Popliteal artery injuries are very rare (4% of all vascular injuries).
The majority of injuries are secondary to penetrating injury (70+%)
Blunt mechanism of injury has the higher rate of amputation.
Prolonged ischemia time (from injury to repair greater than 6 hours) leads to higher rates of amputation
Hard signs of vascular injury should prompt X-ray imaging of the knee, femur, and lower extremity and transfer to an operating room for repair.
Soft signs ("a history of significant bleeding which has ceased, nonexpanding hematomas, and the presence of an Ankle-Brachial Index of less than 0.9") and shotgun injury should prompt CT angiogram to evaluate arterial injury.
In a metanalysis of studies looking at intercranial hemorrhage in fall patients older than 65 years, the following were unadjusted odds ratio risk factors for finding an ICH in this patient population:
suspected open or depressed skull fracture , signs of basal skull fracture ), reduced baseline Glasgow Coma Scale score , focal neurologic signs , seizure , vomiting , amnesia , loss of consciousness , headache ), external sign of head trauma , male sex , chronic kidney disease , preinjury single antiplatelet , and dual antiplatelet medication .
Preinjury anticoagulant was not a significant risk factor.
When looking at adjusted odds rations only focal neurologic signs , external sign of head trauma , loss of consciousness , and male sex were found to be associated with intercranial hemorrhage.
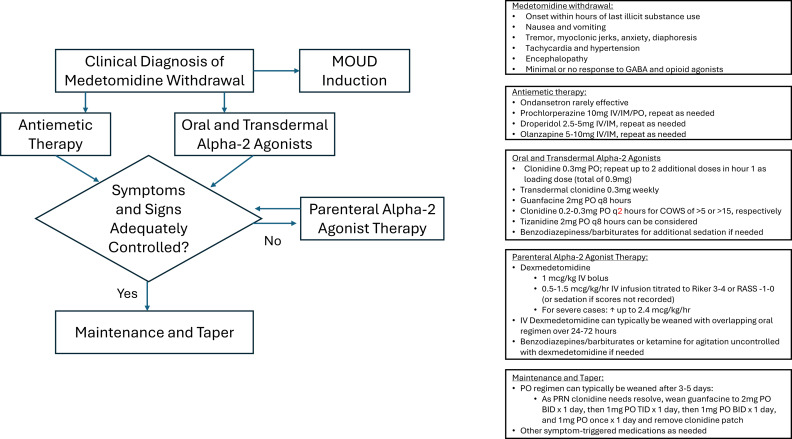
The US drug supply has been found to contain medetomidine as an adulterant to heroine/fentanyl. It is a potent tranquilizer used in animals. It is an alpha 2 blocker (similar pharmacology to clonidine and xylazine). Exposure to this drug can induce withdrawal symptoms to include anxiety, tremor, diaphoresis, nausea, vomiting, agitation, sympathetic hyperactivity, and delirium. Withdrawal can start within 4-6 hours of last use.
Treatment for withdrawal is outlined in this diagram.
An English study describes 30 patients that jumped from a single bridge of 30 meters (98 feet) over the course of 12 years. Twenty six landed in the water. The injury pattern for those landing in water was described as “Hypothermia was the most common presentation (n = 23), followed by pneumothoraces (n = 14), rib fractures (n = 10), thoracic vertebral fractures (n = 9) and lung contusions (n = 8). Lower water temperatures at the time of the incident (p = 0.008) and lower patient body temperatures on arrival to hospital (p = 0.002) were significantly associated with increased 30-day mortality.”
The small group landing on land had more pelvic and extremity fractures than the water group and none had hypothermia.
Remember to start aggressive rewarming in patients who fall into water!
This small study from South Africa shows stab wounds to the chest with a pneumothorax less than 0.5 cm that were managed conservatively had completely resolved on 12 hour repeat chest X-ray. This could facilitate earlier discharge of these patients. It also supports conservative (non-tube placement) approach to asymptomatic small pneumothoraces from stab wounds.
