Identifying Critically Ill Cancer Patients in the ED
The most recent AHA guidelines for goal blood pressure after return of spontaneous circulation (ROSC) post-cardiac arrest recommend a definite mean arterial pressure (MAP) goal of > 65 mmHg.1 There is no definitive data to recommend a higher specific goal, but there is some evidence to indicate that maintaining higher MAPs may be associated with better neurologic outcomes.2
A recently published prospective, observational, multicenter cohort study looked at neurologic outcomes corresponding to different MAPs maintained in the initial 6 hours post-cardiac arrest.3
Findings:
1. Compared to lower blood pressures (MAPs 70-90 mmHg), the cohort with MAPs > 90 mmHg had:
2. The association between MAP > 90 mmHg and good neurologic outcome was stronger among patients with a previous diagnosis of hypertension, and persisted regardless of initial rhythm, use of vasopressors, or whether the cardiac arrest occured in or out of hospital.
3. There was a dose-response increase in probability of good neurologic outcome among all MAP ranges above 90 mmHg, with MAP >110 mmHg having the strongest association with good neurologic outcome at hospital discharge.
Note: The results of a separate trial, the Neuroprotect post-CA trial, comparing MAPs 85-100 mmHg to the currently recommended MAP goal of >65 mmHg, are pending.4
Bottom Line: As per current AHA guidelines, actively avoid hypotension, and consider use of vasopressor if needed to maintain MAPs > 90 mmHg in your comatose patients post-cardiac arrest, especially those with a preexisting diagnosis of hypertension.
We know that high flow nasal cannula is an option in the management of acute hypoxic respiratory failure without hypercapnea. A newer iteration of high flow, "high velocity nasal insufflation" (HVNI), may be up-and-coming.
According to its makers (Vapotherm), it is reported to work mainly by using smaller bore nasal cannulae that deliver the same flows at higher velocities, thereby more rapidly and repeatedly clearing dead space, facilitating gas exchange and potentially offering ventilatory support.
In an industry-sponsored non-inferiority study published earlier this year:
Bottom Line:
The availability of a nasal cannula that helps with CO2 clearance would be great, and an option for patients who can't tolerate the face-mask of NPPV would be even better.
HVNI requires more investigation with better studies and external validation before it can really be considered noninferior to NPPV, but it certainly is interesting.
Sedating Mechanically Ventilated Patients
The recently published BICAR-ICU study looked at the use of bicarb in critically ill patients with severe metabolic acidemia...
Bottom Line:
Consider administration of sodium bicarbonate for your critically ill ED patients with severe metabolic acidosis and AKI, especially if acidosis &/or renal function is not improved with usual initial measures (such as IVF, etc).
*Acute Kidney Injury Network Staging Criteria

Does Lactated Ringer's Raise Serum Lactate?
Critical Post-Arrest Interventions
The highly-awaited PARAMEDIC2 trial results are in:
Interestingly, the authors also queried the public as to what mattered to them most:

Bottom Line:
Respiratory alkalosis is the most common acid-base disturbance in acute severe asthma.
Lactic acidosis is also extremely common, developing in up to 40%. This may be related to:
- tissue hypoxia
- increased respiratory muscle usage related to work of breathing
- beta agonist therapy
The first report of beta agonist administration associated with hyperlactatemia was in 1981 in patients treated for preterm labor with terbutaline. Since then, numerous case reports and studies have linked IV and inhaled beta agonist administration with the development/worsening of lactic acidosis in severe asthmatics in the ICU and in the ED.
The exact mechanism is unclear, but is thought to be related to adrenergic stimulation leading to increased conversion of pyruvate to lactate.
In a study published in Chest in 2014, investigators evaluated plasma albuterol levels and serum lactate levels, as well as FEV1.
They found plasma albuterol levels correlated with lactate concentration and maintained significant association after adjusting for asthma severity (suggesting the association was independent of work of breathing/respiratory muscle usage).
Furthermore, several reports have suggested that dyspnea may improve in patients with elevated lactate and acidosis after beta agonists are withheld.
Take Home Points:
- Beta agonist therapy may contribute to lactic acidosis.
- Lactic acidosis may contribute to respiratory distress.
