Trapezium Fractures
Suspect the Diagnosis when you note
If you are suspected the diagnosis oblique radiographs or a CT scan of the wrist will note the fracture the best.
Treatment consists of placing the patient in a thumb spica splint.
The adolescent brain has not yet reached full maturation and is in a period of rapid development from ages 14 - 16.
Adolescents have been found to be more sensitive to the effects of concussion than adults
Concussed adolescents have deficits in attention and executive function lasting up to 2 months post injury.
Be aware that the adolescent brain will require extended recuperation time following injury
In the future, discharge instructions might need to say more than "don't get hit in the head till your headache goes away." Because of deficits in attention and executive function, physicians should consider recommendations about adolescents and jobs, school work and driving an automobile.
Adhesive capsulitis aka frozen shoulder
idiopathic loss of BOTH active and passive motion (this is a significant reduction of at least 50%)
Motion is stiff and painful especially at the extremes
Occurs due to thickening and contracture of the shoulder capsule
Affects patients between the ages of 40 and 60
Diabetes is the most common risk factor
Imaging is normal and only helpful to rule out other entities such as osteophytes, loose bodies etc.
Treatment includes NSAIDs, moist heat and physical therapy.
Patients should expect a recovery period of 1-2 years!
Fabella Syndrome
The fabella is a sesamoid bone that is embedded in the tendon of the gastrocnemius muscle where the fibers of the popliteus, arcuate complex and the fibular-fabellar ligament attach.
Fabella syndrome is a painful condition of the posterolateral knee that is exacerbated when the knee is extended. The pain can be exacerbated by palpation of the fabella and if it is compressed against the condyles. The condition is most common in adolescence, but occurs in adults too.
Consider this condition in patients with posterolateral knee pain, which can also be due to tears of the posterior horn of the lateral meniscus, and tendonitis of the lateral head of the gastrocnemius.
You have a patient with a spinal cord syndrome and you order the MRI. Have you ever had that conversation with radiology where you have to "choose" what part of the spine you want imaged?
The entire spine needs to be imaged!
The reason: False localizing sensory levels.
For example: The patient has a thoracic sensory level that is caused by a cervical lesion.
A study of 324 episodes of malignant spinal cord compression (MSCC) found that clinical signs were very unreliable indicators of the level of compression. Only 53 patients (16%) had a sensory level that was within 3 vertebral levels of the level of compression demonstrated on MRI.
Further, pain (both midline back pain and radicular pain) was also a poor predictor of the level of compression.
Finally, of the 187 patients who had plain radiographs at the level of compression at referral, 60 showed vertebral collapse suggesting cord compression, but only 39 of these predicted the correct level of compression (i.e. only 20% of all radiographs correctly identified the level of compression).
The authors note that frequently only the lumbar spine was XR at the time of clinical presentation (usually at the referring hospital), presumably due to false localizing signs and a low awareness on the part of clinicians that most MSCC occurs in the thoracic spine (68% in this series).
You have a patient with a spinal cord syndrome and you order the MRI. Have you ever had that conversation with radiology where you have to "choose" what part of the spine you want imaged?
The entire spine needs to be imaged!
The reason: False localizing sensory levels.
For example: The patient has a thoracic sensory level that is caused by a cervical lesion.
A study of 324 episodes of malignant spinal cord compression (MSCC) found that clinical signs were very unreliable indicators of the level of compression. Only 53 patients (16%) had a sensory level that was within 3 vertebral levels of the level of compression demonstrated on MRI.
Further, pain (both midline back pain and radicular pain) was also a poor predictor of the level of compression.
Finally, of the 187 patients who had plain radiographs at the level of compression at referral, 60 showed vertebral collapse suggesting cord compression, but only 39 of these predicted the correct level of compression (i.e. only 20% of all radiographs correctly identified the level of compression).
The authors note that frequently only the lumbar spine was XR at the time of clinical presentation (usually at the referring hospital), presumably due to false localizing signs and a low awareness on the part of clinicians that most MSCC occurs in the thoracic spine (68% in this series).
