When you think of an acid or base causing a burn, you usually think of the local damage but there is one particular acid that causes systemic illness. Hydrofluoric Acid, found in your local Home Depot in brick/stone cleaning products, can cause severe illness despite a small total body surface area burn and exposure. A recent case report came out that illustrates how deadly HF can be. The reason is that this acid enters the body and chelates cations like calcium and potassium. The abstract is below but essentially hypocalcemia, hypokalemia leading to asystole 16hrs after exposure all from a 3% TBSA Burn - very impressive.
The answer was fomepizole would be the treatment for life-threatening disulfiram reaction. Blocks Alcohol Dehydrogenase and ironically prevent metabolism of ethanol and prolong intoxication.
I forgot how many see the pearls and the response was overwhelming. That was great and cost a me a little more. There were two winners:
Katie Baugher, PGY-1
Ari Keslter
Please email me how to best send you the gift certificate.
There are medications, if taken with ethanol, will cause a disulfiram reaction. This reaction results from inhibition of aldehyde dehydrogenase, the enzyme in ethanol metabolism that breaks acetaldehyde to acetic acid. The increase in acetaldehyde results in nausea, vomiting, diarrhea, flushing, palpitations and orthostatic hypotension. So if you prescribe a patient with any of these medications you must make certain to tell them NOT to drink any ethanol - that includes cough/cold preparations that have ethanol:
Antibiotics: Metronidazole(Flagyl), Trimethoprim-sulfamethoxazole (Bactrim)
Sulfonylureas: Chlorpropamide and tolbutamide
These have possible reactions: griseofulvin, quinacrine, procarbazine, phentolamine, nitrofurantoin
Bonus Question: $10 Starbuck's Gift Card for first person that emails me with the answer to this question
What treatment could you give to someone suffering from a life threatening disulfiram reaction that biochemically should cure him?
As we eat our turkey today and the myth that we are tired because of the tryptophan content is propagated further - nothing to do with the 2000kcals that we just ate - I would like to share an interesting and controversial study.
Use of stimulants and and sedatives by EM residents. Incidence is as follows:
In a study of 485 residents with 47% response rate:
Prescription Stimulants: 3.1%
Sleep Aids (all): 89%
Use of Nonbenzodiazepines (zolpidem): 14%
Use of Melatonin: 10%
Benzodiazepines: 9%
Difficult job with difficult hours. What is the appropriate medication or is there a medication that truly assists with performance? Are they doing harm to themselves? to patients?
Disrupted circadian rhythm, addiction tendencies and the hardship of a stressful nightshifts are the price we pay for this specialty. Awareness and education are needed for the residents as well as the attendings.
In the setting of a patient suffering from an anticholinergic overdose with hallucinations/agitation, it may be beneficial to administer the antidote: Physostigmine. Many hesitate simply because they have never administered before or there may be doubt in the diagnosis. Here is the skinny:
1) Anticholinergic OD seen in following meds: diphenhydramine (Benadryl), dimenhydrinate (Dramamine), scopolamine, benztropine (Cogentin), some plants like datura stromonium (thorn apple)
2) Physostigmine 1mg IV slowly over a REAL 5 min. Administer to fast and patient may seize. Maximum dose of 2mg IV.
3) Contraindications: suspicion of TCA OD (anectdotal and from old case report) - screening EKG should be done prior to administration of physostigmine. Also glaucoma, closed angle, obstructive uropathy.
Remember your clinical endpoint needs to be measurable, thus hallucinations and agitation should be reversed. No indication if the patient is only experiencing dry mouth or other more mild anticholinergic symptoms.
When a patient presents to the ED with a recent ingestion of a wild mushroom there are three very specific questions you must ask:
1) Exactly what time did you eat the mushroom?
2) Exactly what time did you begin vomiting/diarrhea/GI Sx in general?
3) Are there are more mushrooms that can be brought to ED for identification?
