STARRT-AKITrial
The Standard versus Accelerated initiation of Renal Replacement Therapy in Acute Kidney Injury
The development of acute kidney injury (AKI) in the critical care setting portends a greater morbidity and mortality for patients. Additionally, it places the patient at high risk of complications and requires a greater use of resources. Several studies in the past have examined if the timing of initiation of renal replacement therapy (RRT) would result in a mortality benefit, but have failed to demonstrate consistent outcomes.
The STARRT-AKI trial was a multinational, randomized controlled trial designed to determine if early initiation of RRT in critically ill adult patients with AKI lowered the risk of 90-day mortality. The Kidney Disease Improving Global Outcomes (KDIGO) classification was used to define AKI and over 2900 patients were randomly assigned to two groups over a 4 year period. Exclusion criteria included: recent RRT, a renal transplant within the preceding year, advanced CKD, an overdose necessitating RRT, or a strong suspicion of obstruction or autoimmune/vascular cause of their AKI.
Groups:
Outcomes/Results:
Take home points:
Ketamine In the Critically Ill Patient
Another week, another COVID-19 study...
On August 12th, the Metcovid study was e-published ahead of print in Clinical Infectious Diseases. This was another study looking at steroids in COVID-19 pneumonia, this time performed in Brazil. Metcovid was a parallel, double-blind, randomized, placebo-controlled phase IIb clinical trial which enrolled 416 patients at a single academic center for the evaluation of methylprednisolone (MP; 0.5 mg/kg BID x 5 days) vs placebo. As with all COVID studies, Metcovid has some significant limitations, and some equivocal findings. However, Metcovid was largely in line with RECOVERY and other trials looking at steroids in COVID-19, which lends it some face validity. Metcovid found no significant difference in the primary outcome (mortality at day 28), but did find a difference in mortality in patients over 60 years old (a post-hoc analysis). Metcovid was probably underpowered (sample size was based on a 50% reduction in mortality), and did have a very small trend towards reduced mortality in the MP group (37.1% vs 38.2%, p=0.629).
Bottom Line:
Prior to this study, a Cochrane review and meta-analysis of TXA for upper GI bleeds with 7 trials (1654 patients), showed a large reduction in mortality with TXA (RR 0.61, 95% CI 0.42-0.98, p=0.01)
Design:
-Randomized, international, multicentre, placebo-controlled trial at 164 hospitals in 15 countries Juy 2013-2019
->16/18 years old with upper or lower GI bleeding
-1 g TXA IV over 10 minutes followed by maintenance dose 3 g TXA over 24 hours
Results:
-Main outcome death due to bleeding within 5 days
-4% (222/5994) died in TXA group vs 4% (226/5981) placebo risk ratio RR 0.99, 95% CI 0.82-1.18
-Arterial thromboembolic events MI/CVA similar in both groups (0.7% vs 0.8%)
-Venous thromboembolic events PE/DVT higher in TXA group (0.8% vs 0.4%)
Pitfalls:
-Initially calculated all cause mortality until realization that over half deaths were due to non-bleeding causes, changed to death related to bleeding, allowing study appropriate power to detect difference
-Majority of patients had UGIB/variceal bleeding due to liver disease, over 75% deaths in those with liver disease
-Only 16% patients randomized in <3 hours, most >8 hours (CRASH-2 trial found benefit TXA in trauma patients only <3 hrs to administration)
Takeaway:
-TXA should not be used in the management of GI bleeds
-Increased venous thromboembolic events associated with TXA administration for GI bleeds
Patient
Single Center, double-blinded, randomized trial.
Patients with cancer and septic shock
Intervention
4% albumin + lactate ringer bolus in 10 minutes
180 patients
Comparison:
Lactate ringer bolus in 10 minutes
180 patients
Outcome:
Primary: Any mortality within 7 days of randomization.