Knee Pain Injuries are Radiographs needed?
Many people know that the folks in Ottawa have come up with a rule to determine whether radiographs are needed in patients complaining of knee pain. The Ottawa Knee rules that that radiographs are only required for knee injuries with any of the following:
• Age 55 years or older
• isolated tenderness of patella
• tenderness at head of fibula
• inability to flex to 90'
• inability to bear weight both immediately and in the emergency department (4 steps)
Well another group in Pittsburgh have their own set of rules that were recently shown to be more specific with equal sensitivity. The Pittsburgh decision rules state that radiographs are only needed if
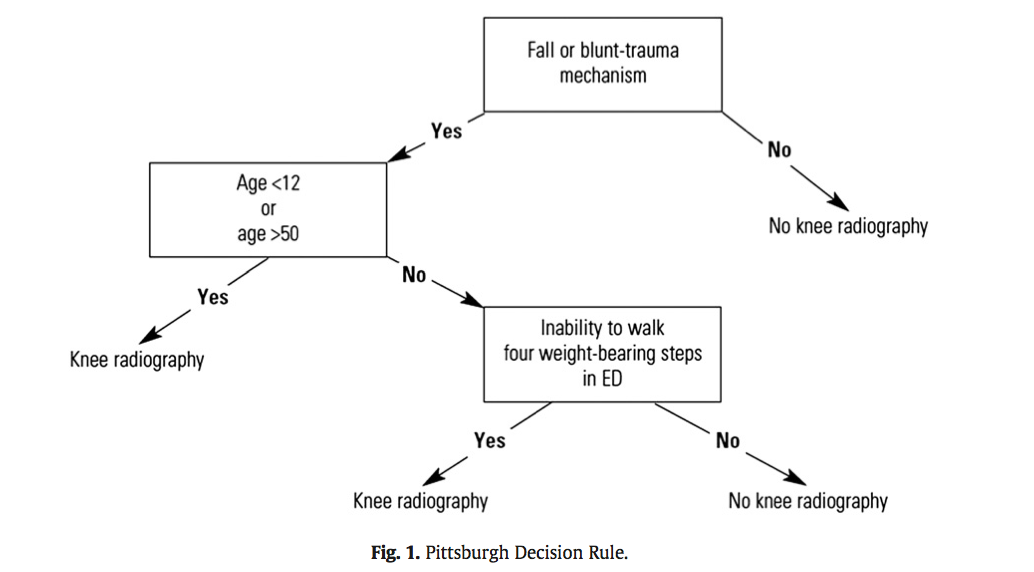
So consider using the Pittsburgh or Ottawa Knee rules the next time you have a patient with knee pain to determine if those radiographs are really needed.
The full article can be found at http://www.ajemjournal.com/article/S0735-6757%2812%2900566-9/abstract
Scapular fractures
Key components in the determination of return to play following concussion include assessment of 1) brain function, 2) reaction time and 3) balance testing
Balance testing has become increasingly utilized in the diagnosis and management of sports related concussion. Studies have identified temporary or permanent deficits in static and/or dynamic balance in individuals with mild-to-moderate traumatic brain injury and sports related concussion. An example of this is the Balance Error Scoring System (BESS). Three stances are testing (narrow double-leg stance, single leg stance and a tandem stance) with the hands on the hips and eyes closed for 20 seconds. The FNL Sideline Concussion Assessment Tool utilizes a modified BESS. Example video below:
http://www.youtube.com/watch?v=xtJgv-D7IdU
Just before you upgraded your old computer, recall what happened when you had Excel, Word and PowerPoint all open at the same time. In the concussed state, the brain is essenatially functioning like your old computer... and the more tasks it must perform, the slower it will work and slower it will recover. Hence the concept of cognitive rest. Below is taken from the AMSSM position statement of concussion in sport.
Return to school
There are no standardized guidelines for returning the injured athlete to school. If the athlete develops increased symptoms with cognitive stress, student athletes may require academic accommodations such as a reduced workload, extended test-taking time, days off or a shortened school day.