The reason the first two questions are critically important is it determines the total time of onset of toxicity. As a very general rule of thumb, delayed GI symptoms >6hrs is predictive of a possible lethal ingestion of a cyclopeptide containing mushroom like Amanita Phalloides. Immediate symptoms < 6hrs and even more so if within 2 hrs usually indicates ingestion of a nonlethal mushroom that causes GI distress (many mushrooms like Clitocybe nebularis)
Website with pics of the most poisonous mushrooms:
http://scienceray.com/biology/botany/13-deadliest-mushrooms-on-the-planet/
There is a saying:
"There are old mushroom pickers and wise mushroom pickers but no old and wise mushroom pickers"
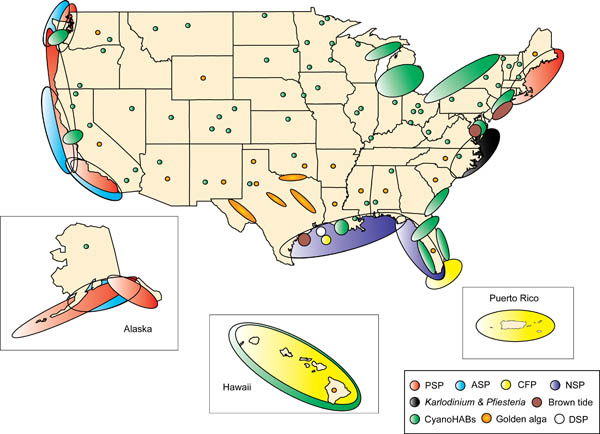
Although we may not be able to eat as much shellfish after the oil spill, there are still some left that can cause some interesting toxicity here in the USA. Shellfish act as vectors for the bacteria, virus etc that produces toxin thus not specific to one species of shellfish. There is a map attached that shows where shellfish poisoning occurs most. In the picture CFP=ciguatera, PSP=Paralytic and ASP=AmnesticC. Surprising the distribution and it will be interesting how the oil spill affects the distribution. Treatment for all of these is supportive with no known antidote and incidence increases during Red Tide months:
A fentanyl patch contains 100-fold more fentanyl in the reservoir than what is posted on the patch. For instance, 100mcg/hr patch will have over 10mg - thats milligrams - of fentanyl. This provides a rather large source for potential abuse. Overdose and deaths have occurred by patients in the following ways:
It is the many
In a previous pearl we were discussing the need to perform EGD for any suicidal patient with a history of ingestion of a caustic to grade injury and assess chance of perforation and/or stricture formation. Suicidal patients are intentionally ingesting the caustic and can thus justify the risk/benefit ratio more easily than the pediatric unintentional ingestion. The concerned parent will bring the child in with a possible ingestion of a caustic. The container could be simply in the same room, spilled on the child and never be ingested. Even if ingested, the amount is less if the child tastes the caustic and will reflexively cause spitting. The literature is scant in regards to this type of patient but seems to point to this general algorithm:
Child displays 2 or more of the following symptoms there is enough evidence from case series that there will be a clinically signficant lesion found on EGD.
Vomiting, Drooling, Stridor, Presence of Oropharyngeal Burns
That being said, many clinicians would elect for EGD and assessment of airway with stridor alone. Do not be fooled into thinking if you see no oral lesions that there is no way the child ingested the caustic. Each case series showed a lack of correlation of physical exam findings to EGD findings.
We will all get the patient presenting with low blood glucose on a regular basis. In general, barring any underlying infection, those who are insulin dependent can be corrected with IV dextrose and/or food and be discharged. Those on a sulfonylurea may experience repeated hypoglycemic episodes and require admission - perhaps even treatment with the antidote: octreotide.
Below is the duration of action and half-life of the sulfonylureas which illustrates the need for admission:
Duration of action is the physiologic effect whereas the half-life is the pharmacokinetics of elimination of the drug. Often these two numbers are different for drugs. Do not let the half-life fool you into thinking it is safe to discharge a hypoglycemic patient on a sulfonylurea.
