Settings: systemic review and meta-analysis
Participants: 2 RCTs, 21 observational studies. Fifteen studies were published between 2020-2023.
There was a total of 25721 patients with septic shock
Outcome measurement: Primary outcome was short-term mortality (ICU, hospital, 28-day, 30-day). Secondary outcomes included ICU LOS, Hospital LOS, time to achieve MAP > 65 mm Hg,
Study Results:
Composite outcome of short term mortality:
Secondary outcome:
Discussion:
Conclusion:
More and more studies, although a RCT is still necessary, are showing that early initiation of vasopressor within 1-6 hours of septic shock would be more beneficial to patients with septic shock.
For the folks who have been in practice for a while, you may be aware of the roller-coaster evidence base looking at steroids for pneumonia. Once thought to be beneficial and clearly indicated, of late steroids for pneumonia have fallen out of favor. Hamad et al have published an excellent (and brief) review in Clinical Infectious Diseases which suggests the pendulum might be swinging back in favor of giving steroids to patients with pneumonia. It's a ~5 minute read, so I recommend glancing through it yourself, but below are my two cents (solely my opinion) on where we are with steroids for pneumonia.
Take Home Points (OPINION ALERT):
1) When you have a condition present that you consider an indication for steroids (e.g. severe COVID-19 for sure; septic shock, s. pneumo infection, and ARDS depending on how you feel about the existing literature) --> strongly consider giving steroids unless there's a contraindication
2) When you have an undifferentiated patient who MAY have one of these conditions (e.g. pneumonia with COVID pending, patient potentially in ARDS or high risk of going into ARDS, etc) who is very sick --> it is reasonable to give steroids (if no contraindication) or not give steroids. My tendency is to lean towards giving steroids in these cases, but do be aware that society guidelines recommend against steroids here (although debatable if they just haven't caught up to more recent literature)
3) When you have an undifferentiated patient who may have one of these conditions, but is NOT very sick --> I do not think there is significant enough evidence to support empiric steroids
4) Factors that might push you one way or another:
IV Fluid Resuscitation
Settings: Retrospective study of a national inpatient database (Japan).
Participants:
Outcome measurement: Primary outcome was in-hospital mortality, after propensity score matching.
Study Results:
Discussion:
Conclusion:
Risk-stratifying patients according to SOFA score is a potential strategy for appropriate admission strategies.
Bottom line: As part of a systematic protocol, peripheral pressors administered through a peripheral line greater 22Ga or larger reduced the number of days of central venous catheter (CVC) use in a MICU population at an academic medical center. 35 (5.5%) patients had an extravasation event all with “minimal” tissue injury complications. None required surgery. 51.6% of patients did not require a CVC as a result of the protocol
Details
Notes on protocol
PIV were placed and confirmed with US, were between wrist and AC fossa with q2h patency checks. Max allowable dose of NE 15 mcg/min with requirement that patients be able to report pain at site. Initially, max infusion time was set at 48h but was eventually liberalized to indefinite use.
The BRASH syndrome (Bradycardia, Renal failure, AV nodal blockade, Shock, Hyperkalemia) has been increasingly described in the literature in the past 3-5 years.
The inciting factor is generally considered to be something that prompts acute kidney injury, often hypovolemia of some sort. Rather than AV nodal blocker overdose or severe hyperkalemia causing conduction problems, the combination of AV nodal blocker use (most often beta-blockers, but can be any type) and hyperkalemia (often only moderate) has a synergistic effect on cardiac conduction with ensuing bradycardia that can devolve into a cycle of worsening renal perfusion and shock.
Treatment is supportive, but most effective when the syndrome is recognized and all parts simultaneously managed. ED physicians should be familiar with its existence for targeted whole-syndrome stabilization and to avoid diagnostic delay.
When patients fail simple respiratory support therapies like nasal cannula or non-rebreather, it is often a point of debate whether to move next to High Flow Nasal Cannula (HFNC) or Noninvasive Positive Pressure Ventilation (NIPPV). This study randomized patients in acute respiratory failure (ARF) to CPAP, a form of NIPPV, vs HFNC. They looked at all comers in ARF, and primary outcome was need for intubation. Importantly, they excluded asthma/COPD exacerbation, for which BiPAP is typically considered the first line therapy due to improved CO2 clearance.
