FILE RESEND. This was tested via email and will hopefully work. I apologize for errors - Dlemkin (webmaster)
What is the diagnosis? (DON'T LOOK DOWN AT THE ANSWER)
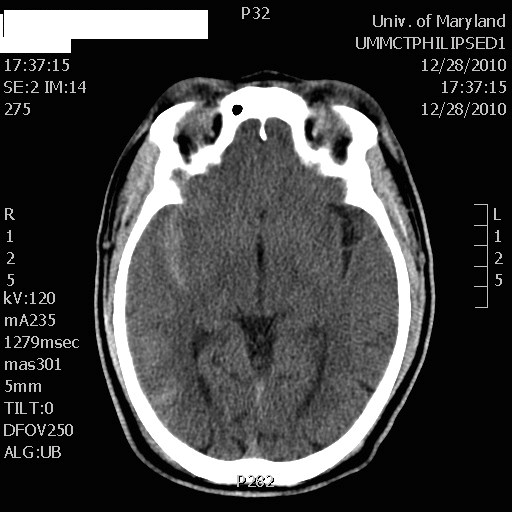
50 year-old male prisoner s/p assault, + LOC
CT shows right-sided traumatic subarachnoid hemorrhage
-- CSF reforms within 6 hours, making its removal short-term, unless there is a CSF leak.
-- LP can be challenging in obese patients and uncomfortable for patients, in general.
-- LP complications such as low pressure headaches, CSF leak, CSF infection, and intraspinal epidermoid tumors.
Optimal management of subarachnoid hemorrhage requires prognostic understanding and effective communication with neurology and neurosurgical consultants, as well as the patient and their family members.
It is therefore often helpful to utilize and reference the widely recognized Hunt and Hess Scale in grading symptoms of ruptured cerebral aneurysm and subarachnoid hemorrhage severity:
For your convenience, an online Hunt and Hess Scale calculating tool can be found at:
http://www.mdcalc.com/hunt-and-hess-classification-of-subarachnoid-hemorrhage-sah
Classic Cerebrospinal Fluid Characteristics
--- High NIH Stroke Scale scores.
--- Large areas of infarct.
--- Cerebellar infarcts.
--- Extended time to tPA administration.
--- Previous stroke.
--- Older age.
Chlorhexidine (CHG) has rapidly become the antiseptic of choice for most skin preparation prior to any percutaneous procedures including:
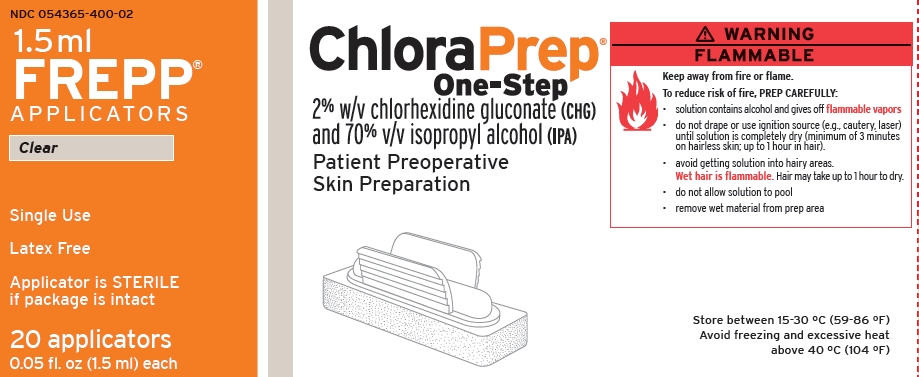
The Chlorprep(R) label notes: "DO NOT USE FOR LUMBAR PUNCTURE OR IN CONTACT WITH THE MENINGES" (attached)
Authors of the British Royal College of Anaesthetists 3rd National Audit Project provided some guidance for the use of chlorhexidine for spinal procedures
Further: Correspondance from the Journal of Regional Anesthesia and Pain Medicine
"Dr. David Hepner published a correspondence in the April 2007 issue of Anesthesiology that stated the expert panel for Regional Anesthesia and Pain Medicine “felt strongly that although the US Food and Drug Administration has not approved chlorhexidine before lumbar puncture, it has a significant advantage over povidone iodine because of its onset, efficacy, and potency” and commented that “interestingly, povidone iodine is also not approved for lumbar puncture."
Chlorhexidine off-label use is supported in academic literature. Due to specific labeling prohibiting use, a formal institutional policy to support such use may be indicated.
How to Perform a Median Nerve Block