Secondary: Mortality within 28 days, renal replacement therapy (RRT)
Results:
7-day mortality: 46 (25%) for LR + albumin vs. 40 (22%) for LR only
28-day mortality: 96 (53%) for LR + albumin vs. 83 (46%) for LR only
RRT: 16 (9%) for LR + albumin vs. 12 (7) for LR only
Conclusion:
Adding albumin for early resuscitation to crystalloids did not improve mortality in cancer patients with septic shock.
Design
-Two-center prospective observational study with 157 patients admitted to the ICU for pneumonia and being treated with HFNC
-ROX (Respiratory rate-OXygenation) index = ratio of SpO2/FIO2 to RR
Results:
-ROX index ≥4.88 at 12 hours after HFNC onset with a sensitivity of 70.1%, a specificity of 72.4%, PPV of 89.4%, NPV of 42%, LR+ of 2.54, and LR- of 0.41 in predicting treatment failure
Validation study: Roca, 2019
-results similar, but ROX index ≥4.88 at 12 hour with LR+ of only 1.82
-also found that a ROX index of <3.85 at 12 hours had a sensitivity of 23.5%, specificity of 98.4%, PPV of 88.9, NPV 69.9, LR+ of 14.47, and LR- 0.78
Pitfalls:
-decision to intubate was not made based on ROX index
-criteria for intubation was also part of the ROX index
-NIV was not part of their treatment algorithm
-created and validated prior to current COVID-19 pandemic
Takeaways:
- The ROX index can be a tool to help predict whether a patient with pneumonia on HFNC may need mechanical ventilation or higher level of care
- May be most helpful with patients with pneumonia on HFNC boarding in the ED
- At 12 hours of HFNC, ROX index of >4.88 suggests patient likely to succeed with HFNC vs. <3.85 which suggests likely need for mechanical ventilation
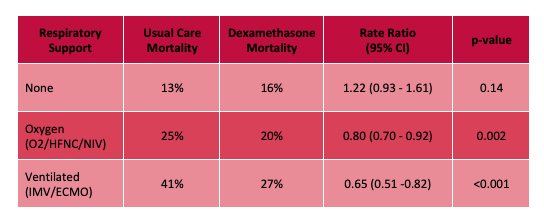
The RECOVERY (Randomized Evaluation of COVid-19 thERapY) investigators recently published a non-peer reviewed article on their findings utilizing dexamethasone to treat patients with COVID-19.
Rx: Dexamethasone 6mg daily* x 10 days (PO or IV) *or steroid equivalent
Primary outcome: All-cause mortality at 28-days
Secondary outcomes:
Results:
Limitations:
Bottom Line: Strongly consider admininstering dexamethasone to your patients with known COVID-19 who require respiratory support, and look for the peer-reviewed publication from the RECOVERY Trial investigators.
We all know the frustration that comes with the phone call from radiology asking if you “really want IV contrast” for your patient’s CT because the creatinine is elevated…
Recently, a joint statement was published between the American College of Radiology and the National Kidney Foundation regarding the safety of IV contrast in patients with kidney disease. The recommendations are based on GFR and apply to those with both chronic kidney disease as well as those who have an acute kidney injury. Summary points of the statement are below:
Every decision to use contrast should be made based on clinical need for contrast as well as individual patient risk factors and underlying disease processes.
As has been previously noted, the white blood cell count is "the last refuge of the intellectually destitute." However, within a CBC (especially if a differential is obtained), there is information that can sometimes be of value. One measure, which was noted before COVID but has come under increasing attention in the current pandemic, is the Neutrophil-To-Lypmhocyte Ratio (NLR). Because physiologic stress typically causes the Absolute Neutrophil Count (ANC) to increase and the Absolute Lymphocyte Count (ALC) to decrease, the ratio of the two values (NLR = ANC/ALC) should increase when the body is under stress. Similar to the WBC however, it should be noted that ANY source of physiologic stress can cause abnormalities of the NLR, and thus this is not limited strictly to infectious etiologies.