They found a significantly lower number of patients required intubation in the CPAP (28.9%) group than the HFNC (42.6%) group (p=0.006). They hypothesized that the enhanced PEEP improved oxygenation (hypoxia being a common trigger for moving to intubation), but as opposed to BiPAP, the lack of additional driving pressure limited tidal volumes and Patient Self-Inflicted Lung Injury (P-SILI), which is a known mechanism of ARDS and mortality. They use this argument to explain why trials like FLORALI, pitting HFNC vs BiPAP, tend to not find an advantage for the NIPPV arm. While this rationale makes sense, it should be noted that the study does not directly investigate if this was the reason for the difference, and for what its worth the inverse argument that using driving pressure to reduce respiratory rate, hypercarbia, and work of breathing (other very common indications for intubation) would also theoretically reduce intubations. Furthermore, it's not clear why reducing P-SILI, which tends to cause mortality on a much longer duration, would improve the short-term outcome of need for intubation.
Bottom Line: This study demonstrated a benefit to CPAP over HFNC in terms of decreasing need for intubation amongst non-asthma/non-COPD patients with acute respiratory failure, and offered a physiologic rationale but one that requires further verification and discussion. While it may be reasonable to choose CPAP instead of HFNC in marginal patients at risk of intubation (but stable enough to trial noninvasive support first), in my opinion more studies are likely needed before a wholesale change in practice. The study also does not take into consideration the enhanced comfort and compliance we tend to see with HFNC over NIPPV, which should be considered as well.
Pearls for the Patient in Cardiogenic Shock
Settings: Single ICU in Poland, randomized trial
Participants: intubated patients who needed arterial catheter placement. Patients who had adequate access to one axillary and one femoral artery were eligible.
Patients were randomized 1:1 for axillary or femoral artery cannulation.
Outcome measurement: Primary outcome was cannulation success rate. Secondary outcomes were first pass success rate, number of attempts.
Study Results:
Discussion:
Conclusion:
Ultrasound-guided cannulation of the axillary artery via the infraclavicular route is non-inferior to the cannulation of the common femoral artery. When cannulation of the radial or femoral artery is not available, we can consider axillary artery via the infraclavicular approach.
Background:
There has been interest in vitamin C as an adjunctive therapy in patients with systemic inflammation and vasoplegia to reduce inflammation. While it was suggested that vitamin C may have some benefit (along with hydrocortisone and thiamine) in septic shock, the LOVIT trial showed possible harm from high-dose vitamin C administration in septic ICU patients. The VALENCIA trial sought to evaluate whether vitamin C could reduce the duration of vasopressor therapy in patients with moderate vasoplegic shock.
Study:
-double-blinded RCT at two tertiary centers, 71 patients (36 to placebo, 35 to vitamin C)
-adult patients with vasoplegic shock of any cause
-vasopressor requirement >10 μg/min of norepi after hypovolemia was excluded
-notable exclusion criteria: end-stage renal failure and expected survival <12 hrs
Results:
-65 pts with septic shock, 6 pts with non-infectious cause
-no significant difference in the duration of vasopressors between the treatment group (median, 44 h [95% CI, 37-54 hrs]) and the control group (55 hrs [95% CI, 33-66 hrs])
-also no statistically significant difference in the vasopressor dose at 12 hourly time points, ICU or 28-day mortality and ICU or hospital length of stay
Take-home points:
Small study that ultimately may be under-powered but did not show that vitamin C reduces vasopressor duration in moderate vasoplegic shock
Targeted Therapeutic Mild Hypercapnia after Resuscitated Cardiac Arrest (TAME)
Current guidelines recommend normocapnia for out-of-hospital cardiac arrest (OHCA), the TAME Study asked is mild hypercapnia better?
Conclusion: "In patients with coma who were resuscitated after out-of-hospital cardiac arrest, targeted mild hypercapnia did not lead to better neurologic outcomes at 6 months than targeted normocapnia."
