Background: The use of steroids in pneumonia has long been controversial with conflicting data, and the recent ESCAPe randomized controlled trial by Meduri et al. showing no mortality benefit with their use, but likely underpowered due to recruitment issues. The recently published CAPE COD study by Dequin et al. may change the game.
Design: Double-blind, placebo-controlled, multicenter, RCT
Intervention: Early hydrocortisone within 24 hrs, 200mg/day x 4-8 days depending on improvement, then preset taper
Primary outcome: Death at 28 days
Secondary outcomes:
Bottom Line: The addition of hydrocortisone to antibiotics in severe CAP may decrease need for intubation and development of shock, and in this well-done study, decreased 28 and 90-day mortality.
Background: The use of sodium bicarbonate in the treatment of out-of-hospital cardiac arrest (OHCA) has been longstanding despite conflicting data regarding its benefit, outside of clear indications such as toxic ingestion or hyperkalemic arrest.
Study: A recent retrospective cross-sectional study by Niederberger et al.1 examined prehospital EHR data for ALS units responding to nonpregnant adults with nontraumatic OHCA, noting use of prehospital bicarb and the outcomes of 1) ROSC in the prehospital encounter and 2) survival to hospital discharge. They created propensity-matched pairs of bicarb and control patients, with a priori confounders: age, sex, race, witnessed status, bystander CPR, prearrival instructions, any defibrillation attempt, use of CPR feedback devices, any attempted ventilation, length of resuscitation, number of epi doses.
There were 23,567 arrests (67.4% asystole, 16.6% PEA, 15.1% VT/VF), 28.3% overall received sodium bicarb.
Results:
In the propensity-matched sample, survival was higher in bicarb group (5.3% vs. 4.3%; p=0.019).
There were no differences in rate of ROSC overall, but looking at the different rhythms, ROSC was higher in the bicarb group with asystole as the presenting rhythm (bicarb 10.6 vs 8.8%; p=0.013) but not PEA or VT/VF.
*There is no indication by the authors as to the dosing of bicarb most associated with survival to hospital discharge (or ROSC in asystole) in the study, however a previous study has indicated that a single amp of bicarb is unlikely to significantly improve severe metabolic acidosis (pH <7.1),2 so the general recommendation of at least 1-2mEq/kg should be employed.
Bottom Line: The use of sodium bicarb may increase survival in OHCA with initial PEA/asystole. The recommended initial dose is 1-2mEq/kg; giving at least 2 amps of bicarb (rather than the standard 1) should achieve this in many patients.
Emergency physicians are familiar with posterior reversible [leuko]encephalopathy syndrome as an entity associated with untreated hypertension. It also happens to be a well-documented entity amongst solid organ transplant patients.
While the exact pathophysiology remains unclear, PRES is characterized by posterior subcortical vasogenic edema due to blood-brain barrier disruption, usually in the setting of elevated blood pressure with loss of cerebral autoregulation and/or endothelial dysfunction.
The immunosuppressants used in this population, namely calcineurin inhibitors (CNI) such as tacrolimus and cyclosporine, are thought to contribute most to this endothelial dysfunction and development of PRES in transplant patients, although high-dose corticosteroids, ischemia-reperfusion injury during surgery, and antibiotics have also been implicated.
Presentation of PRES post-transplant:
Clinical symptoms:
Time course:
Diagnostics:
Management:
Bottom Line:
Patients with a history of solid organ transplant are at risk for PRES. While ED stabilization of these patients remains the same, recognition of PRES as a potential etiology for a transplant patient's presentation is crucial to proceed with important testing and necessary changes to their immunosuppressive regimen.
Deep sedation in the ED has previously been associated with longer duration of mechanical ventilation, longer lengths of stay, and higher mortality.1 Current guidelines recommend light sedation, consistent with a goal RASS of -2 to 0, for most critically-ill patients in the ICU.2
The ED-SED3 multicenter, pragmatic, before-and-after feasibility study implemented an educational initiative (inservices, regular reminders, laminated sedation charts) to help target lighter sedation depths in newly-intubated adult patients without acute neurologic injury or need for prolonged neuromuscular blockade.