Some athletes have persistent neurocognitive deficits following a concussion, despite being symptom free. Consideration should be made to withhold an athlete from contact sports if they have not returned to their ‘academic baseline’ following their concussion (level of evidence C).
The CDC developed educational materials for educators and school administrators that are available at no cost and can be obtained via the CDC website. Additional resources for academic accommodations should be developed for both clinicians and educators (level of evidence C).
Adam Friedlander shared the practical application of this which I found amusing:
" I always recommend what Peds neuro called "a brain holiday" - my favorite part. All of our nurses look at me like I'm nuts, but it is now on our official concussion/CHI DC instructions. I always say to the kiddo: "You'll love this part. No homework, no reading." Then I turn to mom and dad and tell them they'll love the next part: "No TV, no video games."
Thank you for sharing Adam!!
Estimated 3.8 million sport-related concussions per year (likely significantly higher due to underreporting)
Most patients recover within a 7-10 day period
** Children and teenagers require more time than college and professional athletes
This "accepted" time for recovery is not scientifically established and there is a large degree of variability based on multiple factors including age (as above), sex & history of prior concussions
Approximately 10% of athletes have persistent signs and symptoms beyond 2 weeks (which may represent a prolonged concussion or the development of post-concussion syndrome)
During this time the patient should have complete rest from all athletic activities, close follow-up with PCP and be educated re concussions.
If practical, "cognitive rest" should also be prescribed. This is one of the most frequently neglected aspects of post-concussion care and will be discussed in a future pearl.
Hematoma Block
Provides good aesthesia for reduction of fractures. Onset in approximately 5 minutes
Benefits: No need for NPO, simple and easy to perform & can be done without additional personnel (unlike w/ procedural sedation)
Contraindications: Open fractures, dirty or infected overlying skin
1) Identify fracture site with x-ray and palpation
2) Clean skin w/ Betadine
3) Insert needle into the hematoma. * Confirm placement by aspirating blood *
4) Inject anesthetic (lidocaine 1 or 2%) into the fracture cavity and adjacent periosteum
http://www.youtube.com/watch?v=tjnsdjfwMmY
"When can my child get back out on the field doc?"
Return to play
▸ Concussion symptoms should be resolved before returning to exercise.
▸ A RTP progression involves a gradual, step-wise increase in physical
demands, sports-specific activities and the risk for contact.
▸ If symptoms occur with activity, the progression should be halted and
restarted at the preceding symptom-free step.
▸ RTP after concussion should occur only with medical clearance from a
licenced healthcare provider trained in the evaluation and management
of concussions.
Short-term risks of premature RTP
▸ The primary concern with early RTP is decreased reaction time leading
to an increased risk of a repeat concussion or other injury and
prolongation of symptoms.
Long-term effects
▸ There is an increasing concern that head impact exposure and
recurrent concussions contribute to long-term neurological sequelae.
▸ Some studies have suggested an association between prior concussions
and chronic cognitive dysfunction. Large-scale epidemiological studies are
needed to more clearly define risk factors and causation of any long-term
neurological impairment.
Metacarpal Neck Fractures (i.e.: Boxer’s Fracture if 5th Metacarpal)
Depending on the MCP joint involved a certain amount of angulation is permissible before it adversely affects normal function.
Wishing everybody a Happy and Healthy New Year.
NSAIDs are commonly used by professional and recreational athletes to both reduce existing and/or prevent anticipated exercise induced musculoskeletal pain
NSAIDs have potential hazardous effects on the gastrointestinal (GI) mucosa during strenuous physical exercise
Potential effects include mucosal ulceration, bleeding, perforation. and short-term loss of gut barrier function in otherwise healthy individuals
Intense exercise by itself has previously been shown to induce small intestine injury
Human intestinal fatty acid binding protein (1-FABP) is a protein found in mature small bowel enterocytes which diffuses into the circulation upon injury
Ibuprofen and endurance exercise (cycling) independently result in increased 1-FABP levels
When occurring together, ibuprofen ingestion with subsequent exercise causes significantly increased small bowel injury and intestinal permeability
Small bowel injury was found to be reversible in 2 hours
Taking empiric NSAIDs before endurance exercise may be an unhealthy practice and should be discouraged in the absence of a clear medical indication
Are discharged patients who suffer minor thoracic injury at risk of developing delayed pneumonia?