Tramadol has been viewed as a safer alternative for pain control than opioids. This study says differently.
“Tramadol use was associated with increased risk of multiple ER utilizations, falls/fractures, CVD hospitalizations, safety event hospitalizations, and mortality (new users only) compared to nonuse.”
A reminder from a recent position paper on pelvic trauma that we should not be doing stability testing to evaluate pelvic trauma
“EMS clinicians should recognize the challenges in accurately identifying pelvic fractures by physical exam alone. Manual stability testing of the pelvis is neither sensitive nor specific and may cause harm.”
In 261 ED patients over age 65 receiving first generation antihistamines, 15% had an adverse reaction. Most common was delirium and urinary retention. Age over 85, previous cognitive impairment and multiple doses increased the risk of adverse reaction. Along with previous literature, this should discourage use of first generation antihistamines in older ED patients.
In this study reviewing data from the American College of Emergency Physicians’ Emergency Quality Network substance use disorder program, EDs prescribed naloxone in 27% of patients discharged after opioid overdose. Only 7% received ED administered or prescription for buprenorphine, etc. There is a lot of room for improvement in the care we provide for this subset of ED patients.
Much has been written about the benefits of prehospital blood transfusion for traumatic hemorrhage. Can this success be ascribed to non-traumatic hemorrhage as well? This small study (50 patients over 10 years!) says there were improvements in patient physiology (shock index) for those patients receiving blood for GI bleed, etc. Much more research is needed however this could be a beneficial practice in the future.
This systematic review found improved pain scale at 15 and 120 minutes in 495 patients who received nebulized ketamine. Dosing at 0.75 mg/kg was as effective as 1.5 mg/kg and the nebulized ketamine was non-inferior to IV morphine and ketamine with fewer side effects.
The Geriatric Measurement Tool (GMT) was used in this study prospectively to assess 24 hour mortality rate in ED patients over age 65. The GMT is a combination of FRAIL Questionnaire and Barthel index for Activity of Daily Living. The study found:
“ From 700 enrolled patients, GMT categorization revealed that 53.6% of patients were in Category-4 (moderate/more dependent and frail), while 34% were in Category-1 (independent or slight dependency, prefrail/fit). The 24-h mortality rate was 9%. GMT Category-4 demonstrated high sensitivity (87.3%) for mortality prediction, but low specificity (49.7%). Conversely, GMT Category-1 showed low sensitivity (44.1%) but high specificity (90.2%) for predicting discharge.”
Probably the biggest take away is we should be thinking about assessing our older patient's health status using some validated scale/tool to help us have conversations with patients and families regarding prognosis and interventions.
The Geriatric Measurement Tool combines the FRAIL Questionnaire with the Barthel Index For Daily Living to give a prognosis on your patient's mortality. First used to predict mortality in older patients with pneumonia during COVID-19 pandemic. Now being investigated for other ED patient populations.
FRAIL Questionnaire: Fatigue, Resistance, Aerobic, Illness, Weight loss. https://www.activeagingweek.com/pdf/abbott/FRAILQuestionnaire.pdf
Barthel: Ten questions about ADL's to create a score 0-100. https://www.mdcalc.com/calc/3912/barthel-index-activities-daily-living-adl
This study looked at industry sponsored payments to EM physician through non-covered entities (ie not directly to physician or through an academic institution). It found a $100 million increase from 2015-23 in this payment model. It appears that private equity is not the only money entering emergency medicine in the past decade.