After educational intervention:
Even with the caveats of the confounding and bias that can exist in before-and-after studies, these results are consistent with prior sedation-related studies and offer more evidence to support for avoiding deep sedation in our ED patients. The study also demonstrates the importance of nurse-driven sedation in achieving sedation goals.
Bottom Line: Our initial care in the ED matters beyond initial stabilization and compliance with measures and bundles. Avoid oversedating intubated ED patients, aiming for a goal RASS of -2 to 0.
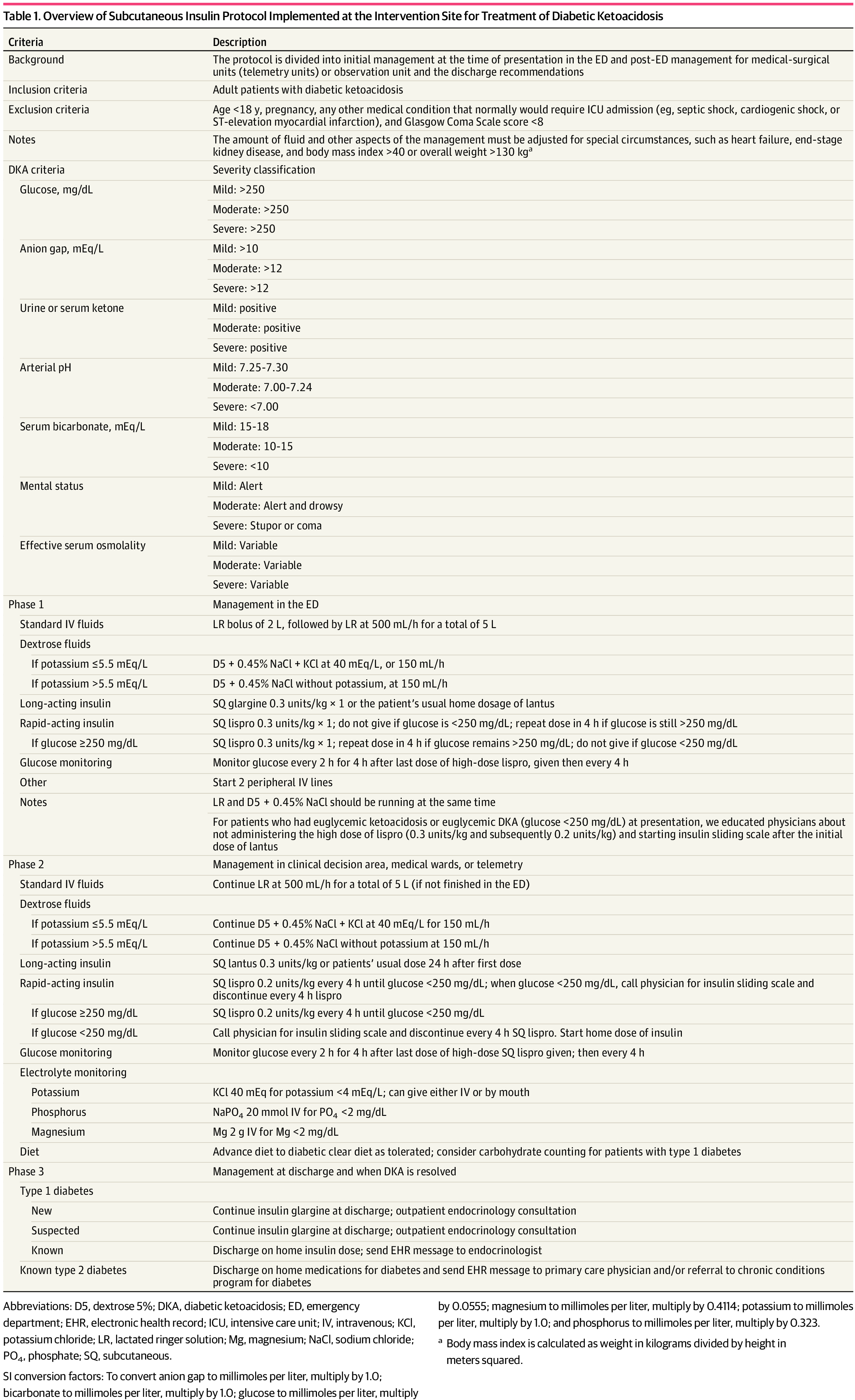
Background: It is classically taught that the tenets of DKA management are IV fluids, electrolyte repletion, and an insulin infusion that is titrated until approximately 2 hours after anion gap closure, when long-acting subcutaneous insulin is administered if the patient is tolerating oral intake. It has been previously found that earlier administration of subcutaneous long-acting insulin can shorten the time to anion gap closure, while other small studies have noted similar efficacy in subcutaneous insulin compared to IV in mild/moderate DKA.