With that caveat in mind, the NLR can sometimes be a clue to the degree of physiologic stress the patient is under. As lymphopenia is a frequent finding in COVID, the NLR has come under particular interest in the setting of COVID and appears to have prognostic value in COVID+ patients.
It should be kept in mind that inflammatory stressors (e.g. sepsis) are likely to disproportionately raise the NLR relative to noninflammatory stressors (e.g. pulmonary embolism), so a septic patient with an NLR of 10 might not be all that ill, whereas a PE patient with an NLR of 10 may be sicker. As with any single lab, and particularly one so nonspecific, there are no hard and fast cutoffs, and the NLR has to be interpreted in the context of other clinical data (it is very much possible to have a high NLR and not be that sick, or to have a low NLR and be sick... this is only one datapoint and does have pitfalls associated with it). As a rough guide however, a Pulmcrit post by Josh Farkas from 2019 suggested the following interpretation of the NLR:
1-3: Normal
6-9: Mild stress (e.g. uncomplicated appendicitis)
9-18: Moderate stress, may be associated with critical illness
>18: Severe stress, commonly associated with critical illness
The post (see references below) provides an excellent overview of NLR, further information on the uses and pitfalls of NLR, and several additional sources on the subject. It's a very worthwhile read.
Bottom Line: The Neutrophil-To-Lymphocyte Ratio (NLR = ANC/ALC) is one indicator of the degree of physiologic stress, and may be used in conjuction with other clues to determine how sick your patient is.
Mortality is high in intracranial hemorrhage, and even higher for anti-platelet associated ICH (AP-ICH). The Platelet Transfusion Versus Standard Care After Acute Stroke Due to Spontaneous Cerebral Hemorrhage Associated with Antiplatelet Therapy (PATCH) trial was shocking: it demonstrated platelet transfusion was associated with worse outcomes, excluding those patients who were planned to go to surgery in the next 24 hours. SCCM and the Neurocritical Care Society recommend AGAINST platelet transfusion in non-operative ICH, but encourage a dose of DDAVP.
But who knows who will go to surgery? If you've been giving platelets and DDAVP to non-operative AP-ICH, you're not alone. So in the July Issue of Crit Care Medicine, the authors of the PATCH trial published a retrospective study of 140 patients, excluding those who immediately had surgery. In this group in which a quarter eventually had decompressive craniectomy and a fifth had an external ventricular drain placed, half received platelets and DDAVP instead of DDAVP alone.
The result? Still no benefit to platelet transfusion (despite the inclusion of patients who went on to have surgery). We all WANT to give platelets to AP-ICH, but there is NO evidence of BENEFIT and we may cause HARM. A test of platelet function (like the TEG) should be performed at the very least to select for patients with actual platelet dysfunction, and transfusion should be limited to patients going to surgery.
Analgesics & Sedatives in the Critically Ill Obese Patient
Patient
· A North America multicenter study involving 821 asymptomatic patients who had exposure to Covid-19-positive patients. The study was double-blind, placebo-controlled randomized trial.
Intervention
· Within 4 days of exposure, participants were randomized to receive hydroxychloroquine. Dose of hydroxychloroquine was 800 mg once then 600 mg in 6-8 hours then 600 mg daily for 4 more days.
· There were 414 patients in this arm. Median age 41 years [IQR 33-51]
Comparison:
· Placebo treatment. There were 407 patients in this arm. Median age 40years [IQR 32-50]
Outcome:
· Incidence of either laboratory-confirmed Covid-19 or Covid-19 symptoms within 14 days.
Results:
· 49 (11.8%) patients with treatment had Covid-19 findings (positive tests or symptoms)
· 58 (14.3%) patients with placebo had Covid-19 findings (p=0.35).
· The absolute difference was -2.4%. The number need to treat (NNT) to prevent one infection is 42 patients. Number needed to harm is 50 patients.
