Within the past few days we completed a review of complications of COVID-19, to describe what sequelae and clinical patterns, besides the obvious (URI, respiratory failure, ARDS, sepsis, etc), are noted in the literature. This review, along with a plethora of other information focusing on critical care of the COVID-19 patient, will be posted in the next few days to http://covid19.ccproject.com/. Below are the key points from that review:
Acute cardiovascular complications appear to be the most common and concerning sequelae:
-Acute myocardial injury (7-17% of hospitalized patients in one study),
-Myocarditis (primary cause of death in 7% of COVID deaths in one study),
-Arrhythmias (16.7% of hospitalized and 44.4% of ICU patients in one study),
-Venous thromboembolism (incidence unknown).
Concerns for sudden cardiac death, even after recovery, have been raised but are not well documented in the literature. Proposed mechanisms include respiratory compromise, myocarditis, malignant tachydysrhythmias, heart failure, and coronary plaque instability (i.e. Type 1 MI) secondary to inflammation
Co-infection and secondary infection rates are unknown but estimates range from 4.8% to 21%, with higher rates in sicker patients. Viral co-infection is more common than bacterial co-infection, but both may be seen. The ability to rule out COVID-19 by a positive multiplex respiratory viral panel is questionable.
Cytokine release syndrome and secondary HLH are both described complications, but their incidence is unknown. The relation of this finding to purported benefits of tocilizumab (which is also a therapy for HLH) is unknown.
Other extrapulmonary complications are relatively typical of sepsis, such as kidney injury, abnormal LFTs, and delirium
If anyone would like a copy of the full document, which details known complications by organ system, please feel free to email me at msutherland@som.umaryland.edu. Thanks to David Gordon for organizing the project.
Everyone stay safe, and be sure to take care of each other, as well as our patients.
This week we anticipate treating more COVID19 cases as they progress to ARDS. The World Health Organization issued guidelines on 3/13/20 for treating Severe Acute Respiratory Infection (SARI) due to COVID19.
How to identify ARDS?
No different than before COVID. Order a CXR, ABG, and perform bedside ultrasound evaluation of cardiac function and volume status. If there are bilateral opacifications you cannot explain entirely with volume overload, nodules, or lobar collapse, AND if the ratio of PaO2/FiO2 is < 300 (mild), < 200 (moderate), or < 100 (severe), then treat for ARDS.
***While you are waiting for your blood gas, SpO2/FiO2 <315 suggests ARDS.
What is the oxygen goal?
During resuscitation: > 93%
Once stabilized: > 89%
What is the expected clinical course?
Patients experience RAPID deterioration to respiratory failure. You should expect to intubate. This should be performed with N95 protection and should be done by the person with greatest first pass success.
Be CONSERVATIVE with fluids. Do not give a 30mL/kg bolus. Give 250-500mL bolus and re-evaluate. Excess fluid results in prolonged hypoxia and mechanical ventilation.
Should empiric treatments change?
No. Co-infection with influenza, bacterial pneumonia, and all other pathogens is possible, so you should continue to cover all suspected pathogens and de-escalate as microbiology labs result.
Should ventilator settings change?
No. Use lung protective volumes and permissive hypercapnia. The volume is based on the patient's height, not weight. A quick way to do this? Measure the height in cm. Subtract 100 for a man and subtract 110 for a woman and this is the ideal body weight. Provide 6mL/kg of tidal volume with a goal plateau pressure < 30. Use the high PEEP strategy from the ARDSnet trial and even consider clamping the ET tube when transitioning from machine to bag for transport in order to preserve PEEP.
Do patients benefit from proning?
Yes. 12-16 hours/day for severe ARDS. Not true in pregnancy as a whole, though early pregnancy may still benefit.
Is ECMO beneficial in refractory cases?
Unknown. In the case of MERS-CoV, ECMO reduced mortality.
Are corrticosteroids useful?
No. Do not administer steroids routinely to these patients. You may give steroids where indicated, including cases of refractory shock following pressors.
(*It is important to note that many of the percentages in these early studies will change as more asymptomatic or minimally symptomatic patients are identified with increased testing)
Epidemiology
Among more than 44,000 confirmed cases of COVID-19 in China as of Feb 11, 2020:
- 30–69 years: ~78%
- severely or critically ill: ~19%
Case-fatality proportion:
-60-69 years: 3.6%
-70-79 years: 8%
-≥80 years: 14.8%.