A recent JAMA article presents a retrospective evaluation of a prospectively-implemented DKA protocol (see "Full In-Depth" section) utilizing weight-based subcutaneous glargine and lispro, rather than IV regular insulin, as part of initial and ongoing floor-level inpatient treatment.
When compared to the period before the DKA protocol:
The only exclusion criteria were age <18 years, pregnancy, and presence of other condition that required ICU admission.
Bottom Line: Not all DKA requires IV insulin infusion.
At the very least, we should probably be utilizing early appropriate-dose subcutaneous long-acting insulin. With ongoing ICU bed shortages and the importance of decreasing unnecessary resource use and hospital costs, perhaps we should also be incorporating subcutaneous insulin protocols in our hospitals as well.
Based on prior studies1 indicating possibly improved outcomes with vasopressin and steroids in IHCA (Vasopressin, Steroids, and Epi, Oh my! A new cocktail for cardiac arrest?), the VAM-IHCA trial2 compared the addition of both methylprednisolone and vasopressin to normal saline placebo, given with standard epinephrine resuscitation during in hospital cardiac arrest (IHCA).
The use of methylprednisolone plus vasopressin was associated with increased likelihood of ROSC: 42% intervention vs. 33% placebo, RR 1.3 (95% CI 1.03-1.63), risk difference 9.6% (95% CI 1.1-18.0%); p=0.03.
BUT there was no increased likelihood of favorable neurologic outcome (7.6% in both groups).
Recent publication on evaluation of long-term outcomes of the VAM-ICHA trial3 showed that, at 6-month and 1-year follow-up, there was no difference between groups in:
Bottom Line: Existing evidence does not currently support the use of methylprednisolone and vasopressin as routine code drugs for IHCA resuscitation.
Background: Conventional medical wisdom long held that patients with pneumothorax (PTX) who require positive pressure ventilation (PPV) should undergo tube thoracostomy to prevent enlarging or tension pneumothorax, even if otherwise they would be managed expectantly.1
Bottom Line: The cardiopulmonar-ily stable patient with small PTX doesn’t need empiric tube thoracostomy simply because they’re receiving positive pressure ventilation. If you are unlucky enough to still have them in your ED at day 5 in these COVID times, provide closer monitoring as the observation failure rate may increase dramatically around this time.
Fever has long been understood to be associated with worse outcomes in patients post-cardiac arrest. Whether ascribing to the goal of 33-34°C, 36°C, or simply <38°C, close monitoring and management of core temperatures are a tenet of post-cardiac arrest care.
A recently published study compared the effectiveness of several methods in maintaining temperatures <38°C…
Results:
Maintenance of temp <38°C:
Mean change in temp from baseline:
Limitations:
Bottom Line:
Background:
There are also no clear guidelines regarding how fast fluid boluses should be administered, and there has been debate about whether different infusion rates could lead to different outcomes in patients receiving intravenous fluid (IVF) boluses (i.e. fast infusions may cause more third spacing due to the rapidity of the expansion of the intravascular space compared to fluid administered more slowly). A recent study compared IVF infusion rates in ICU patients.
-- Unblinded, randomized
-- 10,520 patients clinically requiring a fluid challenge, from 75 ICUs in Brazil
-- Infusion rate 333 mL/hr vs 999 mL/hr
* (Trial also compared plasmalyte vs 0.9% saline, analyzed in separate study)
-- Some notable exclusion criteria: severe hypo/hypernatremia, AKI or expected to need RRT 6 hrs after admission
--Other caveats:
* Faster infusion rates allowed at physician discretion in patients with active bleeding or severe hypotension (SBP < 80 or MAP < 50 mmHg); patient was returned to assigned rate after condition resolved
* Almost 1/2 the patients received at least 1L of IVF in 24 hours prior to enrollment
-- Results: No sig difference in 90-day survival, use of RRT, AKI, mechanical ventilator free days, ICU/hospital mortality/LOS
Bottom Line: There is not yet compelling evidence that there are differences in patient outcomes in patients receiving fluid boluses given at 333 cc/hr vs. 999 cc/hr.
