with treadmill exercise.
Non operatively, gait retraining programs have been shown to help symptoms. Appropriate if symptoms are mild.
Surgical treatment involves a minimally invasive fasciotomy
Post surgery success rates are between 63-100% with recurrence rates up to 20%
Low dose ketamine was compared to morphine for the treatment of patients with long bone fractures
126 patients with upper and lower extremity long bone fractures were divided into two treatment groups
Pain scores were compared pre and at 10 minutes post treatment
Pain severity significantly decreased in both groups to a similar degree
Increase adverse effects (emergence phenomenon) noted in ketamine group but all effects resolved spontaneously without intervention.
Conclusion: Analgesic effect of ketamine is similar to morphine in patients with long bone fractures.
NSAIDs for lower back pain (LBP)
NSAIDs are recommended for first line treatment of lower back pain.
Ibuprofen (600mg), ketorolac (10mg) and diclofenac (50mg) were compared.
3 arm, double-blinded study in an ED population with musculoskeletal LBP.
66 patients in each arm.
Outcomes via telephone interview 5 days later
Primary outcome was improvement in Roland-Morris Disability Questionnaire (RMDQ).
Lower scores indicate better LBP functional outcomes.
Secondary outcomes: Pain intensity and the presence of stomach irritation.
Baseline characteristics similar in 3 groups.
Results: No significant differences between 3 arms in primary outcome.
Ibuprofen 9.4, ketorolac 11.9, and diclofenac 10.9 (p = 0.34).
Ketorolac group reported less overall pain intensity at day 5.
Ketorolac group reported less stomach irritation that the other drugs ((p < 0.01).
While there was no differences in terms of functional outcomes, there may be a benefit of using ketorolac in terms of overall pain intensity and stomach irritation. This would benefit from further study in a larger population in order to draw definitive conclusions.
You are covering a sporting event or working an ED shift when a young adolescent athlete without significant PMH presents with SOB and wheezing associated with exercise.
You immediately think exercise-induced asthma, prescribe a short-acting bronchodilator and pat yourself on the back.
While you may be right, there is increasing recognition of an alternative diagnosis
Exercise-induced laryngeal obstruction (EILO)
During high intensity exercise, the larynx can partially close, thereby causing a reduction in normal airflow. This results in the reported symptoms of SOB and wheezing.
This diagnosis has previously been called exercise induced vocal cord dysfunction. As the narrowing most frequently occurs ABOVE the level of the vocal cord, EILO is a more correct term.
While exercise induced bronchoconstriction has a prevalence of 5-20%, EILO is less common with a prevalence of 5-6%.
Patients are typically adolescents, with exercise associated wheezing and SOB, frequently during competitive or very strenuous events. Wheezing is inspiratory and high-pitched. Symptoms are unlikely to be present at time of medical contact unless you are at the event as resolution occurs within 5 minutes though associated cough or throat discomfort can persist after exercise cessation. EIB symptoms typically last up to 30 minutes following exercise.
Inhaler therapy is unlikely to help though some athletes report subjective partial relief. This may be explained as approximately 10% of individuals have both EIB and EILO.
In athletes with respiratory symptoms referred to asthma clinic, EILO was found in 35%.
Consider EILO in athletes with unexplained respiratory symptoms especially in those with ongoing symptoms despite appropriate therapy for EIB.
Hand elevation test
https://www.youtube.com/watch?v=IO2qC5qHVFE
Both erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) are highly sensitive (84-100%) for spinal infections and are observed in >80% with vertebral osteomyelitis and epidural abscesses.
ESR
Most sensitive and specific serum marker, usually elevated in both spinal epidural abscess (SEA) and vertebral osteomyelitis.
ESR was elevated in 94-100% of patients with SEA vs. only 33% of non-SEA patients
Mean ESR in patients with SEA was significantly elevated (51-77mm/hour)
CRP
Not highly specific
Less useful for acute diagnosis since CRP levels rise faster and return to baseline faster than ESR (elevated CRP seen in 87% of patients with SEA as well as in 50% of patients with spine pain not due to a SEA)
Better used as a marker of response to treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}