· Symptoms were fatigue (49.5%), cough (44.9%), sore throat (40.2%) myalgia (37.4%), fever (34.6%), anosmia (23.4%), shortness of breath (18.7%).
Conclusion:
Hydroxychloroquine prophylaxis did not prevent post-exposure Covid-19 infection.
Clinical Question: Will resuscitation guided by dynamic assessments of fluid responsiveness in patients with septic shock improve patient outcomes?
Methodology:
Design: Randomized, unblinded clinical trial among adults with sepsis-associated hypotension comparing PLR-guided SV responsiveness as a guide for fluid management (intervention) versus “usual care” at 13 hospitals in the United States and the United Kingdom (randomization was in a 2:1 allocation of SV-guided to usual care).
Inclusion criteria:
-patients presenting to the ED with sepsis or septic shock and anticipated ICU admission.
-refractory hypotension (MAP ≤ 65mmHg after receiving ≥ 1L and < 3L of fluid)
Exclusion criteria:
-infusion of > 3L of IV fluid prior to randomization
-hemodynamic instability due to active hemorrhage
-pregnancy or being incarcerated
-indication for immediate surgery
-acute CVA, acute coronary syndrome, acute pulmonary edema, status asthmaticus, major cardiac arrhythmia, drug overdose, injury from burn or trauma, status epilepticus
-inability or contraindication to passive leg raising
Intervention (in ICU):
-PLRs were performed prior to any treatment of hypoperfusion with either fluid bolus or vasopressors for the first 72 hours after ICU admission or until ICU discharge (whichever occurred first)
-If patient was FR (increase in SV ≥10%) a 500 ml crystalloid fluid bolus was given with repeat PLRs after every fluid bolus
-If the patient was non-FR, initiation or up-titration of vasopressors was prompted with repeat PLRs after significant escalation (an increase of 1 mcg/kg/min norepinephrine)
Results:
-83 patients in Intervention arm, 41 in Usual Care arm
-Both arms received a similar volume of resuscitation fluid prior to enrollment (2.4 ± 0.6 L Intervention vs. 2.2 ± 0.7L Usual Care)
-Positive fluid balance at 72 hours or ICU discharge, was significantly less in the Intervention arm (-1.37L favoring Intervention, 0.65 ± 2.85L Median: 0.53L Intervention vs. 2.02 ± 3.44L Median: 1.22L Usual Care, p=0.02).
-Fewer patients required RRT (5.1% vs 17.5%, p=0.04) or MV in Intervention arm compared to Usual Care (17.7% vs 34.1%, p=0.04)
-ICU length of stay was similar in the two arms
-There was no difference in overall 30-day mortality (6.3% difference, Intervention: 15.7% vs. Usual Care: 22.0%, 95% CI -21.2%, 8.6%)
Implications:
Although this is a smaller, unblinded (also funded by maker of SV monitoring device) study, Douglas et al. demonstrate that limiting fluid administration using dynamic assessments of fluid responsiveness to guide resuscitation in patients in septic shock is likely safe. In fact, this may actually decrease the need for renal replacement therapy and mechanical ventilation amongst this patient population. At the very least, this study adds to the body of literature showing the harms of excessive fluid administration and positive fluid balance.
Bottom line:
If possible, use dynamic assessments of fluid responsiveness in patients with septic shock to guide interventions, particularly for further resuscitation beyond initial fluid resuscitation (~2 liters in this study).
As the debate regarding the pathophysiology and ventilator mechanics of COVID pneumonia rages on, it is important to have a method to evaluate the distensibility of patients' lungs so that we can minimize lung injury. It has been well shown that both under- and over-distention lead to acute lung injury and inducing or worsening ARDS.