Approximately 15,000 children experience an in hospital cardiac arrest (IHCA) with little improvement in outcomes over the last two decades. During that time, epinephrine has been the constant basis for resuscitation of these patients. Current recommendations by the AHA recommend bolus dosing of epinephrine every 3-5 minutes in a pediatric cardiac arrest. Animal studies suggest that more frequent dosing of epinephrine may be beneficial.
This was a retrospective study of 125 pediatric IHCAs with 33 receiving “frequent epinephrine” interval (≤2 minutes). Pediatric CPC score 1-2 or no change from baseline was used as primary outcome to reflect favorable neurologic outcome, with frequent dosing associated with better outcome (aOR 2.56, 95%CI 1.07 to 6.14). Change in diastolic blood pressure was greater after the second dose of epinephrine among patients who received frequent epinephrine (median [IQR] 6.3 [4.1, 16.9] vs. 0.13 [-2.3, 1.9] mmHg, p=0.034).
This study is subject to all sorts of confounding and should be studied more rigorously, but suggests that more frequent dosing for pediatric IHCA may be of benefit.
Despite the knowledge that minimizing interruptions in chest compressions during CPR is key to maintaing coronary perfusion pressure and chance of ROSC,1-4 difficulties in limiting hands-off time remain.
Dewolf et al.5 recently performed a prospective observational study using body cameras to find that 33% (623/1867) of their CPR interruptions were longer than the recommended 10 seconds:
Previous studies have shown an increase in hands-off time associated with the use of cardiac POCUS during rhythm checks as well.6,7
Bottom Line:
A recent prospective observational study examined the diagnostic usefulness of head-to-pelvis sudden death computed tomography (SDCT) in 104 patients with ROSC and unclear OHCA etiology.
Diagnostic performance:
Safety:
Bottom Line: For OHCA without clear etiology, SDCT explicitly including a thoracic CTA may have diagnostic benefit over standard care alone with the added benefit of identification of resuscitation complications.
Supplemental oxygen therapy is frequently required for patients presenting with acute respiratory distress and COPD exacerbation. Over-oxygenation can derail compensatory physiologic responses to hypoxia,1 resulting in worsening VQ mismatch and, to a lesser degree, decreases in minute ventilation, that cause worsened respiratory failure.
The 2012 DECAF (Dyspnea, Eosinopenia, Consolidation, Acidaemia, and Atrial Fibrillation) score was found to predict risk of in-hospital mortality in patients admitted with acute COPD exacerbation.2,3 Data from the DECAF study’s derivation and external validation cohorts were examined specifically to look at outcome associated with varying levels of oxygen saturation.