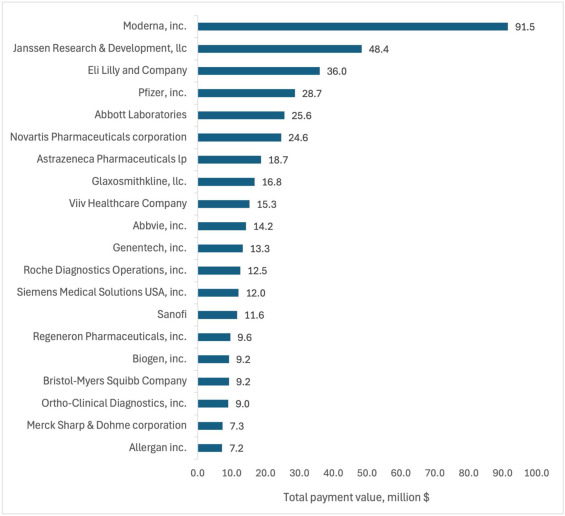
Total value of Industry-Sponsored Research Payments (ISRPs) by company. The 20 companies with highest total ISRPs awarded to emergency physician PIs.
We have all been on that busy shift and just quickly looked at the impression section of the radiology report whether that is a CT, plain film, US or MRI. In doing this you run the risk of missing important information that is contained in the body of the report and has either not been carried down into the impression or contradicts the impression by some error.
To avoid missing important information that can impact patient care, always read the entire report and look at the images yourself. You have seen the patient, know the clinical history, and a second set of eyes never hurts.
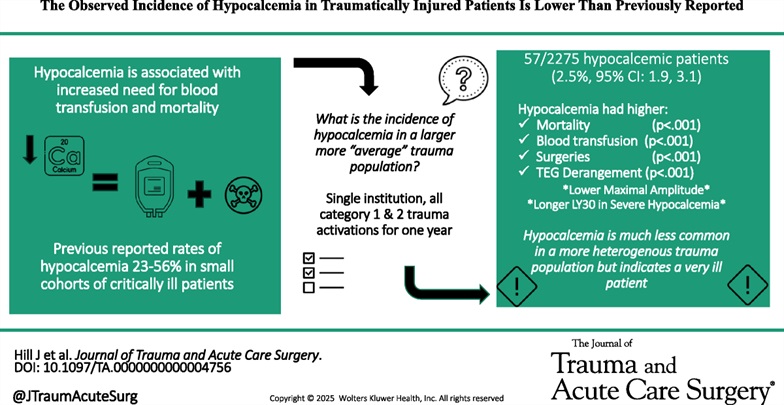
Previous small studies had put the prevalence of hypocalcemia in trauma patients at 23-56%. This single center study of 2200 patients looked at prevalence and outcome and found a much lower prevalence however worse outcomes than those who were not hypocalcemic.
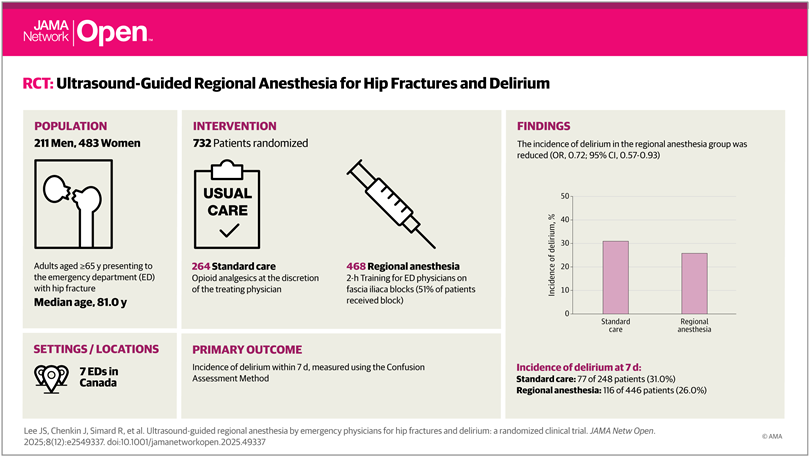
This study is a reminder of the efficacy of regional nerve blocks for older patient's with hip fractures. The authors trained EM physicians for 2 hours then evaluated delirium levels in patients who did and did not receive nerve blocks for hip fractures.