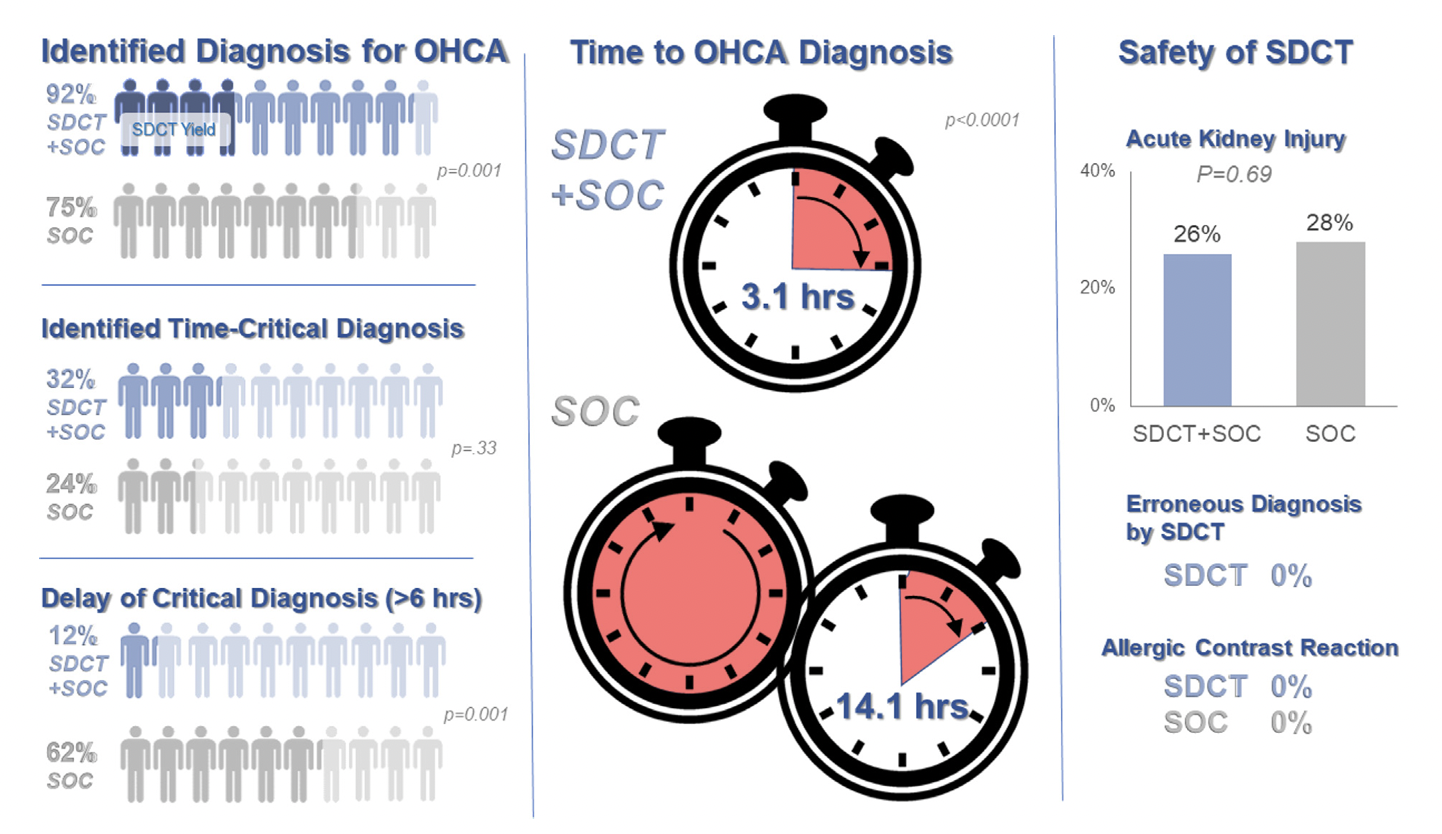
Background: Prior evidence1,2 has suggested that early “pan-scan” after ROSC provides clinically-relevant information that assists in the care of the patient in question, when the cause of OHCA is unclear.
The recent CT FIRST trial looked at patients pre- and post- implementation of a protocol for head-to-pelvis CT within 6 hours of ROSC for adult patients without known cause or evidence of possible cardiac etiology, stable enough for scan. *Patients with GFR <30 were excluded from assignment to CT, although were included in the post/CT cohort if their treating doctors ordered CT scans based on perceived clinical need. To balance this, a similar number of patients with GFR <30 were included in the pre/“standard of care” cohort.
Outcomes After Protocol (Pre- vs. Post-):
Bottom Line: Early pan-CT allows for earlier definitive diagnosis and stabilization without increase in adverse events. While this earlier diagnosis does not seem to yield better survival, earlier stabilization may provide some benefits in terms of resource allocation and disposition, a notable benefit during our current crisis of staffing shortages and ED boarding.
Central Venous Catheter (CVC; aka central line) placement is a common procedure in both the ED and ICU, and while overall quite safe, does carry some risk. In particular, many of us regularly are confronted with the challenge of placing a line in a patient with profound thrombocytopenia, which can result in significant bleeding. In these cases, should we give platelets before we place the line?
Van Baarle et al published a randomized study in NEJM comparing an empiric 1u platelet transfusion vs no transfusion in patients with a platelet count of 10,000-50,000, prior to line placement. The study included both HD and non-HD (e.g. TLC) lines, from all three major access sites, in patients in their ICU or hematology ward. They found statistically fewer serious bleeding events in the transfusion group (4.8%) vs no transfusion group (11.9%). The study wasn't powered to look at more patient oriented outcomes like mortality, but I'm sure we can all agree less bleeding is probably a good thing. Also importantly, this study did not evaluate the risks/benefits of delaying line placement to obtain platelets when the line is urgently needed, so I would not recommend extending this to conclude platelets must be given before line placement if the line is needed for something highly time-sensitive (e.g. only available access to infuse pressors in a hypotensive patient).