One method to find the "best" level of PEEP is through the PEEP titration test (also called a Driving Pressure titration test). High Driving Pressure (DP), which is equal to Plateau Pressure - PEEP, has been shown to be associated with lung injury, and the minimal DP obtainable for a given patient while still meeting ventilatory goals is often an objective in the ICU (common DP goal is < 15 cm H2O). A PEEP titration is optimally done on paralyzed patients, although it can be used on sedated or very calm patients as a "best guess" approximation. It will not work well on agitated patients or those participating heavily in their ventilation. Be sure not to do this if you are not authorized to make vent changes, and always make sure to coordinate appropriately with your RT.
To perform a PEEP titration:
*Consider placing the patient on square waveform VC, as this will also allow evaluation of stress index (if patient is not participating). This can be skipped if not evaluating stress index
1) Make a table for yourself on a piece of paper where you can record PEEP, Plateau Pressure, Driving Pressure, Blood Pressure, and SpO2.
2) Write down the initial PEEP, BP, and SpO2. Clearly document for yourself that this is the initial PEEP, so you do not inadvertantly leave the vent on different settings at the end. Perform an inspiratory hold to measure a plateau pressure. Fill in DP by using the equation DP = Pplat - PEEP
3) Change the PEEP. You can either increase or decrease. If you have a suspicion that the patient is over or under distended, go towards optimal distention, but if unsure it is ok to guess. Usually we go by increments of 2 cm H2O. Wait about 20-30 seconds on the new PEEP.
4) Measure a new plateau pressure and calculate a new DP. At each step, write down the BP and SpO2 as well to ensure you are not generating decreased cardiac preload or derecruitment/hypoxia (keep in mind that due to pulse ox lag, you may not see hypoxia for up to a few minutes).
5) Repeat at a few different PEEP levels. Typically in more unstable patients who may not tolerate aggressive vent changes you may only want to check 2-3 levels of PEEP. In more stable patients or if concern for ongoing lung injury is high, you might check up to 5-6 different levels of PEEP. Please note that some COVID ARDS patients are so unstable that they will not tolerate any derecruitment, and this manuever should not be used in those patients as they could desaturate during the titration.
Once you have all of your data, consider changing to whichever PEEP level gives the lowest driving pressure. Keep in mind that while data from a PEEP titration can be very useful, it is only one data point and should be considered in combination with blood pressure, volume status, CXR findings, habitus, FiO2 weaning, and other factors. PEEP titrations should be reperformed periodically (usually daily in most semi-stable ICU patients, more often in unstable patients). it is also recommended to write a note in the chart with your initial vent settings, data from the titration, and settings upon termination of the titration -- and call your RT if you changed the vent settings.
Bottom Line: PEEP titration (aka Driving Pressure titration) aims to identify the PEEP level where (PPlat - PEEP) is minimal and may help reduce risk of ongoing lung injury in ventilated patients.
If you have an intuition your patients older than 65 are at increased risk of infection, especially pneumonia (4-11 times the risk of the under 65 cohorts), you are correct.
If you are concerned your patients co-morbidities, such as COPD, heart disease, and malnutrition will contribute to prolonged mechanical ventilation (the rate of VAP increases 1-3% every extra day on the vent), you are correct.
After age 70, the ICU length of stay and duration of mechanical ventilation increase by 5 days and 9 days respectively.
In the age of COVID-19, itself associated with prolonged mechanical ventilation, it's fair to prepare patients and families for this. We are fortunate we do not need to ration ventilators, so our discussions remain centered on the wishes of our patients, informed by a realistic understanding of what treatment and recovery entail.
Vitamin C for Septic Shock?
Title: Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus
Settings:
Patients:
Intervention:
Comparison:
Outcome: absence of clinical seizure at 60 minutes after infusion of medication.
Study Results:
Discussion:
Conclusion:
Clinical Question: Does a lower MAP target (60-65 mmHg) for ICU patients ≥ 65 years-old reduce 90-day mortality?