Ingestion of caustics can lead to immediate burns to mouth, esophagus, stomach as well as possible perforation. Months and years later, further complications are esophageal stenosis and increased incidence of esophageal carcinoma. The main benefit to EGD is to determine extent of injury within the esophagus. The lesions are graded much like a burn:
Grade I: Mild burn, no risk for esophageal stenosis
Grade II: Moderate, if circumferential, patient is at risk for esophageal stenosis
Grade II: Eschar present, high risk of perforation as well as esophagel stenosis
You can make a case that all intentional-suicidal ingestions of caustics should undergo EGD since there should be some injury if ingestion truly occurred or at the least a higher probability. The difficult case is the pediatric unintentional ingestion. Utilizing clinical exam and history will assist with that determination - there is a little research to guide this decision (next pearl)
The attached picture is the post-mortem of a caustic injury showing grade II linear lesions in esophagus with eschar distally and in stomach (Grade III).
Valproic Acid (Depakote) is a drug that uniquely has the ability to raise serum ammonia concentrations. It is able to do this without raising liver er enzymes and it can occur in overdose or at therapeutic levels. Do not think of this in the context of hepatic encephalopathy. This a metabolic derangement caused by VPA.
In the state of Maryland, the most common venomous snake is the copperhead. Though not as dangerous as the rattlesnake, it can still cause loss of function of limb and mortality in the pediatric patient.
Treatment has involved the use of CroFab (Protherics, Atlanta). This ovine derived monovalent immunoglobolin is actually made against the following snakes:
Though efficacy has been shown with these snakes, we are hoping for cross-reactivity when we treat copperheads. There are case series and case reports (1) that have shown anectdotal improvement. We are still awaiting a real randomized controlled trial - may never happen.
Scombroid is caused by ingestion of preformed histamine on skin of fish.
Here are is a list of common drugs that will cause thrombocytopenia as a result of antiplatelet antibodies (its not just heparin!). This list is not complete but are common ones that you will see in the ED, coming from USH or on the floors/units during residency:
Abciximab, Acetaminophen, amiodarone, amphotericin B, ASA
Carbamazepine, cimetidine
Digoxin
Methyldopa
Quinidine, Quinine
Rifampin
Trimethoprin-sulfamethoxazole
Vancomycin
Several drugs and compounds may be radiopaque on an abdominal radiograph. This may be helpful in an overdose to determine ingestion or amount ingested. Attached is a pic a patient that ingested potassium sustained release tables.
The mneumonic CHIPES will help you remember which are:
C - Calcium Carbonate, chloral hydrate
H - Heavy metal - like Mercury, lead
I - Iron and Iodine
P - Phenothiazines (compound that has S(C6H4)2NH in it), drugs that include: antipsychotics like chlorpromazine (thorazine) and antiemetics like prochlorperazine (compazine)
E - Enteric coated pills
S - Solvents [halogenated ones like chloroform] and Sustained Release preparations [Lithobid and K-Dur]
When you draw a urine toxicology screen it can mislead more often than help you. Here is a quick list of the test followed by some medications that cause false positives - when in doubt, call your lab to find out specifics since results will vary lab to lab:
TCA - diphenhydramine, carbamazepine, cyclobenzaprine (side note: TCA screen should never be used to determine TCA toxicity, your ECG and physical exam should be enough to determine if the patient is toxic from TCA
Cocaine - the most accurate test on the screen, positive for up to 5 days
PCP - dextromethorphan and ketamine can turn it positive
Amphetamines - pseudoephedrine, ephedrine, phenylephrine and many other OTC cough decongestants can as well, the worst screening test with the largest number of false positives
When a child is reported to be exposed to a rat poison it is commonly a long acting coumarin like brodifacoum. The rat usually eats the poison then during its traumatic little life will cause its own death by jumping and squeezing through a crack. When a human is exposed, this is the typical sequence of events:
Treatment is the same as for coumadin, vitamin K. However, do not start empirically since the patient will be committed to high doses of vitamin K for several months. Let the patient prove they have been poisoned which means they will require recheck of their INR 2-3 days later though they can be sent home with specific warning signs of anticoagulation.