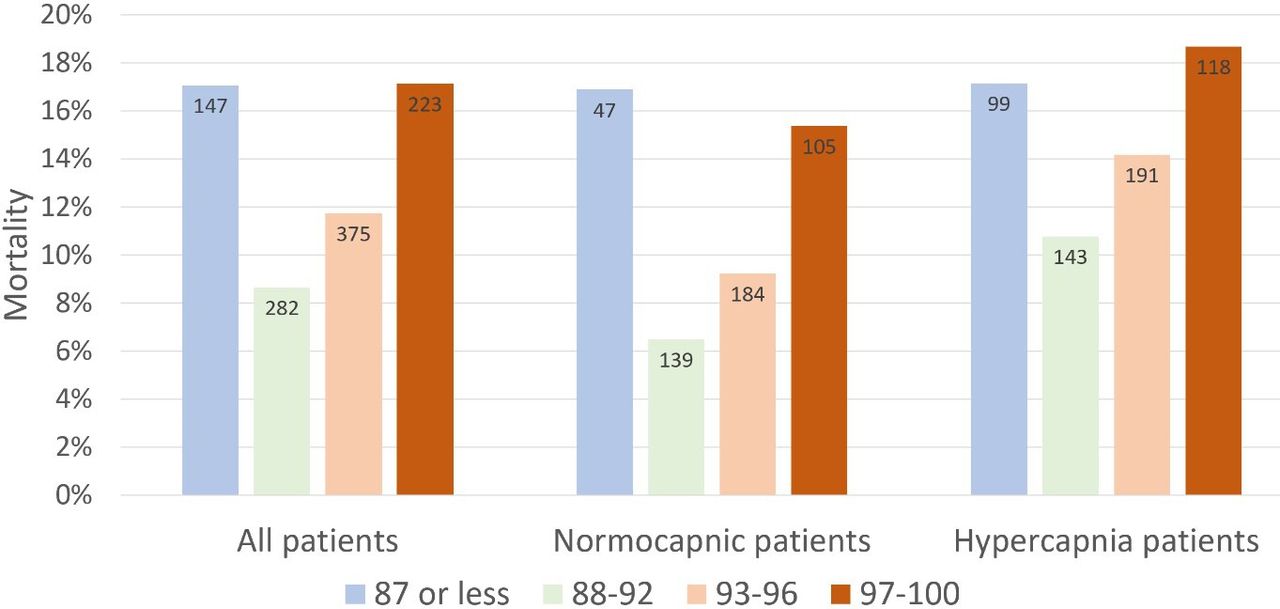
Bottom Line
In patients presenting to the ED with acute COPD exacerbation requiring oxygen supplementation, a target oxygen saturation of 88-92% is associated with the lowest in-hospital mortality, and higher oxygen saturations should be avoided independent of patients' PCO2 levels.
Background: In respiratory failure due to COPD and cardiogenic pulmonary edema, noninvasive positive pressure ventilation decreases need for intubation and improves mortality,1 while its utility in other scenarios such as ARDS and pneumonia has yet to be proven.1,2 We know that patients on NIV with delays to needed intubation have a higher mortality,1,3 but intubation and mechanical ventilation come with risks that it is preferable to avoid if possible.
So how and when can we determine that NIV is not working?
The HACOR (Heart rate, Acidosis, Consciousness, Oxygenation, Respiratory rate) score at 1 hour after NIV initiation has been demonstrated to be highly predictive of NIV failure requiring intubation.4,5
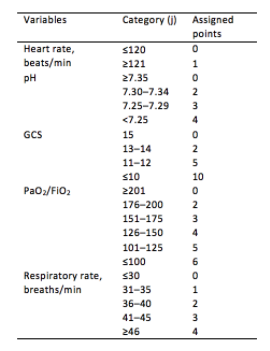
Initial development/validation: Score > 5 after 1 hour of NIV corresponds to >80% risk of NIV failure4
Earlier intubation (before 12 hours) in these patients = better survival
External validation: Score > 8 after 1 hour of NIV most predictive of eventual NIV failure 5
Average score @ 1-hour of patients with NIV success = 3.8
Score remained predictive at 6, 12, 24, 48 hours as well & mortality worsened as delay to intubation time increased
Baseline, pre-NIV score not predictive
Better predictive agreement in pneumonia and ARDS
Bottom Line:
Patients on NIV require close reassessment to prevent worsened survival due to intubation delay should invasive mechanical ventilation be indicated.
A HACOR score >8 after 1 hour of NIV should prompt intubation in most instances, with strong consideration given to a score >5.
*Note: ABGs were obtained for PaO2 assessment in the above studies -- the use of SpO2 was not evaluated -- but we are often not obtaining ABGs in our ED patients with acute respiratory failure. The following chart provides an estimated SpO2 to PaO2 conversion.
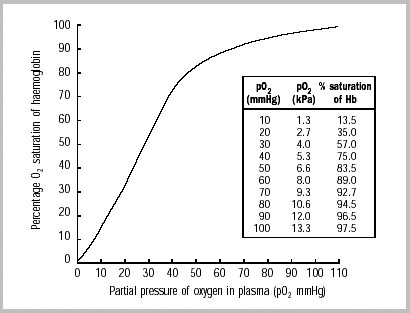
WHO 2001
Caveats:
As the number of COVID-19 cases rises worldwide, prehospital and emergency department healthcare workers remain at high risk of exposure and infection during CPR for patients with cardiac arrest and potential SARS-CoV-2.