-With no underlying medical conditions: overall case fatality of 0.9%
-With comorbidities:
-cardiovascular disease (10.5%), diabetes (7%)
-chronic respiratory disease, hypertension, and cancer (6% each)
Presentation
For patients admitted to the hospital, many non-specific signs and symptoms:
- fever (77–98%) and cough (46%–82%) were most common
- of note, gastrointestinal symptoms (~10%) such as diarrhea and nausea present prior to developing fever and lower respiratory tract signs and symptoms.
Diagnosis
No general lab tests have great sensitivity or specificity
A normal CT scan does NOT rule out COVID-19 infection
-In an early study, 20/36 (56%) of patients imaged 0-2 days (‘early’) after symptom onset had a normal CT with complete absence of ground-glass opacities and consolidation
Treatment-
Mainstay of treatment will be management of hypoxemia including early intubation if necessary. However, specifically:
-Steroid therapy is controversial and the WHO is currently recommending against it unless it is being administered for another reason
-has not been associated with any benefit
-associated with possible harm in previous smaller studies with SARS and MERS
-associated with prolonged viremia
-intravenous remdesivir (a nucleotide analogue prodrug with promising in-vitro results against SARS-CoV and MERS-CoV) is available for compassionate use
-lopinavir-ritonavir has been used without any associated benefit
Settings: Multicenter randomized controlled trial
Patients: 710 patients
Intervention: 345 patients. no sedative but only boluses of morphine as clinically indicated (Sedation group)
Comparison: 356 patients. light sedation with daily interruption (Nonsedation group)
Outcome: all-cause mortality at 90 days after randomization
Study Results:
42.4% of nonsedation group died vs 37% of sedation group (95% confidence interval [CI], −2.2 to 12.2; P = 0.65).
Number of ventilator-free days for nonsedation group was 27 days vs. 26 for sedation group.
Discussion:
This study did not agree with previous studies that lighter sedation was associated with shorter length of stay on mechanical ventilation , ICU or hospital. The authors attributed to the findings that RASS score was not significantly different between the 2 groups.
Conclusion:
Critically ill adult patients receiving mechanical ventilation, there was no difference in 90-day mortality between patients receiving light sedation or no sedation.
With ED-boarding of critically-ill patients becoming more common, it is likely that ED physicians may find themselves caring for a patient who develops ACS – that is, abdominal compartment syndrome. While intraabdominal hypertension (IAH) is common and is defined as intraabdominal pressure > 12 mmHg, ACS is defined as a sustained intraabdominal pressure > 20mmHg with associated organ injury.
WHY you need to know it:
ACS → Increased mortality & recognition is key to appropriate management
WHO is at risk:
HOW it kills:
→ Lactic acidosis, respiratory acidosis, multisystem organ failure, cardiovascular collapse & death
WHEN to consider it:
WHAT to do:
Bottom Line: Abdominal compartment syndrome is an affliction of the critically ill, is assosciated with worsened mortality, and requires aggressive measures to lower the intraabdominal pressure while obtaining emergent surgical consultation for potential emergent laparotomy.
Don't forget cerebral fat embolism syndrome (FES) on the differential for altered trauma patients. FES is typically associated with long bone fractures, but has been reported with other fractures, orthopedic reaming (i.e. aggressive orthopedic procedures), and in rare cases even with non-fracture (soft-tissue) trauma. Typically symptoms occur between 24 and 72 hours after injury, but there have been cases both earlier and later. Diagnosis is clinical, but MRI may be helpful, and will often show multiple cerebral white matter lesions. It is debated whether FES is truly an embolic phenomena (i.e fat molecules traveling to and blocking blood supply of organs), or rather an inflammatory response to free fatty acids in the blood stream (i.e. more of a vasculitis type pathology). Management is supportive care, but give these patients time as there can be favorable outcomes, even after prolonged coma.
Dr. Bryan Hayes wrote a Pearl 10/4/2013 to remind us autoimmune encephalitis can present like neuroleptic malignant syndrome.
Dr. Danya Khouja wrote a Pearl 6/28/2017 to inform us autoimmune encephalitis is associated with tumors and can be investigated with serum and CSF antibody panels.
Since those publications, the number of validated autoimmune biomarkers in these panels has increased dramatically. In 2020 we now know, autoimmune encephalitis is at least as common as infectious encephalitis.