Prospective study of 1,057 patients age 16 and older with minor thoracic injury who were discharged from the ED.
32.8% had at least one rib fracture
8.2% had asthma
3.4% had COPD
Only 6 patients developed pneumonia!!
Sex, smoking, atelectasis on CXR, and alcohol intoxication were not significantly associated with delayed pneumonia.
However, for patients with preexistent pulmonary disease (asthma or COPD) AND rib fracture, the relative risk of delayed pneumonia was 8.6. Patients without either of these conditions are at extremely low risk of future development of pneumonia.
Hematoma blocks for distal radius fractures
Hematoma blocks provide safe, effective analgesia without an increased risk of post procedural infections when compared with other regional blocks
Provide equal reduction quality AND pain control as procedural sedation with Propofol.
However, mean time to reduction (0.9 vs. 2.6 hours) and time to discharge post procedure (0.74 vs. 1.17 hours) were reduced with hematoma blocks.
Consider this option next time the department is busy or the patient is not an ideal procedural sedation candidate.
Tarsal Tunnel Syndrome (TTS)
Prior pearls have addressed Carpal Tunnel Syndrome and Cubital Tunnel Syndrome, which affect the median and ulnar nerves, respectively. Tarsal tunnel syndrome, is a similar compression neuropathy of the tibial nerve as it transverses through the tarsal tunnel of the foot.
The tarsal tunnel is located behind the medial malleolus, and is where the posterior tibial artery, tibial nerve and several tendons transverse. Patients will present complaining of numbness of the foot radiating into Digits 1-4, pain, burning , and tingling of the base of the foot and heel. TTS has many causes and is more common in athletes.
Consider the diagnosis in patients with foot pain and numbness. If interested in more information about TTS please consider reading this eMedicine article, http://emedicine.medscape.com/article/1236852-overview
Injury is often caused by sudden dorsiflexion on a plantar flexed foot w/ the knee in extension or similarly sudden knee extension with the ankle in a dorsiflexed position.
Injury has a predilection for the poorly conditioned middle-aged athlete, with "thick calves" who are engaged in strenuous activity
Strains are treated with ice, analgesics, and compression (decreases hematoma size and facilitates healing)
Also, consider casting/splinting as dictated by injury severity, such as with a night splint or a CAM boot.
Severe strains and ruptures can be splinted in plantar flexion for 3 weeks.
Distal radius fractures are common in children
Traditional management includes closed reduction +/- procedural sedation
The downside of this approach includes: patient risks, cost, physician time, ED bed time and tying up resources.
Kids have excellent bone remodeling potential...displaced and angulated fractures heal well without reduction
Crawford et al - 51 children aged 3 to 10 (avg 6.9 yrs) w/closed distal radius fractures.
Exclusions: open or growth plate fractures, metabolic bone disease or neurovascular injury.
No sedation, analgesia or fracture reduction was performed
Treatment: simple casting and gentle molding to correct angulation... i.e. fractures were left in a shortened, overriding position
Outcome: All patients had clinical and radiographic union and full range of motion of the wrist at one year w/ good patient (parent) satisfaction. This was associated w/ significant cost savings.
Consider this approach in consultation with orthopedist
Remember exclusions: open fractures, fracture dislocations, growth plate injuries and neurovascular injury.
Children w/ excessive angulation or rotational deformity should have standard care (closed reduction w/ sedation)
Multiple guidelines exist for "excessive angulation" but as a general rule
Age < 5 Up to 35 degrees
Age 5- 10 Up to 25 degrees
Age >10 Up to 20 degrees