Existing evidence supports similar cardiac arrest outcomes in airways managed with a supraglottic airway (SGA) compared to endotracheal intubation (ETT).1 It is generally accepted that the best airway seal is provided with endotracheal intubation + viral filter, but how well do SGAs prevent spread of aerosols?
In CPR simulation studies:
While the invasive monitoring of central venous pressure (CVP) in the critically ill septic patient has gone the way of also transfusing them to a hemoglobin of 10 mg/dL, it remains that an elevated CVP is associated with higher mortality1,2 and renal failure.2,3
Extrapolating from existing data looking at hepatic vein, portal vein, and renal vein pulsatility as measures of systemic venous hypertension and congestion,4,5,6 Beaubien-Souligny et al. developed the venous excess ultrasound (VExUS) grading system incorporating assessment of all 3, plus the IVC, using US to stage severity of venous congestion in post-cardiac surgery patients.7 They evaluated several variations, determining that the VExUS-C grading system was most predictive of subsequent renal dysfunction.
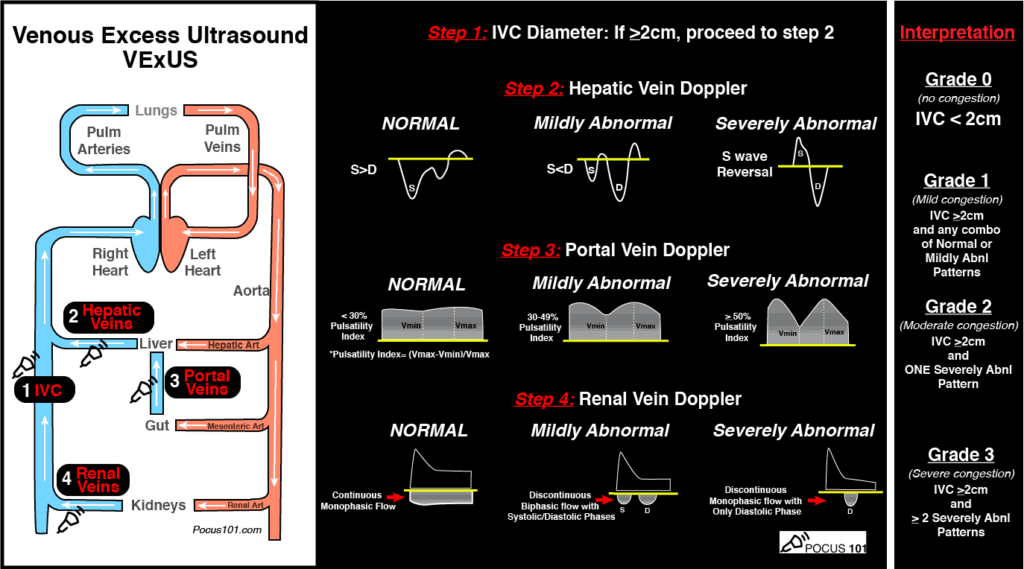
(Image from www.pocus101.com)
High Points
VExUS Grade 3 (severe) venous congestion:
Caveats
Clinical Uses
A great how-to can be found here:
https://www.pocus101.com/vexus-ultrasound-score-fluid-overload-and-venous-congestion-assessment/
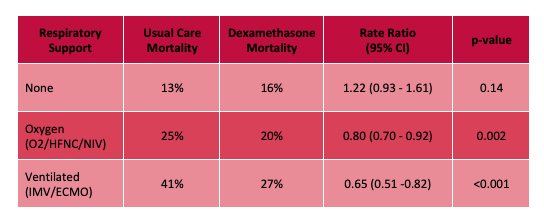
The RECOVERY (Randomized Evaluation of COVid-19 thERapY) investigators recently published a non-peer reviewed article on their findings utilizing dexamethasone to treat patients with COVID-19.