Here is how to diagnose it
1. Suspect the diagnosis in patients with subacute/rapidly progressive altered mental status, memory loss, or psychiatric symptoms. It can be mistaken for a new diagnosis of schizophrenia or bipolar disorder.
2. Look for one or more additional findings: new seizures, focal CNS findings, CSF pleocytosis, MRI findings
3. Exclude other likely etiologies (but try not to get hung up on a positive drug test, especially if drug use was not recent).
Why is this important?
Early treatment with steroids and plasmapheresis can prevent progression of disease (prevent seizures, prevent months-long hospitalizations).
Young girls are especially likely to have teratomas as a cause for the disease. Finding and resecting those tumors is life-saving.
Mechanical Ventilation Pearls for Acute Ischemic Stroke
Settings: multicenter, double-blind, phase 3 trial (apparently vitamin D worked in phase 2 trials).
Study Results:
Discussion:
Conclusion:
Early administration of high dose vitamin D did not improve 90-day all cause mortality.
The arrival of a critically ill pregnant patient to the ED can be anxiety-provoking for emergency physicians as two lives and outcomes must be considered.
Some basic tenets of care, regardless of underlying issue, include:
Finally, once critical illness is identified the OB and NICU teams should be consulted immediately. Fetal distress in a viable pregnancy may be an indication for delivery, and initiation of the transfer process should occur if the supportive specialties are not in-house.
There are few conditions that can be as dramatic or difficult to control as variceal GI bleeding in a cirrhotic patient. It is important to be familiar with all options in these cases, from Blakemore/Minnesota tube placement to massive transfusion to when and which consultants to get involved. In cases that are refractory or not amenable to endoscopic intervention, emergent interventional radiology consultation for Transjugular Intrahepatic Portosystemic Shunt (TIPS) may be a consideration. In high risk cases, think about getting IR on the phone at the same time as you engage GI, in case endoscopic management fails. Variceal bleed patients can decompensate rapidly, get your consultants involved early!
Generally accepted indications for emergent TIPS (both of the following should be true):
-GI bleeding not amenable or not controllable by endoscopy
-Cause is felt to be variceal. May also consider in portal hypertensive gastropathy
Contraindications:
-Right heart failure or pulmonary hypertension
-Severe liver failure (MELD > 22, T Bili > 3 or Child-Pugh C. In these cases TIPS may not confer a significant survival benefit)
-Hepatic encephalopathy (relative contradindication. HE may be worsened by TIPS).
-Polycystic liver disease (makes TIPS technically challenging)
-Chronic portal vein thrombus (makes TIPS technically challenging. Acute PV thrombus is NOT considered a contraindication)
Bottom Line: In cases of variceal GI bleeding from portal hypertension, consider getting IR on the phone early to discuss emergent TIPS.
Pearl: consider desmopressin (DDAVP) for patients with an intracranial hemorrhage who are taking an antiplatelet. Caution, this is not for patients with an ischemic stroke with hemorrhagic conversion and it was not specifically evaluated for patients on anticoagulation or going to the OR with neurosurgery.
How strong is this evidence? International guidelines already give cautious approval for this practice, and now there is a retrospective review to support it. Though there were only 124 patients in the trial, the rate of hemorrhage expansion was much lower in the DDAVP group (10.9% vs 36.2%, P = .002) and there was no increased risk of hyponatremia (no events reported).
Interventions Shown to Reduce Mortality in RCTs
Settings
Study Results:
Discussion:
This study’s results differed from previous single center study (Girardis JAMA 2016) or meta analysis (Chu DK, Lancer 2018), which showed mortality benefit in patients with conservative oxygen (Girardis & Chu) and more ventilator-free days (Girardis).
Conclusion: Conservative oxygen did not significantly affect the ventilator free days of mechanically ventilated patients.
When managing cardiac arrest, it is important to differentiate PEA, the presence of organized electrical activity without a pulse, from "pseudo-PEA,"where there is no pulse but there IS cardiac activity visualized on ultrasound.
Why:
How:
What:
Bottom Line: Pseudo-PEA is different from PEA. Utilize POCUS during your cardiac arrests to identify it and to help diagnose reversible causes, and treat it as a profound shock state with the appropriate supportive measures, i.e. pressors or inotropy.