Methodology:
-Design: multicenter (across 65 UK ICUs), randomized clinical trial (not blinded), ultimately with 2598 patients
-Inclusion criteria: ICU patients ≥ 65 years-old receiving vasopressors for vasodilatory hypotension with adequate fluid resuscitation
-Exclusion criteria: vasopressors being solely used for bleeding or acute RV/LV failure or post-cardiopulmonary bypass vasoplegia, ongoing treatment for brain/spinal cord injury, death perceived as imminent
-Intervention:
Results:
-Patients in the permissive hypotension group had a lower exposure to vasopressors compared with those in the usual care group
-Mean MAP was on average 6 mmHg lower in permissive hypotension group
-At 90 days, there was no statistically significant difference in all-cause mortality
-No significant difference in mean duration of ICU and hospital stay, duration and days alive and free from advanced respiratory and renal support to day 28
-No significant different in number of serious adverse events (severe acute renal failure, supraventricular and ventricular cardiac arrhythmia, myocardial injury, mesenteric ischemia, and cardiac arrest)
Bottom line:
A lower MAP goal of 60-65 mm Hg appears to be safe for ICU patients ≥ 65 years-old being treated for vasodilatory hypotension
There is currently a high, and appropriate, concern regarding the aerosolization of viral particles during various methods of respiratory support. While studies are limited, here is some of the currently available data (mostly-simulated) on the approximate maximum distances of particle spread:
Nasal Cannula 5LPM:1 1 ft 4.5 in
Non-Rebreather Mask, 6-12LPM: 4 in, minimal change with increasing flows1
High Flow Nasal Cannula
CPAP (20 cmH2O) provided by oronasal mask with good fit (leak from exhaust port):2 11.5 in
Bilevel positive airway pressure w/ oronasal mask (IPAP 10-18/EPAP 4): max dispersal:4 1 ft 7.7 in
Bilevel positive airway pressure with full facemask5 (IPAP 18 / EPAP 5): 2 ft 8 in
Bilevel positive airway pressure with helmet:4
Utility of Surgical Mask:6
Bottom Line:
In vivo data from actual patients is lacking, however there is potentially lower risk of aerosol spread with HFNC than regular nasal cannula, perhaps due to higher likelihood of a tighter nare/nasal cannula interface. Nonrebreather mask performs well indirectly with the shortest dispersal distance. Noninvasive positive pressure ventilation with an oronasal mask and good seal has a relatively short dispersal distance, and a surgical mask over respiratory support interventions actively decreases amount, if not distance, of particle spread. Use of appropriate PPE and negative pressure rooms, if available, remains key.
Please see Part I from 12/24/19 for information about causes and symptoms.
Diagnosis:
The diagnosis of HLH is challenging, as it often mimics sepsis or other critical illness. A high index of suspicion is vital and early treatment, imperative.
Diagnostic criteria in adults include 5 of 8 of the following:
(based on the Hscore: https://www.mdcalc.com/hscore-reactive-hemophagocytic-syndrome#use-cases)
· Presence of known immunosuppression
· Fever >38.5
· Splenomegaly or hepatomegaly
· Cytopenias
· Ferritin elevation (usually markedly elevated)
· Elevated triglycerides
· Low fibrinogen level
· ALT elevation
Immunologic testing:
· CD25 levels are elevated
· NK cell activity is low or absent
In adults, highly elevated ferritin levels (>10,000) are highly suggestive of HLH.
Elevated LDH, Ddimer, and multisystem organ dysfunction (especially CNS) is common.
Immunologic testing should not delay treatment if other lab values suggestive of HLH.
Treatment:
Given the high mortality rate, treatment should be initiated if the symptoms are suggestive of HLH. In the setting of a critically ill individual, hematology consultation is warranted for treatment guidance as treatment is based on lab values and clinical picture. Treatment usually starts with high dose , IV steroids (dexamethasone) and may include chemotherapeutic agents, such as Etoposide. For those patients with CNS involvement, intrathecal chemotherapy is usually a mainstay of treatment