- In patients on prolonged, high-dose beta agonist therapy, consider checking a serum lactate periodically. If elevated, consider whether worsening lactic acidosis is contributing to respiratory distress and contemplate transitioning to less frequent treatments.
-Patients with severe asthma exacerbation and elevated serum lactate must have thorough evaluation for true tissue hypoxia/hypoperfusion. **Beta agonist associated hyperlactatemia should be a diagnosis of exclusion.**
Improving Analgesia in Mechanically Ventilated ED Patients
When a do-not-intubate (DNI) hospice patient arrives in the ED with respiratory distress, consideration of non-invasive positive pressure ventilation (NIPPV) could invoke either a “What other option do I have?” or “Why torture the patient and prolong the dying process?” sentiment.
But what’s the data?
A recently-published meta-analysis1 found that in DNI patients receiving NIPPV, there was a 56% survival rate to hospital discharge and 32% survival to 1-year.
Independent studies have demonstrated:
Bottom Line:
Legionella is an important cause of community-acquired pneumonia. It ranks among the three most common causes of severe CAP leading to ICU admission and carries a high mortality rate – up to 33%. Resulting from inhalation of aerosols containing Legionella species and subsequent lung infection, it is often associated with contaminated air conditioning systems, and other hot and cold water systems.
Recommended antibiotic regimens include a fluoroquinolone, either in monotherapy or combined with a macrolide (typically Levaquin +/- or Azithromycin).
A retrospective, observational study published in the Journal of Antimicrobial Chemotherapy in 2017 looked at 211 patients admitted to the ICU with confirmed severe legionella pneumonia treated with a fluoroquinolone vs a macrolide and monotherapy vs combination therapy. Combination therapy included fluoroquinolone + macrolide, fluoroquinolone + rifampicin, or macrolide + rifampicin.
Of these 211 cases, 146 (69%) developed ARDS and 54 (26%) died in the ICU. Mortality was lower in the fluoroquinolone-based group (21%) than in the non-fluoroquinolone based group (39%), and in the combination therapy group (20%) than in the monotherapy group (34%). In a multivariable analysis, fluoroquinolone-based therapy, but not combination therapy was associated with a reduced risk of mortality (HR 0.41).
Take Home Points:
-Remember, our usual blanket coverage with vanc + zosyn in the ED does not cover atypicals!
-Consider Levaquin instead of Azithro if there is clinical concern for Legionella PNA
-hyponatremia, abnormal LFTs may be clues in the appropriate context
Volume Responsiveness, Carotid Ultrasound, and the PLR
Although not specifically a part of current recommendations due to lack of data, the AHA has previously recommended shifting upward on the sternum during CPR in the pulseless pregnant patient in order to account for upward displacement of the heart by a gravid uterus. Should the same be done for our obese patients?
Lee et al. performed a retrospective study that reviewed chest CTs to determine the location on the sternum that corresponded to the optimal point of maximal left ventricular diameter (OPLV), in both obese and non-obese patients.
They found that the OPLV was higher (more cranial) on the sternum for obese patients than for patients with normal weight, although 96% of obese patients' OPLV fell within 2cm of where the guidelines recommend standard hand placement should be, compared to a notable 52% in non-obese patients.
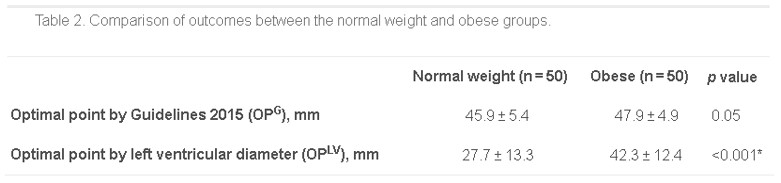
*as measured from the distal end of the sternum
Bottom Line: Radiographically, the location on the sternum that corresponds to optimal compression of the LV is more cranial in obese patients than in non-obese patients. It remains to be seen whether the recommendations for hand placement in CPR should be adjusted, but we may want to consider staying within 4cm of the bottom of the sternum in patients of normal weight.


Take Home Points:
Precedex (dexmedetomidine) is a selective alpha-2 adrenergic receptor agonist used as a sedative.