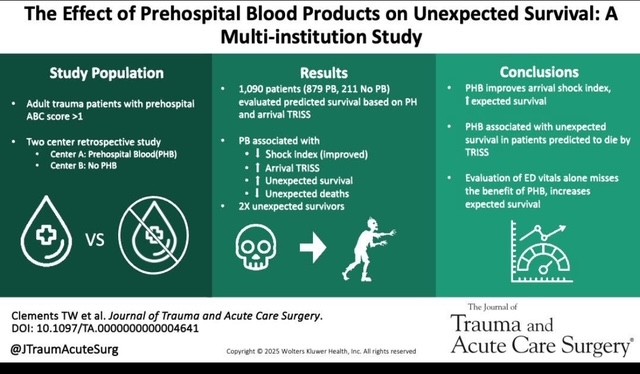
This study demonstrated that administration of prehospital blood to trauma patients lead to a higher rate of survival in patients whose initial ED vital signs or pre-hospital shock index would have predicted death.
This review article reminds us that circulation needs to be prioritized over airway in trauma patients. This means bleeding control (pressure on wound, tourniquet, surgery/IR intervention), correcting tension pneumothorax, correcting pericardial tamponade, as well as resuscitation to return physiologic homeostasis (blood products, vasopressors where needed, warm the patient, etc.) before intubation. Altered mental status/low GCS may be due more to hypoperfusion than neurologic injury. Correcting the hypotension may alleviate that need to intubate.