Rx: Dexamethasone 6mg daily* x 10 days (PO or IV) *or steroid equivalent
Primary outcome: All-cause mortality at 28-days
Secondary outcomes:
Results:
Limitations:
Bottom Line: Strongly consider admininstering dexamethasone to your patients with known COVID-19 who require respiratory support, and look for the peer-reviewed publication from the RECOVERY Trial investigators.
Background:
· Empiric broad spectrum antibiotic therapy is a mainstay of the management of critically ill patients with septic shock.
· Vancomycin is widely used for the coverage of potential MRSA infection
· Continuous infusion of vancomycin has been repeatedly demonstrated to reach target serum concentrations faster, maintain consistent serum vancomycin levels better, with fewer serum concentration sampling required, and less overall vancomycin required to do so, in both adult and pediatric populations.2-5
Current Article:
Flannery AH, Bissell BD, Bastin MT, et al. Continuous Versus Intermittent Infusion of Vancomycin and the Risk of Acute Kidney Injury in Critically Ill Adults: a Systematic Review and Meta-Analysis. Crit Care Med. 2020;48(6):912-8.
· Systematic review and meta-analysis of 11 studies for a total of 2123 patients
· Comparing continuous versus intermittent vancomycin infusion.
· Primary outcome of AKI, secondary outcome of mortality
· Found a reduction in the incidence of AKI in the continuous infusion cohort:
· No association between infusion strategy and mortality
Considerations:
· Initial loading dose used in most of the studies (15 mk/kg) probably underdosed, current recommendation for 25mg/kg initial loading dose7 (which is not even always effective by itself)8 (Reardon)
· Continuous infusion may be difficult with limited IV access
· AKI associated with increased hospital stay, costs, mortality (although didn’t pan out in study) – worth preventing if possible.
Take Home:
· Give a 25-30mk/kg loading dose of vancomycin in critically ill patients with suspicion of MRSA to achieve target serum concentrations sooner.
· Continuous vancomycin is a viable option and could be considered in ED boarders, especially if there is concern for impending renal injury.
There is currently a high, and appropriate, concern regarding the aerosolization of viral particles during various methods of respiratory support. While studies are limited, here is some of the currently available data (mostly-simulated) on the approximate maximum distances of particle spread:
Nasal Cannula 5LPM:1 1 ft 4.5 in
Non-Rebreather Mask, 6-12LPM: 4 in, minimal change with increasing flows1
High Flow Nasal Cannula
CPAP (20 cmH2O) provided by oronasal mask with good fit (leak from exhaust port):2 11.5 in
Bilevel positive airway pressure w/ oronasal mask (IPAP 10-18/EPAP 4): max dispersal:4 1 ft 7.7 in
Bilevel positive airway pressure with full facemask5 (IPAP 18 / EPAP 5): 2 ft 8 in
Bilevel positive airway pressure with helmet:4
Utility of Surgical Mask:6
Bottom Line:
In vivo data from actual patients is lacking, however there is potentially lower risk of aerosol spread with HFNC than regular nasal cannula, perhaps due to higher likelihood of a tighter nare/nasal cannula interface. Nonrebreather mask performs well indirectly with the shortest dispersal distance. Noninvasive positive pressure ventilation with an oronasal mask and good seal has a relatively short dispersal distance, and a surgical mask over respiratory support interventions actively decreases amount, if not distance, of particle spread. Use of appropriate PPE and negative pressure rooms, if available, remains key.
With ED-boarding of critically-ill patients becoming more common, it is likely that ED physicians may find themselves caring for a patient who develops ACS – that is, abdominal compartment syndrome. While intraabdominal hypertension (IAH) is common and is defined as intraabdominal pressure > 12 mmHg, ACS is defined as a sustained intraabdominal pressure > 20mmHg with associated organ injury.
WHY you need to know it:
ACS → Increased mortality & recognition is key to appropriate management
WHO is at risk:
HOW it kills:
→ Lactic acidosis, respiratory acidosis, multisystem organ failure, cardiovascular collapse & death
WHEN to consider it:
WHAT to do:
Bottom Line: Abdominal compartment syndrome is an affliction of the critically ill, is assosciated with worsened mortality, and requires aggressive measures to lower the intraabdominal pressure while obtaining emergent surgical consultation for potential emergent laparotomy.