Ever been in an acute rescucitation and found yourself unable to remember all of those famous ACLS Hs and Ts? I know I have. A few years ago Littman et al published an alternative approach to critically ill, hypotensive medical patients with non shockable rhythms. Unfortunately, it seems like some of the enthusiasm for this approach has died down, but I still think it's something you're more likely to recall in a pinch than the Hs and Ts and is a better way of getting started with a hypotensive non-trauma patient. And it's so simple you may actually remember it!
1) Look at the monitor. Is the rhythm narrow or wide?
2a) Narrow - more likely a mechanical problem (tamponade, tension PTX, autoPEEP, or PE). Give IVF and search for one of these causes (and correct it!). Keep in mind that ultrasound can help you differentiate a lot of these.
2b) Wide - more likely a metabolic problem (hyperK, sodium channel blockade, etc*). Give empiric calcium, bicarb, and other therapies targeted for these problems (if desired) and get stat labs.
Take a minute and either go to this REBEL EM post:
https://rebelem.com/a-new-pulseless-electrical-activity-algorithm/
To review this, or look at the attached diagrams.
*Dr. Mattu would want me to remind you that hyperkalemia IS a sodium channel poisoned state, so there's no need to think of these two separately
The Critically Ill Geriatric Patient with Sepsis
Rationale: Data regarding temperature management in patients suffered from cardiac arrest with nonshockable rhythm was inconclusive.
Objective: whether moderate hypothermia at 33C, compared with normothermia at 37C would improve neurologic outcome in patients with coma after cardiac arrest with nonshockable rhythm.
Outcome: survival with favorable 90-day neurologic outcome (Cerebral Performance Category scale 1-2/5)
SummaryThere was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
This randomized multicenter trial involved 581 patients with cardiac arrest and nonshockable rhythm. Hypothermia group included 284 patients vs. 297 in the normothermia group. Median GCS at enrollment = 3.
Majority of patients was cooled with the use of a basic external cooling device: 37% for hypothermia and 50.8% for normothermia group.
There was higher percentage of patients achieving CPC 1-2 in the hypothermia group (10.2%) vs normothermia group (5.7%, Hazard Ratio 4.5, 95% CI 0.1-8.9, p=0.04)
Limitation:
A. The study used strict enrollment criteria:
B. normothermia group had higher proportion of patients with temperature at 38C.
C. Hypothermia group underwent temperature management of 56 hours vs. 48 hours for normothermia patients.
Take home points:
In a selected group of patients with cardiac arrest and nonshockable rhythm, moderate hypothermia at 33C may improve neurologic outcome.
Blood Transfusion Thresholds in Specific Populations
Sepsis - 7 g/dL
Acute Coronary Syndrome - no current specific recommendations pending further studies
Stable Cardiovascular Disease - 8 g/dL
Gastrointestinal Bleeds
Acute Neurologic Injury - Traumatic Brain Injury - 7 g/dL
Postpartum Hemorrhage - 1:1:1 ratio strategy
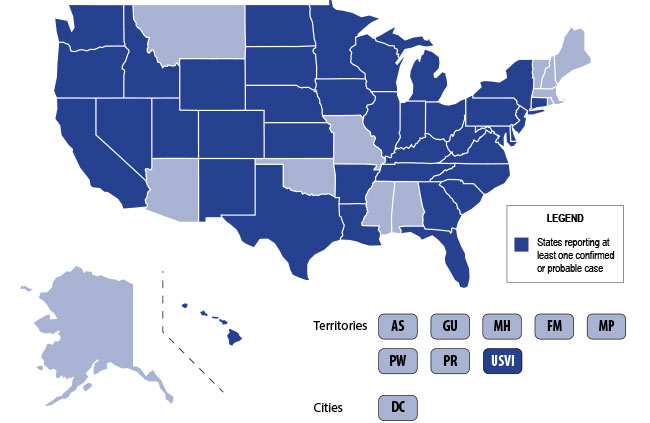
The U.S. is currently experiencing an epidemic of a severe lung disease termed Vaping-Associated Pulmonary Illness (VAPI), with over 500 cases and 7 deaths across 38 states and 1 U.S. territory since July 2019.
The clinical presentation of VAPI varies --
Diagnostics --
Treatment is supportive +/- steroids --
Bottom Line: Include vaping-associated pulmonary illness in your differential for patients presenting with acute lung disease.