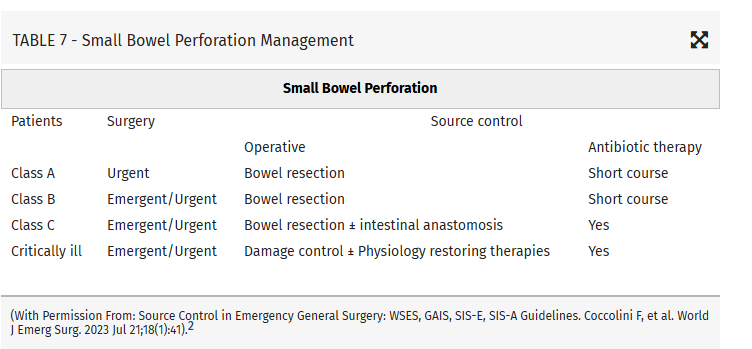
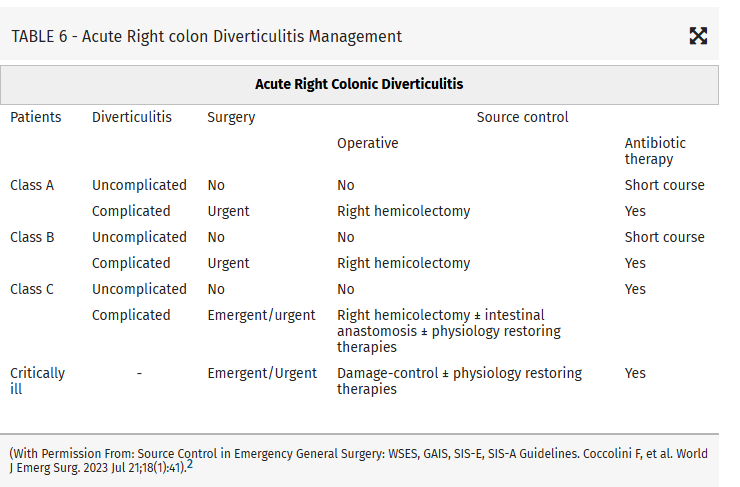
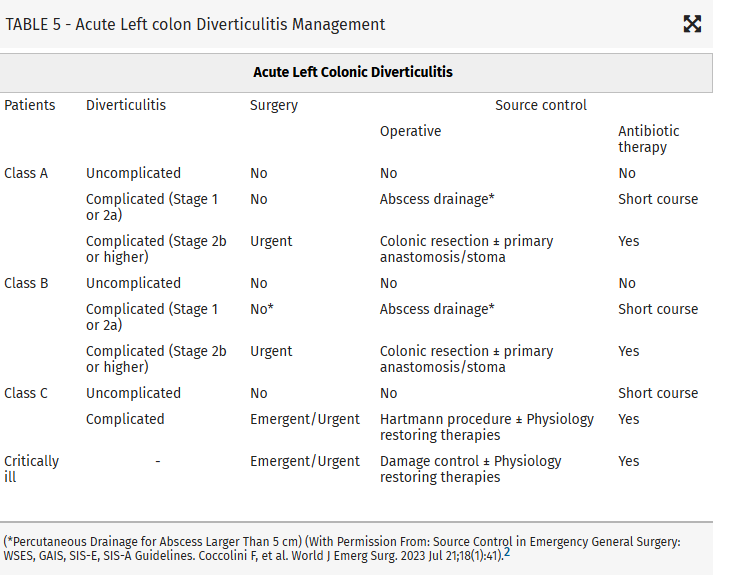
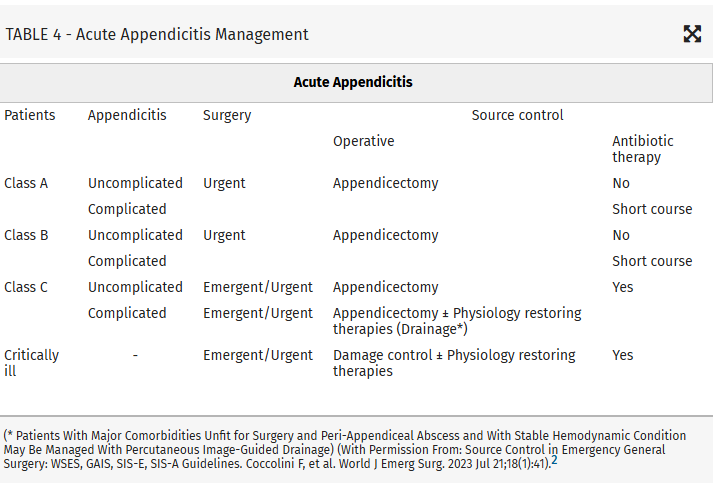
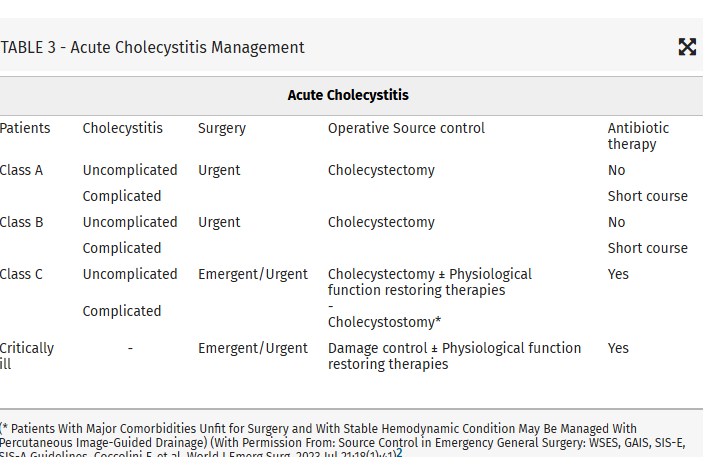
Intraabdominal infections leading to sepsis can come from cholecystitis, small bowel perforation, gastric perforation, left sided colonic diverticulitis, right sided diverticulitis and appendicitis. When to initiate source control and antibiotics is controversial. These authors propose breaking patient populations into three groups:
From this they propose algorithms to treat these intraabdominal infections such as (note the different approach to right and left diverticulitis):