It is unique among sedatives typically used in the ICU in that it lacks GABA activity and lacks anticholinergic activity.
Previous studies have shown significant positive changes in sleep patterns in critically ill patients sedated with dexmedetomidine:
-improved sleep efficiency – decreased sleep fragmentation, decreased stage 1 sleep, increased stage 2 sleep
-improved distribution of sleep (with more than ¾ sleep occurring at night)
Given importance of sleep and preservation of day-night cycles/ circadian rhythms in prevention of delirium, a recent randomized controlled trial evaluated dexmedetomidine's effect on delirium.
100 delirium-free critically ill adults receiving sedatives were randomized to receive nocturnal (21:30-06:15) IV dexmedetomidine (titrated to RASS -1 or max 0.7 mcg/kg/hr) OR placebo until ICU discharge.
80% of patients in the dexmedetomidine group remained delirium-free vs 54% in the placebo group.
There was no difference in the incidence of hypotension, bradycardia, or both between groups.
DOACs and the Critically Ill
ED physicians frequently utilize modailities such as noninvasive positive pressure ventilation (NIV) and high flow nasal cannula (HFNC) to support and potentially avoid intubation in patients presenting with acute hypoxic respiratory failure. Unfortunately, failure of these measures, resulting in "delayed" intubation, has been associated with increased mortality.1,2
A recent post-hoc analysis of data from a multicenter randomized controlled trial evaluated 310 patients with acute hypoxic respiratory failure managed with supplemental O2 by regular nasal cannula, HFNC, or NIV.3
The following factors were predictive of eventual intubation in the different groups:
Of note, 45% of the 310 patients eventually required intubation, and these patients in general had a higher initial respiratory rate and lower PaO2 at presentation, and were more likely to have bilateral infiltrates on CXR.
Bottom Line: Reevaluate your patients frequently. If RR remains high, P:F ratio remains low, or patient respiratory effort/work of breathing is not alleviated by noninvasive measures, consider pulling the trigger on intubation earlier.
Linezolid, an antimicrobial agent in the oxazolidinone class, often used to cover MRSA and/or VRE, is a reversible MAOI that increases the risk of serotonin syndrome, particularly when administered with other serotonergic agents.
In 2011, the US FDA issued a warning against concomitant use of Linezolid and other serotonergic agents, particularly SSRIs and SNRIs. When use of linezolid is absolutely indicated, an appropriate washout period prior to initiation was recommended.
Based on published reports and retrospective reviews, the incidence of linezolid-associated serotonin toxicity is between 0.54% and 18.2%.
A study published in the Journal of Clinical Psychopharmacology in Oct 2017 examined the incidence of serotonin syndrome with combined use of linezolid and SSRIs/SNRIs compared with linezolid alone and though there was a trend toward increased incidence in patients on SSRI/SNRIs, the authors were unable to find a statistically significant difference.
Several flaws:
-Study was retrospective
-Incidence of serotonin syndrome in both groups was very low: 1/87 (1.1%) in Linezolid + SSRI/SNRI group compared to 1/261 (0.4%) in Linezolid alone group.
-Patients in “Linezolid alone” group were not on SSRIs or SNRIs, but were allowed to be on other serotonergic medications.
Despite this study, there are many (>30) case reports of Linezolid-associated serotonin syndrome in patients taking other serotonergic agents.
Cyproheptadine (the “antidote”) is an H1 antagonist and nonspecific serotonin antagonist. A single case study published in 2016, reported successful use of cyproheptadine for prophylaxis against serotonin toxicity in a patient with schizophrenia, depression, and severe osteomyelitis requiring treatment with linezolid while on fluoxetine.
Bottom Line:
Risk of linezolid-associated serotonin syndrome may be lower than previously thought, however, it is still not recommended for use in patients taking concomitant serotonergic agents without an appropriate washout period.
In case of resistant infection with no other antibiotic treatment options, the risks and benefits of concomitant administration must be weighed seriously and providers must familiarize themselves with and be vigilant in watching for signs/symptoms of serotonin toxicity.
In situations where use of linezolid is unavoidable in patients on concomitant serotonergic agents, prophylactic cyproheptadine may be considered.
Acute on Chronic Liver Failure