Bottom Line: It is probably beneficial and appropriate to provide prophylactic platelet transfusion prior to CVC placement in patients with a platelet count less than 50,000, assuming circumstances allow.
Settings: Retrospective data from 3 Dutch EDs (development of the score), 2 Denmark ED (for validation of the score). The novel score (International Early Warning Score) will be composed of the National Early Warning Score (NEWS) + Age +Sex
Components of the National Early Warning Score:
Participants: All adult patients in the Netherlands Emergency department Evaluation Database (NEED) and Danish Multicenter Cohort (DMC).
Outcome measurement: in-hospital mortality, including death in EDs.
Study Results:
Discussion:
Conclusion:
This multicenter study showed that IEWS perform better than the NEWS for predicting in-hospital mortality for ED patients.
Prophylactic antibiotic use in cirrhotic patients with an upper GI bleed has been demonstrated to have a mortality benefit in multiple randomized clinical trials. Some trials as well demonstrated a decreased risk of rebleeding as well as a shorter hospital length of stay (1,2).
The exact means of protection is not entirely clear and its benefit is seen in both variceal and nonvariceal hemorrhages as well as in cirrhotic patient both with and without ascites.
There does appears to be a close interplay between cirrhosis bleeding risk and infection, with infection being a common precipitating factor for upper GI bleed.
The antibiotic of choice is ceftriaxone 1 gram IV daily for seven days. Although in case of allergy/intolerance, fluoroquinolones or aminoglycosides may be used as alternatives (3).
Bottom line:
All forms of upper GI hemorrhage in cirrhotic patients warrant prophylactic antibiotic use (regardless of the presence of ascites) as well as a diligent search and exclusion of possible infectious sources.
Background: In general practice, platelets are typically transfused for invasive procedures when the platelet count falls below 50 x 109/L. Regarding the placement of central venous catheters (CVCs), there is minimal data to support or refute decisions to transfuse platelets in these patients, although the 2015 Clinical Practice Guideline from the AABB (formerly, the American Association of Blood Banks) recommends deferring platelet transfusion until a platelet count of 20 x 109/L for CVC placement [weak recommendation, low quality evidence].1
In a study published this month in NEJM,2 van Baarle et al. performed a multicenter randomized controlled noninferiority trial comparing platelet transfusion to no transfusion in patients with platelets 10 to 50 x 109/L prior to US-guided CVC insertion. The primary outcome was the occurrence of catheter-related bleeding Grades 2-4 (Grade 1 = oozing; managed with <20 min of manual compression, not requiring RBC transfusion, & Grades 2-4 is everything else up to death) within 24 hours post-procedure.
Bottom Line: The jury is still out on best platelet transfusion practices prior to CVC placement, but I would strongly consider prophylactic platelet transfusion in patients with platelets < 30 x 109/L, those with underlying hematologic malignancy, and patients receiving larger CVCs such as dialysis lines. How much to transfuse in those with more severe thrombocytopenia is uncertain.
Separately, I would also strongly recommend use of US-guidance for any CVC placement in this population as well, based on practical common sense and some supportive literature as well.5
Ability to move the head and neck freely can be clutch in endotracheal intubation, so in patients such as certain trauma patients who may have c-spine instability and need to be immobilized, it's all the more important to choose the optimal intubation approach to maximize success and minimize head movement.
Choi et al recently published a study in Anesthesia looking at:
-Video laryngoscopy with a standard geometry Mac blade
vs
-Fiberoptic intubation
as the initial method for intubating patients in c-collars about to undergo spinal surgery. This is an interesting contrast between two extremes, as standard geometry is the most "traditional" approach, whereas fiberoptic is kind of the opposite end of the spectrum, jumping to a more advanced method which might be more flexible (no pun intended) but also introduces new complexities.
All outcomes actually favored standard geometry VL over fiberoptic, including first pass success (98% vs 91%), time to intubation (50s vs 81s) and need for additional airway maneuvers (18% vs 56%). There was no difference in complication rates, although a bigger study might be needed to find rare complications (this study had 330 patients).
In my opinion, it's unfortunate they didn't include hyperangulated VL, as it would be interesting to see how this approach compares. Personally I think of hyperangulated VL in these patients as a nice blend of the two methods, bringing the familiarity and speed of typical VL intubation, but often requiring less neck movement like fiberoptic.
Bottom Line: This study does not support a fiberoptic first approach to intubating patients with cervical spine instability. In fact, it may cause harm.
Bicarbonate Use for Lactic Acidosis?